
Abstract

This case was institutional review board exempt according to Temple University protocol. A 58-year-old female with history of recurrent refractory chronic lymphocytic leukemia (CLL) on ibrutinib presented with one week of nasal congestion, rhinorrhea, and anosmia. She failed a trial of Augmentin and Medrol prior to presenting to ENT clinic. Anterior rhinoscopy showed severe bilateral mucosal edema with pallor along the septum and inferior turbinates (Figure 1). Computed tomography (CT) sinus obtained in the emergency department prior to ENT visit showed anterior nasal cavity mucosal thickening and right sphenoid opacification (Figure 2). Complete blood count demonstrated thrombocytopenia and leukopenia with absolute neutrophil count (ANC) of 500. Given the patient’s immunocompromised state and physical examination findings, acute invasive fungal rhinosinusitis (AIFRS) was suspected. The patient was urgently admitted to the hospital, started on intravenous liposomal amphotericin B, transfused platelets, and home ibrutinib discontinued. The patient was taken to the operating room for urgent biopsy and right sphenoidotomy. Frozen section pathology returned no fungal or yeast elements. Final pathology was negative for fungus but was significant for intranuclear inclusions consistent with herpes infection. Immunohistochemical staining was positive for herpes simplex virus (HSV)-1 and -2 and lymphoid infiltrate concerning for refractory CLL. The patient was diagnosed with intranasal herpes and started on oral and topical acyclovir as well as antibiotics for sphenoid sinusitis. The patient’s symptoms and mucosal abnormalities resolved within 2 weeks. After ANC recovered, the treatment of refractory CLL was resumed; however, the patient expired 2 months later from complications of refractory CLL.
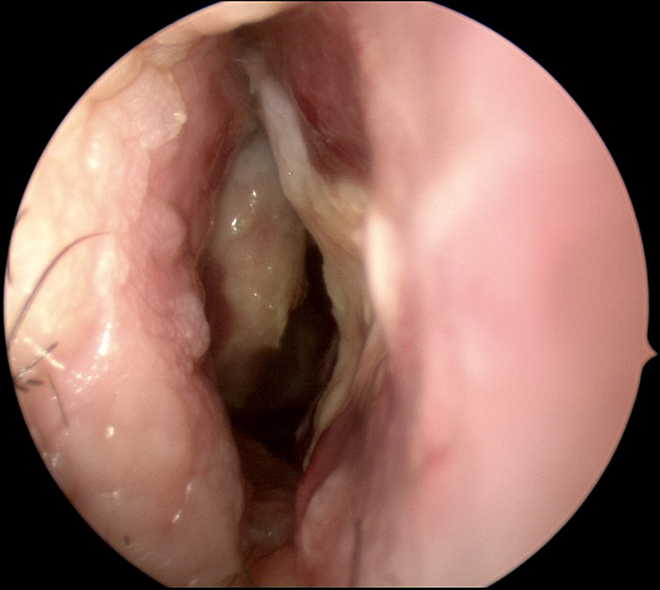
Mucosal edema and pallor along septum and inferior turbinate in right nasal cavity.
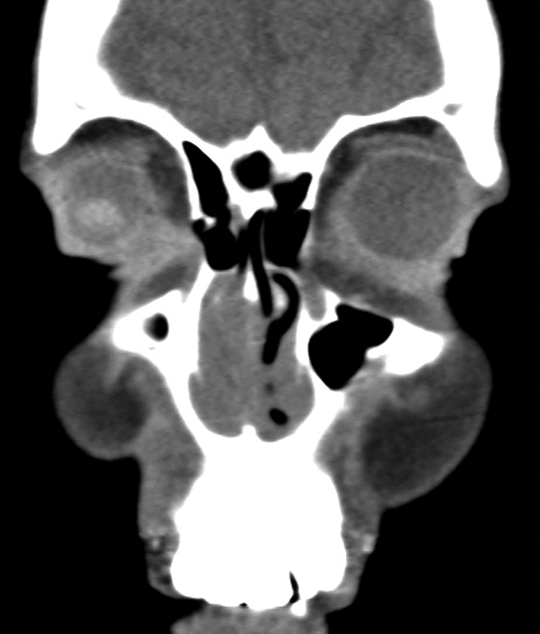
Coronal computed tomography (CT) of sinuses demonstrating right greater than left mucosal thickening.
Acute invasive fungal rhinosinusitis is a rare and often fatal infection that requires early diagnosis and aggressive management. Patients with poorly controlled diabetes and absolute neutropenia (eg, hematologic malignancy like our patient), especially ANC less than 500/μL, are at increased risk. 1 The most common pathogens include Mucor, Rhizopus, and Aspergillus spp. A high index of suspicion should be maintained for AIFRS in immunocompromised patients with sinusitis symptoms. Early symptoms are often nonspecific: facial pain, facial edema, nasal obstruction, and fever. The most common sinus CT finding is intranasal or sinus mucosal thickening. 2 On physical examination, mucosal changes such as pale and black mucosa are the most consistent findings, with ulceration and black mucosa being late findings. Imaging, physical examination, and endoscopy with biopsy are crucial in the workup of AIFRS. Standard treatment includes surgical debridement and antifungal therapy. Once AIFRS has been ruled out, other etiologies should be considered.
Intranasal HSV has not previously been described in the literature. Herpes simplex virus-1 commonly infects and reactivates within the oral mucosa, but infection of the nasal membranes has not been previously documented. Herpes simplex virus is occasionally found to shed from nasal mucosa but has not been found to cause characteristic herpetiform lesions or prodrome. 3 Herpes activations are known to occur in stressful situations, with each reactivation typically becoming less frequent and severe. Reactivation of HSV typically responds well to acyclovir, as in this case, being treated with topical and oral preparations.
The patient presented with CLL following a course of ibrutinib. Some treatments, such as ibrutinib, may further transiently immunocompromise the patient, as in our patient who had worsening neutropenia. 4 Given this presentation, it is critical to maintain a high degree of suspicion for AIFRS. Computed tomography and nasal endoscopy findings were suspicious for AIFRS, necessitating timely frozen section pathology as a rapid means of identifying the presence or absence of fungi in the sinonasal cavity. 5 If fungal elements are excluded, other opportunistic or viral infections may play a role.
As the final pathology included evidence of refractory CLL infiltrating the nasal mucosa, one could argue that CLL caused the nasal symptoms. However, treatment of the intranasal herpes with topical and oral acyclovir resulted in complete symptom resolution. Moreover, during this time, CLL treatment was stopped to allow recovery of the ANC. Therefore, the nasal findings and symptoms can be reasonably attributed to HSV. This unique case, with uncommon reactivation of HSV, sheds light on other opportunistic infections that can affect immunocompromised patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.