
Abstract
The purpose of this study to compare lacrimal sac flap preserving techniques with or without fibrin glue in patients undergoing endoscopic endonasal dacryocystorhinostomy. A retrospective study included 132 patients who underwent unilateral endonasal dacryocystorhinostomy between February 2011 and March 2016. Patients were divided into 2 groups: the nonfibrin glue group (n = 66) and fibrin glue anastomosis group (n = 66). Surgical success was defined as the patients’ subjective report of relief of epiphora and objective endoscopic confirmation of ostium patency confirmed by a positive functional dye test. These parameters were compared between the 2 groups. Both groups were similar, in terms of demographic and clinical characteristics. The surgical success rate was significantly higher in the fibrin glue anastomosis group (95.5%) than in the nonfibrin glue group (84.8%; P = .041). Complication rate was 6.1% in the nonfibrin glue group, whereas in the fibrin glue anastomosis group, it was 4.5%. The complication rate was similar in both groups (P = .99). Creation of an anastomosis between the lacrimal sac flaps and the nasal mucosa using fibrin glue improves the outcome of endonasal endoscopic dacryocystorhinostomy.
Keywords
Introduction
Endoscopic endonasal dacryocystorhinostomy (EEDCR) is a surgical method widely used in patients with chronic dacryocystitis. The surgical success rate of EEDCR is similar to that of external dacryocystorhinostomy (DCR) surgery; EEDCR has a success rate ranging from 58% to 94%. 1 -5 Factors associated with the success of EEDCR include patient selection, surgical technique, occurrence of bleeding, inflammation and fibrosis, and the presence of an atonic lacrimal sac. 6,7
Although the literature shows that nasal mucosal flap preservation during DCR surgery is associated with an higher surgical success rate than flap excision, some studies report that flap preservation has no effect on surgical outcome. 8 -10 In addition, although there is no statistically differences, the lacrimal sac flap preservation has been shown to improve surgical outcomes in some studies. 11,12 The different flap preservation techniques and adjuncts such as silicone stents, mitomycin C, tissue glue, and merogel dressing increase the variety of surgical techniques. 13 In recent literature, there are few studies regarding tissue adhesives in EEDCR. 12,14 The present study aimed to investigate the therapeutic efficacy of the fibrin glue application in the lacrimal sac preservation technique.
Patients and Methods
The study included 132 patients who underwent unilateral EEDCR between February 2011 and March 2016; 66 EEDCR cases that we performed without using fibrin glue until 2013 were compared to an equal number of EEDCR cases using fibrin glue. All surgeries were performed by the same team consisting of an otolaryngology specialist experienced in endoscopic transnasal surgery and an ophthalmologist. The ophthalmologist performed cannula insertion and probing while the otolaryngologist inspected the nasal cavity. Preoperatively, each patient underwent fluorescein dye test and cannula insertion together with endoscopic examination of the nasal cavity. Patients with obstruction of the distal nasolacrimal duct based on preoperative assessment and a negative history of lacrimal surgery were included in the study. Patients intraoperatively diagnosed with lacrimal sac fibrosis, an atrophic sac limiting the creation of flaps, or a severely inflamed sac (intraoperative pus discharge) were excluded from the study. Majority of the cases (n = 126) had postsaccal disease as presaccal obstruction cases were quite limited in number (n = 6) which did not interfere the results statistically, they were not investigated as a separate group. Patients aged <18 years and those with severely inflamed intranasal mucosa (chronic sinusitis, intranasal mass, and diffuse nasal polyposis) were also excluded. Demographic data, medical history, physical examination findings, dacryocystography findings, and surgical modality were recorded. Follow-up data (relief of epiphora) and outcome (endoscopic confirmation of ostium patency) were also noted. A Tertiary Reference Center Ethics Committee approved the study protocol (approval no. GO-17/186), and written informed consent was obtained from each patient following detailed explanation of the study’s objectives and protocol.
Surgical Technique
All surgeries were performed under general anesthesia. During the initial stage of both surgical procedures, decongestion was provided using an adrenaline-soaked pad. The caudal portion of the middle concha and nasal mucosa were treated with a 2-mL mixture of lidocaine (20 mg/mL) and epinephrine (0.0125 mg/mL; Jetokain, Adeka, Istanbul, Turkey). The nasal mucosa was incised, starting 0.5 cm above the adhesion point of the middle concha and extending 1 cm anteriorly, turning down and passing the upper limit of the inferior concha, eventually reaching the anterior border of the uncinate process. The nasal mucosa was elevated up to the anterior border of the uncinate process, and flaps were excised.
During surgery, the bony wall of the lacrimal sac was removed using a hammer-chisel technique and a Kerrison punch. A vertical incision was made in the sac wall using a sickle-shaped blade. After making upper and lower releasing incisions, horizontal “H” shape incision was completed, and then the anterior and posterior lacrimal sac flaps were created (Figure 1A-D). The sac flaps were preserved in both groups. The anterior and posterior sac flaps were juxtaposed end to end with the anterior and posterior nasal mucosa, and the gelatin sponge (Spongostan standart, Ethicon, Istanbul, Turkey) was placed on the sac flaps. Dacryocystorhinostomy in the fibrin glue group involved anastomosis of the nasal mucosa and lacrimal sac wall using 2 mL of fibrin glue (1 mL of thrombin and 1 mL of fibrinogen solvent (Tisseel Lyo, Eczacıbaşı-Baxter, Istanbul, Turkey; Figure 2A-D). At the end of each surgery, each patient was intubated using a silicone tube (O’Donoghue tube). Nasal packing was not performed, and bleeding was controlled using adrenaline-soaked pads.
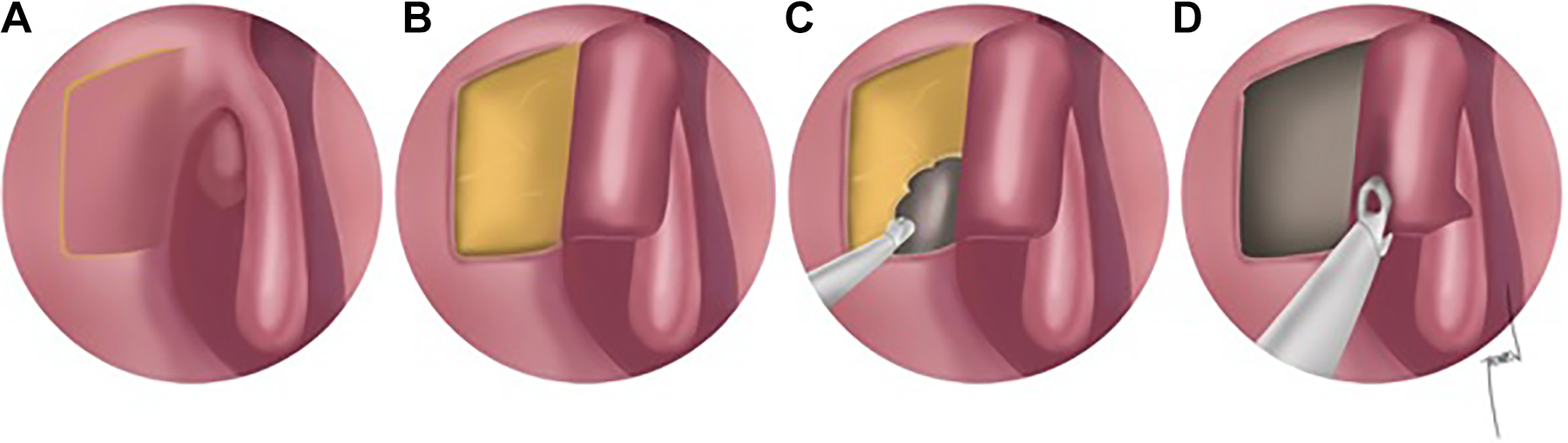
Illustration of the initial step of the surgical procedure. A and B, Anterior and posterior sac flap creation. C and D, Approximation of sac flaps and nasal mucosa.
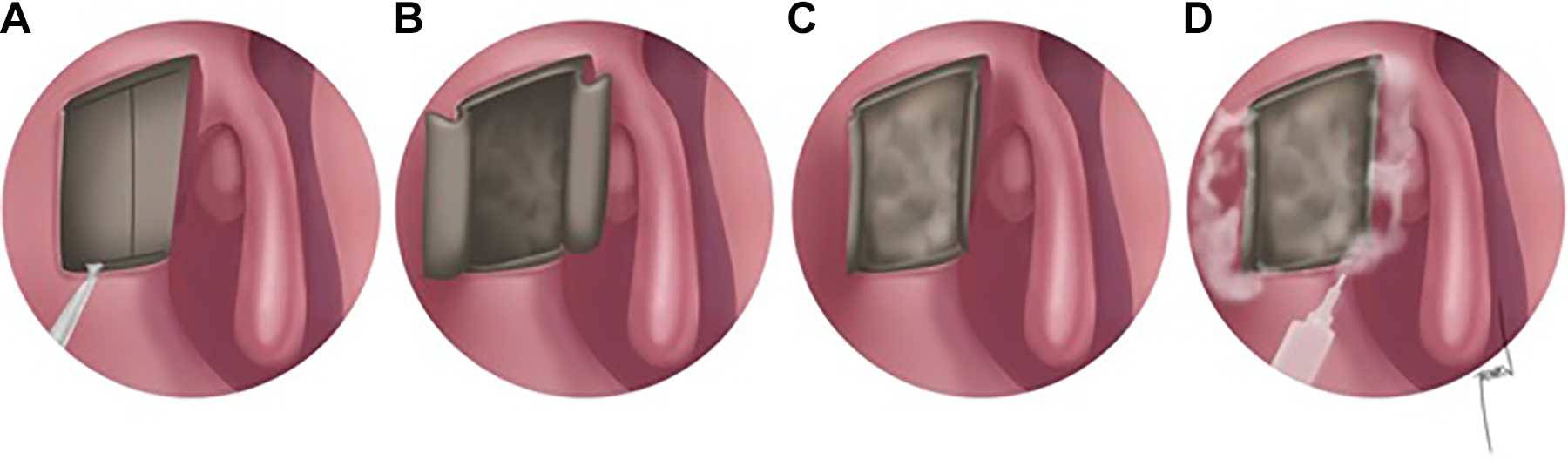
Illustration of the sac flaps preparation and fibrin glue application. A-C, Application of fibrin glue. D, After fibrin glue application.
Postoperative Care and Follow-Up
Postoperative care in both groups included 1-g amoxicillin/clavulanate potassium tablets postoperatively twice daily for 1 week (Augmentin, GlaxoSmithKline, Istanbul, Turkey) and a combination of antibiotic and steroid eye drop (Tobradex, Alcon) thrice daily for 10 days. The patients were recommended to perform nasal cavity irrigation with saline to prevent crust formation. The silicone tube was removed 6 months postsurgery, and the surgical success rate in each group was based on the findings at 1 year postsurgery.
The endoscopic dye test performed is as follows: an ophthalmologist administered a solution of 0.9% saline and methylene blue through the inferior punctum, and then an otolaryngologist used an endoscope to visualize the rhinostomy area. Objective surgical success was based on a patent nasolacrimal passage confirmed via a functioning rhinostomy, which was confirmed by the passage of methylene blue dropped over the conjunctival fornix from the operation side. Surgical failure was defined as no improvement in epiphora and/or no methylene blue passage observed via endoscopic examination.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows version 22.0 (IBM Corp, Armonk, New York). Data are shown as mean (standard deviation), range, and percentage, as appropriate. Gender distribution, complications, and the surgical success rate were compared between groups. As gender distribution was normal, the t test was used for descriptive purposes. As the distribution of follow-up time was not normal, the Mann-Whitney U test was performed to compare follow-up period. The χ2 test and Fisher exact test were used to compare categorical variables. The level of statistical significance was set at P < .05.
Results
Patient Demographics
The demographic characteristics of the 2 groups did not differ significantly (P > .05). Of the 66 patients in the nonfibrin glue group, 16 (24.2%) were male and 50 (75.8%) were female, with a mean age of 44.59 ± 16.51 years. The 66 patients in the fibrin glue anastomosis group had a mean age of 48.73 ± 14.74 years, and 12 (18.2%) were male and 54 (81.8%) were female. Mean duration of follow-up was 10.45 ± 7.39 months in the nonfibrin glue group versus 11.36 ± 7.63 months in the fibrin glue anastomosis group (Table 1).
Demographic features and mean follow-up time of patients.
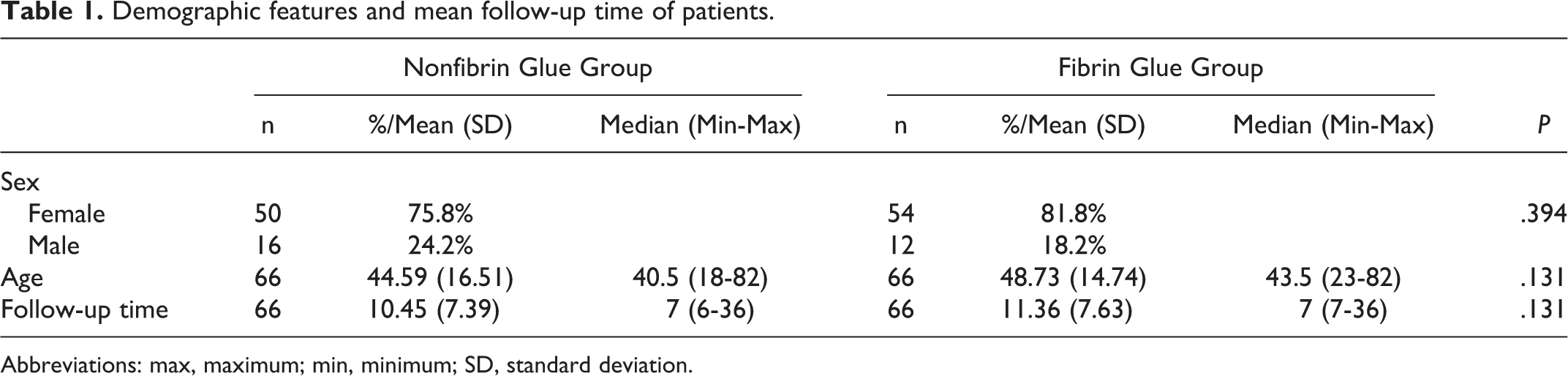
Abbreviations: max, maximum; min, minimum; SD, standard deviation.
Surgical Success and Complications
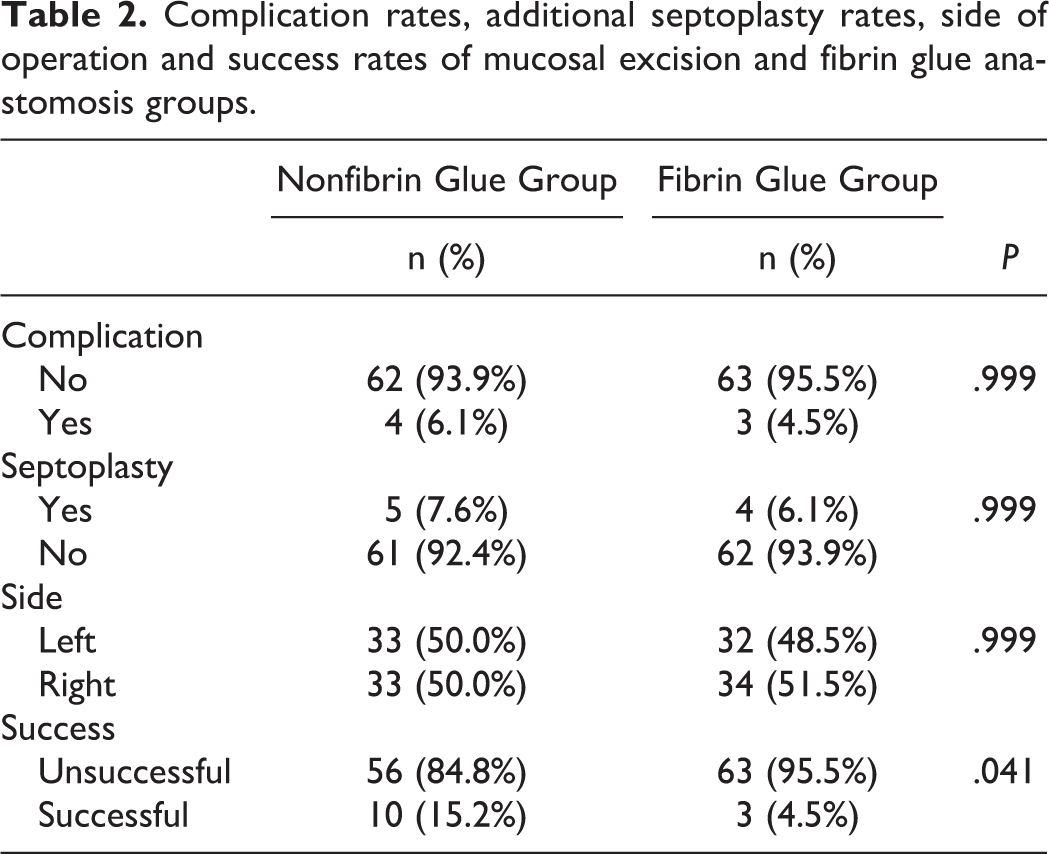
The patients were followed up monthly, with a mean follow-up of 11 months (range: 7-36 months). The surgical success rate was significantly higher in the fibrin glue anastomosis group (95.5% [63/3]) than in the nonfibrin glue group (84.8% [50/16]; P = .041). Of the 16 patients in the nonfibrin glue group who experienced surgical failure, 2 remained symptomatic despite confirmed anatomical patency and 9 underwent revision surgery, including bony wall excision; excision of the mucosa and sac wall due to the occurrence of neo-osteogenesis (n = 1); incision into the medial wall of the sac, which was totally excised using Blakesley forceps (n = 2); and excision of granulation tissues using Blakesley forceps, so as to enable patency (n = 6). In all 9 of these patients, revision surgery enabled patency, although 1 of the patients remained symptomatic.
Among the 3 patients in the fibrin glue anastomosis group who experienced surgical failure after primary surgery, 1 remained partially symptomatic despite endoscopic confirmation of patency, and the other 2 underwent revision surgery are as follows: an incision was made into the medial wall of the sac, and the sac was removed without the creation of flaps (n = 1); granulation tissue was excised (n = 1). Revision surgery was successful in all 3 patients.
Additional nasal surgery—if exist was noted also. Septoplasty was performed in addition to DCR in 5 patients in the fibrin glue anastomosis group and in 4 patients in the nonfibrin glue group. The addition of septoplasty did not affect the surgical success rate in either group and groups were similar (P = .99); all the patients who underwent septoplasty together with DCR (except for 1 in the flap excision group) were considered surgical success. Complications in the flap excision are as follows: ecchymosis (n = 2), postoperative bleeding (n = 1), and exposure of orbital fat tissue (n = 1), for an overall complication rate of 6.1%. In the fibrin glue anastomosis group, complications are as follows: bleeding (n = 1), orbital fat exposure (n = 1), and ecchymosis (n = 1), for an overall complication rate of 4.5%. All patients with complications were considered as surgical success, except for 1 patient in the nonfibrin glue group in which electrocauterization was required to control bleeding. Nasal packing was not used in any of the patients in either group. In other patients, postoperative bleeding was controlled using an adrenaline-soaked pad. The complication rate was similar in both groups (P = .99; Table 2).
Complication rates, additional septoplasty rates, side of operation and success rates of mucosal excision and fibrin glue anastomosis groups.
Discussion
Critical steps for external DCR techniques include wide bone removal to reveal the entire lacrimal sac wall, primary suturing after excision of the lacrimal sac wall and the nasal mucosa, and preventing the formation of granulation tissue. 15 -18 Endoscopic DCR requires accurate localization of the bony ostium, so as to visualize the entire bony medial wall of the lacrimal sac. The lacrimal sac is located in front of the middle turbinate and approximately 8 to 10 mm superior to the middle turbinate adhesion. 19,20 When performing DCR surgery, we took great care to remove the entire bony medial wall of the lacrimal sac. Preservation of the nasal mucosal flap in EEDCR reduces the formation of granulation tissue, thus improving the surgical success rate. 11,12,21 -23 In contrast, other studies report that removal of the nasal mucosal flaps has no effect on the surgical success rate. 21,24 There are many methods for creating mucosal flaps, including U-shaped or V-shaped flaps, with higher success rates than external methods. 9,25 In our study, the nasal mucosal flaps were excised in both groups.
In the present study, the bony medial wall of the sac was removed using a hammer and 4-mm wide chisel. Concomitantly, the bone window was expanded using a Kerrison punch, revealing the entire medial wall of the sac. Use of a microdebrider, drill, and laser is reported to be helpful for bone excision. 26,27 Complete removal of the medial wall is important for optimal preparation of the flaps and to ensure an optimal opening.
It is already a known fact and well established in the current literature and a systematic review by Green et al; flap preservation yield more satisfactory results than flap excision. 13 Additional factors which may affect the surgical success should be the new subheading in EEDCR studies. Interestingly in our study, nonfibrin glue group yielded results similar to mucosal excision cases reported in abovementioned studies. Park et al applied sodium hyaluronate solution as an adjunctive to EEDCR and they concluded that the use of sodium hyaluronate reduced postoperative granulation and increased surgical success. 28 Intraoperative mitomycin C application also seems to be a safe adjuvant that could reduce the closure rate of the osteotomy. 29
Additional procedures and applications of materials that ease the surgery and enhance the surgical outcomes are a novel topic in this area. Thus, we prefer to investigate a commonly used product “fibrin glue” in various surgical interventions especially in gastrointestinal surgery. In our clinic, fibrin glue is widely used in our daily otolaryngology practice such as repair of skull base defects, pharyngocutaneous fistula treatment, and cavity obliteration after mastoidectomy. Since it is a well-tolerated biomaterial and reduces bleeding after surgery, it gains popularity especially after nasal surgery. Brihaye et al used fibrin glue in choanal atresia surgery and they found that mucosal flaps secured with fibrin glue minimize the risk of restenosis. 30 Ophthalmologists are familiar to fibrin glue and also it is well documented in a recent review that fibrin glue may result in less recurrence and may take less time than sutures for fixing the conjunctival graft in place during pterygium surgery. 31 Up to date, there were no larger series in the literature regarding fibrin glue use in EEDCR.
The disadvantage of routine use of fibrin glue in EEDCR is the additional cost. Tisseel (TISSEEL) fibrin glue costs about US$140 per case. It is prepared for use by the surgical nurse during the previous stages of the surgery, and the application takes 10 to 15 seconds. Therefore, indirect costs are negligible. According to the information, we received from the finance department of our hospital, average total cost of an endoscopic DCR operation is US$928 35. Accordingly, the additional cost of fibrin glue is about 15% in our hospital. On the other hand, the use of fibrin glue in our study seems to have resulted in an additional cost of 5% in total due to an increase in surgical success rate of approximately 10%. However, cost analysis may differ between countries and centers depending on different prices and costs.
Earlier studies reported that 14% to 47% required additional procedures after EEDCR. 15,32 In the present study, only 6.8% of patients required additional surgery following the occurrence of any complaint or deviation of the septum which is not allowing surgery. The use of preoperative dacryocystography to confirm the diagnosis of distal nasolacrimal duct obstruction and exclusion of revision cases are both distinctive issues in this study. The present study is among the largest to report outcomes in patients who underwent EEDCR with the sac flap preservation. Surgical success in the present study was measured both objectively (based on patency on irrigation confirmed by methylene blue irrigation) and subjectively (relief of epiphora). The present findings also show that cooperation between otolaryngologists and ophthalmologists is necessary for optimum management of such patients.
The modifications of EEDCR techniques have been introduced to improve the surgical success rate and prevent the formation of granulation tissue. Among rhinologists, fibrin glue is known to be effective for preventing graft and flap migration and to improve wound healing. In the present study, fibrin glue was used to prevent migration of lacrimal sac flaps and to inhibit the formation of granulation tissue. Based on the present findings, we think that additional use of fibrin glue might improve the already well-established success rate of EEDCR with the sac preservation.
Conclusion
In conclusion, the present findings indicate that preservation of lacrimal sac flaps with end-to-end anastomosis to the nasal mucosa using fibrin glue has a positive impact on surgical outcome in patients undergoing EEDCR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.