
Abstract
Management of laryngotracheal stenosis is challenging and laryngotracheal stenosis is generally managed with laryngotracheal reconstruction. Stents are often used as part of the reconstructive surgery. Although most stents adequately stabilize the reconstruction during healing, they often do a poor job of mimicking glottic anatomy, particularly the anterior glottis. Here, we present a modified suprastomal stent designed to stabilize reconstruction after laryngotracheal reconstruction while also improving postoperative glottic anatomy and function. The case of a 15-year-old tracheostomy-dependent patient with glotto-subglottic stenosis who underwent laryngotracheal reconstruction using this modified stent is described. The patient had an excellent outcome with decannulation of her tracheostomy and significant improvement in voice.
Keywords
Introduction
Laryngotracheal stenosis is a challenging problem faced by otolaryngologist–head and neck surgeons. Glotto-subglottic stenosis is particularly challenging and is associated with delayed and decreased rates of decannulation when compared with isolated subglottic stenosis. 1 Laryngotracheal reconstruction (LTR) has become the surgical standard for repair of laryngotracheal stenosis. 2,3 Stents are frequently used to stabilize and maintain postsurgical patency and caliber of the airway after LTR. 4,5 Many stents are commercially available, but the majority remain rudimentary in form and a poor representation of laryngeal anatomy, particularly in respect to the complex shape of the glottis. We present a modified suprastomal laryngeal stent, designed to improve glottic and subglottic anatomy after LTR.
Methods
Case Report
A 15-year-old female presented after recent emigration from the Dominican Republic with a history of congenital airway stenosis for which she underwent 2 surgeries during infancy. The details of these surgeries are unavailable, but the patient has remained tracheostomy dependent since she was 6 months old.
On initial evaluation, the patient had very poor voice production with rough, breathy, and strained vocalization produced while finger occluding her tracheostomy tube. Fiberoptic laryngeal examination revealed type IV glottic webbing (Cohen’s classification) 6 (Figure 1), a small posterior gap, and normal tracheal anatomy from the distal tracheotomy tube to the carina. The patient was taken to the operating room for direct laryngoscopy and was found to have fusion of the anterior 80% of her vocal cords which extended into the subglottis and a small posterior opening (Figure 2).
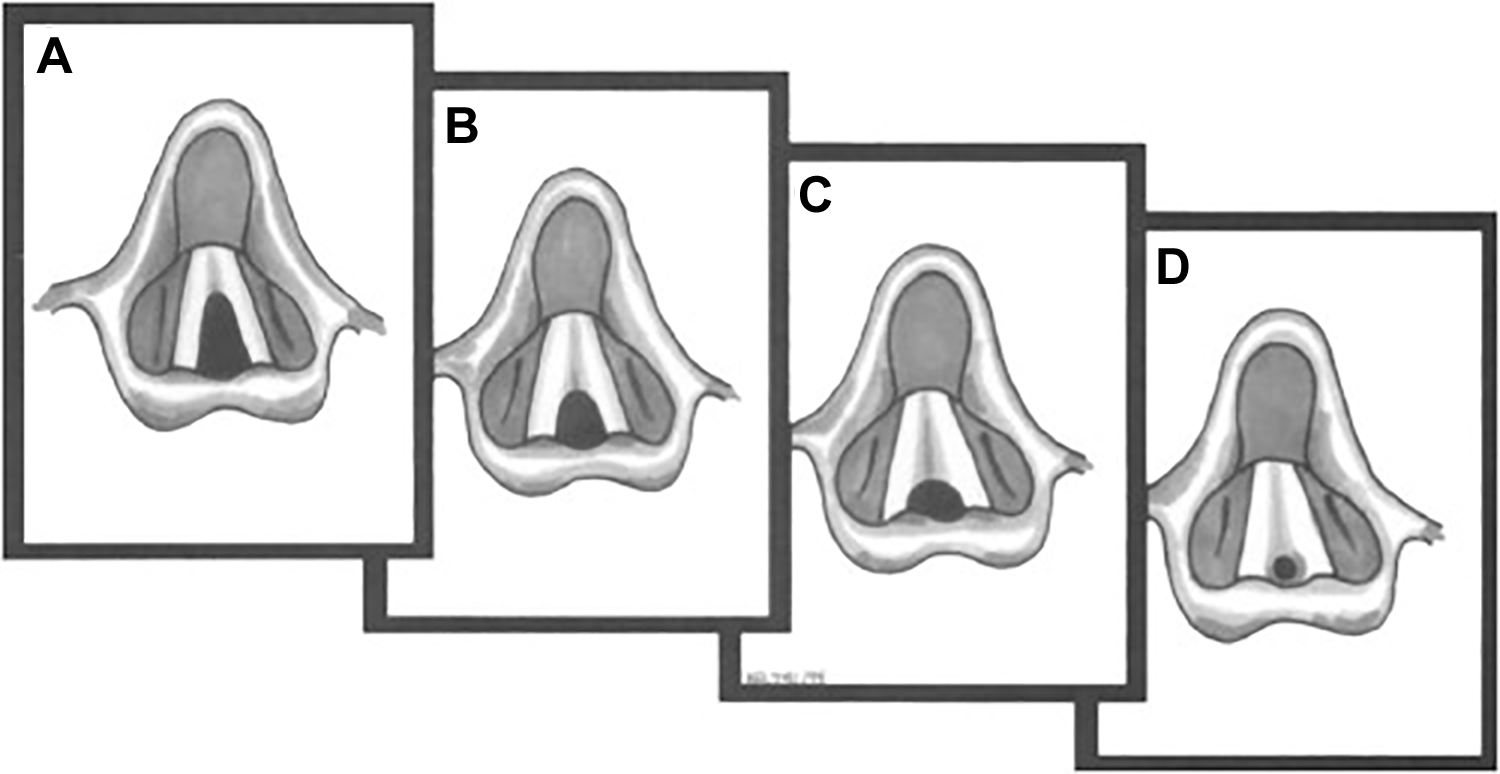
A, Type 1 glottic web. B, Type 2 glottic web. C, Type 3 glottic web. D, Type 4 glottic web. (From Koltai PJ, Mouzakes J. The surgical management of anterior glottic webs. Oper Tech Otolayngol Head Neck Surg. 1999;10(4):326.)

Preoperative fiberoptic examination shows webbing of the anterior 80% of the glottis with a small posterior opening, consistent with a type 4 glottic stenosis.
Surgical Approach
We initially attempted surgical repair with endoscopic lysis of adhesions and silicone keel placement which was complicated by restenosis. The patient was then taken for LTR with cartilage grafting and stenting. Briefly, an incision was made in the skin and dissection was carried down to the anterior laryngeal cartilage. A complete midline laryngeal fissure through the thyroid cartilage and the anterior cricoid ring was performed to adequately divide the anterior glottic webbing and subglottic stenosis. Direct laryngoscopy was concurrently performed by an assistant to guide the laryngofissure through the anterior laryngeal commissure as close as possible to midline. A costal cartilage graft was then harvested in the standard fashion.
An 8-mm silicone stent (Rutter Supra-Stomal Stent) was modified by making a vertical incision at the level of the glottis, placing a silicone sheet in this incision, and suturing the sheet in place. Starting the suture through the incision in the stent allows the knot to be secured inside the lumen of the stent minimizing potential irritation caused by an exposed knot (Figure 3). The modified stent was subsequently placed in the airway with the silicone sheet extending through the anterior commissure and the thyroid cartilage (Figure 4). The proximal end of the stent was in the supraglottis, and the distal end was just above the existing tracheotomy (Figure 5). A costal cartilage graft was subsequently placed inferior to the silicone sheet and secured in the standard fashion. The anterior portion of the silicone sheet was then sutured in place to the thyroid cartilage with the suture buried just beneath the skin. The skin was then closed in the standard fashion.
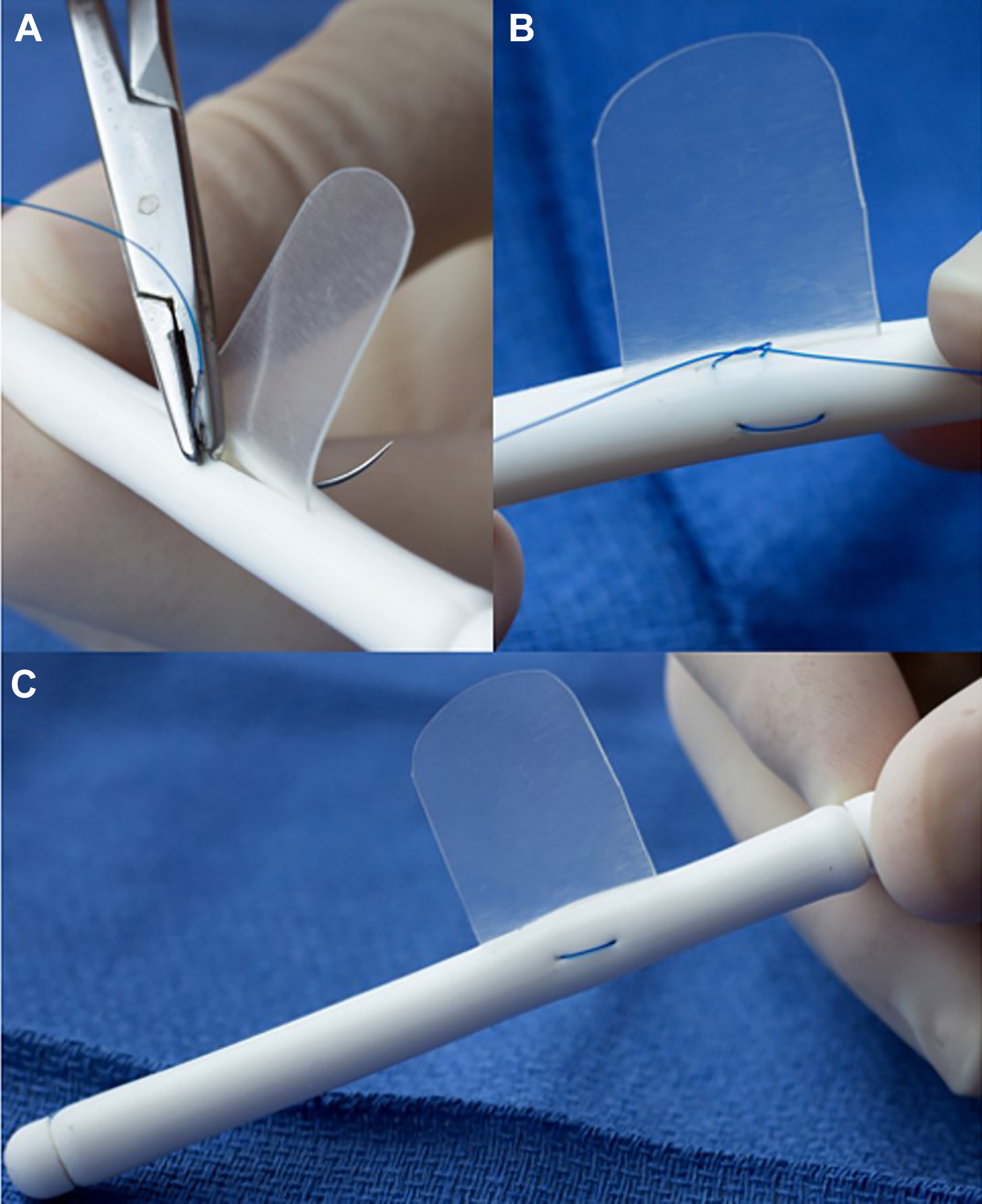
A, Starting and finishing the suture inside the lumen of the stent allows the knot to be inside the stent minimizing irritation. B, The knot being tied into the lumen of the stent. C, Final stent with silicone sheet secured in place with 3-0 Prolene suture.
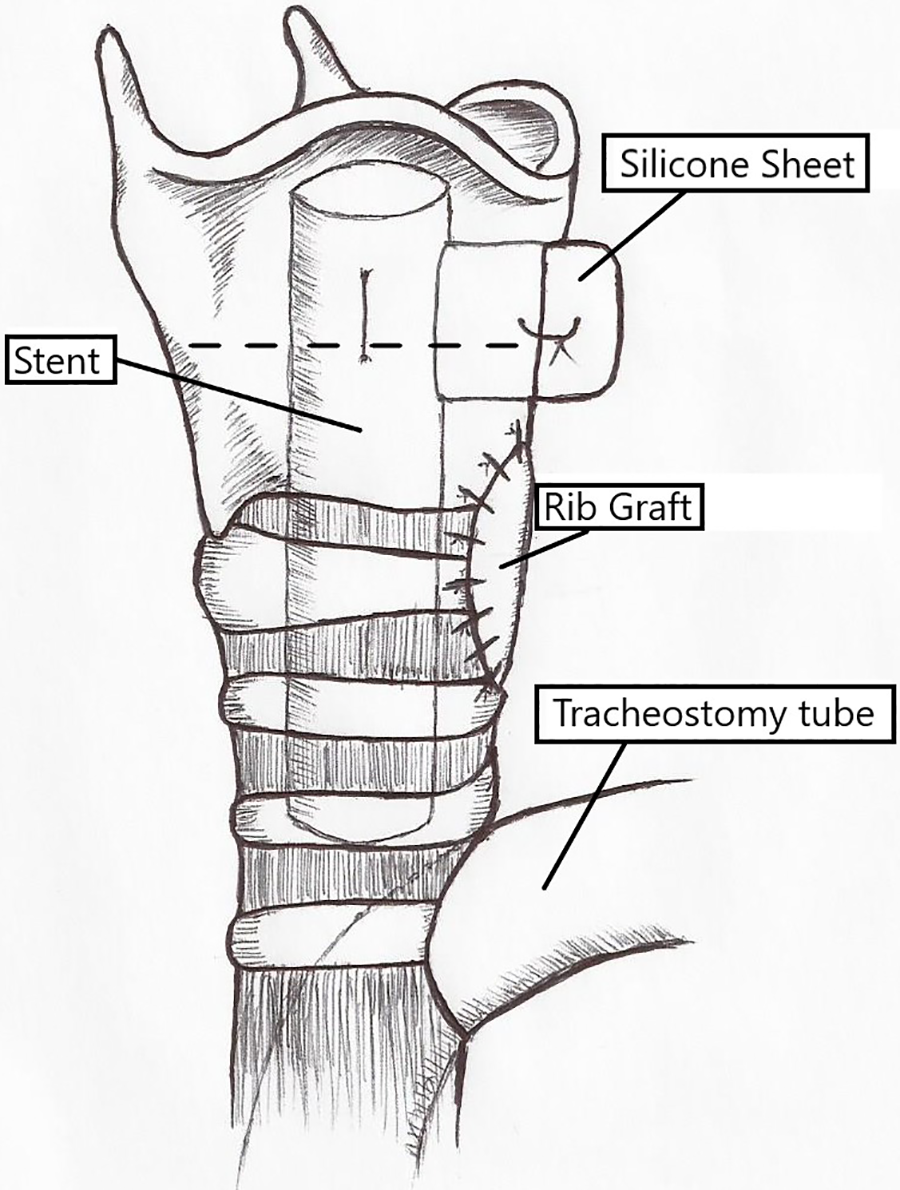
Illustration by the author showing the approximate location of the customized stent with the silicone sheet extending through the thyroid cartilage. Labels identify the stent, the silicone sheet, the tracheostomy tube, and the rib graft. The broken line represents the approximate level of the glottis.
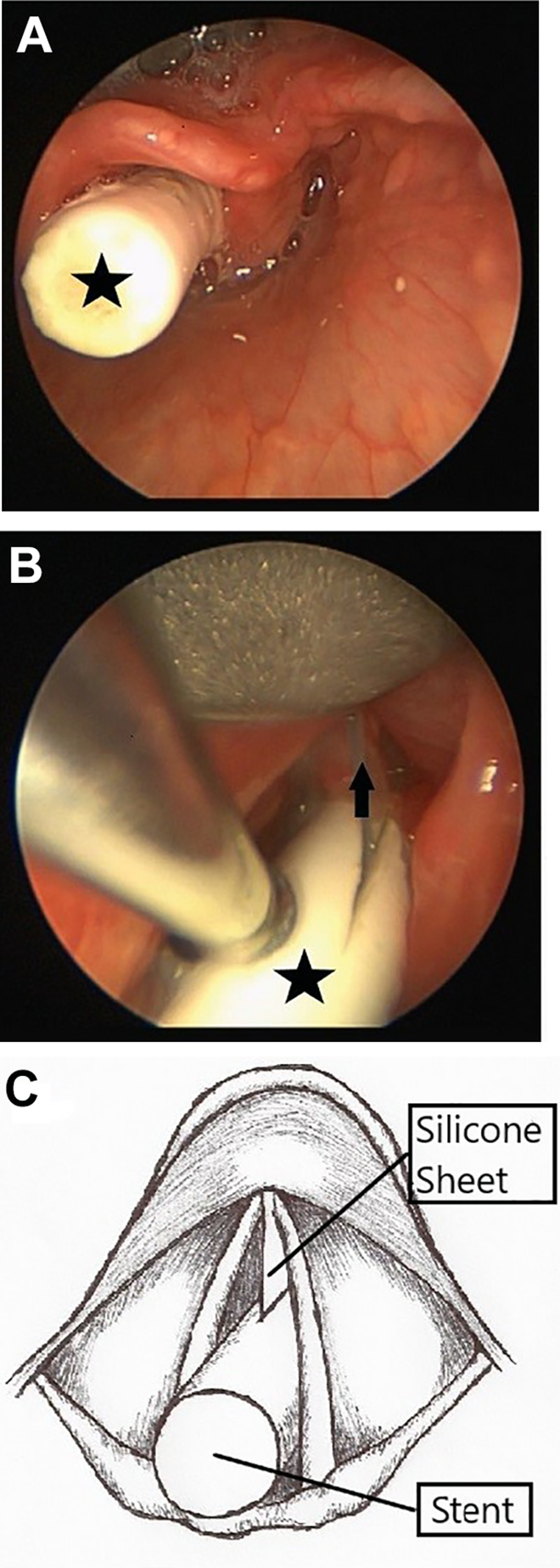
Intraoperative image of stent in place. A, Stent extending into the supraglottis. B, Silicone sheet extending through the anterior commissure. The star identifies the stent, the arrow identifies the silicone sheet. C, Illustration by the author showing the approximate location of the customized stent and silicone sheet within the glottis.
Results
Five weeks after surgery, the stent was removed. The thyroid cartilage and anterior glottic commissure were reapproximated with a horizontal mattress suture. Significant granulation tissue was identified at the superior edge of the stent in the supraglottis. Repeat direct laryngoscopy 3 weeks and 5 months after stent removal revealed near total resolution of granulation tissue. The patient ultimately experienced some restenosis at the level of the glottis with approximately 10% anterior webbing and wide patency of the glottis and subglottis (Figure 6). The patient was ultimately decannulated and her vocal function has dramatically improved.

Postoperative image of glottis with significant improvement. Note a small wrest of granulation tissue which resolved with time.
Discussion
Laryngotracheal reconstruction with stent placement has become the definitive repair for laryngeal stenosis. 2,3 Features of the ideal stent would include ability to be customized to fit the specific shape of stenosis, ability to establish and maintain postoperative airway patency, ability to remain in place with minimal migration, and be constructed of inert material to minimize irritation and formation of granulation tissue. 7 The majority of commercially available stents are cylindrical in shape in either a straight or T configuration; the most commonly used being the Montgomery T-tube. 8 Although these stents adequately approximate the cylindrical anatomy of the subglottis and trachea, they do not approximate the complex triangular shape of the glottis. Efforts have been made to produce stents which more accurately represent upper airway anatomy, the LT-Mold is a promising example. 9 -11
The case described above demonstrated severe glottic webbing in addition to subglottic stenosis. Stenting is particularly important in cases with thick glottic webbing because of the propensity for this area to restenose after excision of the web. 3 Because this patient had a tracheostomy, we had the freedom to use the stent of our choice. We chose the Rutter stent for its ability to stabilize and maintain the expanded airway after LTR with cartilage graft and modified it with the anteriorly projecting silicone sheet in an attempt to prevent restenosis at the glottis. By allowing the silicone sheet to pass through the anterior commissure, the true cords are separated and allowed time to remucosalize postoperatively. Suturing the silicone sheet stabilizes the sheet in place and prevents it from falling back into the larynx. Burying the suture just beneath the skin allows for easy dissection and removal of the suture during stent removal. This combination of a vertically oriented silicone sheet and a cylindrical silicone tube provides postoperative separation of the vocal cords to and through the anterior commissure and postsurgical stabilization of the subglottis. Despite the extension of the silicone sheet through the anterior commissure for 5 weeks postoperatively, this patient ultimately had restenosis of the anterior 10% of her vocal cords.
In conclusion, using a modified stent as described in conjunction with LTR for glotto-subglottic stenosis is a viable option to postoperatively stent the larynx in a more anatomically accurate fashion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.