
Abstract
Background/Purpose:
To retrospectively analyze the epidemiological features, clinical diagnosis, and treatment of 610 patients with maxillofacial fractures, while providing a reference for the prevention and optimized treatment of maxillofacial fractures.
Methods:
Data of patients with maxillofacial fractures who were treated and followed up at the Second People’s Hospital of Kashi Prefecture from June 2012 to April 2018 were summarized. The epidemiological features, clinical manifestations, fracture sites, treatment methods, and results were analyzed.
Results:
The highest incidence was in the age range of 20 to 49 years. The main cause of fracture was traffic injury. Mandibular fractures accounted for 37.77%, zygoma and zygomatic arch fractures for 37.00%, and maxillary fractures for 21.19%. Atypical zygomatic arch fractures were more common in the maxilla, followed by Le Fort I and II fractures. Closed fractures accounted for 85.97%. Many (73.39%) patients were treated with computed tomography 3-dimensional (3D)-mediated precision modified incision internal fixation with satisfactory results.
Conclusions:
There is a high incidence of maxillofacial fractures among young men, especially in summer, with the most common injuries being traffic-related injuries. The most common site is the mandible, followed by the zygomatic arch, zygomatic complex, and maxilla. Computed tomography 3D-mediated precision modified incision internal fixation can achieve satisfactory results.
Introduction
The oral and maxillofacial regions are extremely vulnerable to damage. Although injuries to this area may be less life-threatening than injuries to vital organs such as the brain, the destruction of chewing function and facial appearance, and the accompanying psychosocial disorders can be devastating. 1 As the most prominent feature on both sides of the midface, the zygoma and zygomatic arch are easily injured in car accidents and blows to the face. In particular, the zygomatic arch is a slender and weak arched structure that is composed of the processus temporalis ossis zygomatici and the processus zygomaticus ossis temporalis. These bones are prone to fracture after trauma, and dislocation often occurs in the fractured segment. This can affect appearance and cause limited mouth opening and disturbance of occlusion; therefore, intervention is imperative. Maxillofacial fractures are clinically common, accounting for 3.2% to 3.8% of all body fractures and 80% of maxillofacial trauma. 2 This study retrospectively analyzed the epidemiological features, clinical manifestations, fracture sites, treatment methods, and results of 610 patients with maxillofacial fractures. We noted the efficacy of treatment with computed tomography (CT) 3-dimensional (3D)-mediated precision modified incision internal fixation and provided recommendations for the prevention and optimized treatment of maxillofacial fractures.
Material and Methods
Clinical Data
The study participants were hospitalized patients who had maxillofacial fractures and were treated at the Department of Otolaryngology and Head and Neck Surgery of the Second People’s Hospital of Kashgar Prefecture from June 2012 to April 2018. For each patient, the sex, age, occupation, time of onset, cause of injury, combined injuries, clinical manifestations, fracture sites, and timing and methods of treatment were summarized in detail. This study was in accordance with protocols approved by the institutional research review board at Second People’s Hospital of Kashi Prefecture, Kashi, Xinjiang Uygur Autonomous Region, China.
Surgical and Approaches
Computed tomography 3D-mediated precision modified incision technique: Adequate 3D CT visualization and modeling with properly identified and virtually reduced fracture segments represents key planning features and potentially offers extended patient assessment, planning, and treatment options. All CT images were reorientated according to a reference CT scan representing the desired head position. This technical step ensured that each fracture segment of the mandible was properly identified, separated, and thereby independently movable. The fracture characteristics were identified by inspecting both the multiplanar CT slices and 3-D reconstruction of the mandible. A novel semiautomatic landmark-based approach was implemented to separate the segments.
Among the 610 (mean age: 31 ± 14.88 years) patients with fractures, because the fracture affects the appearance of the face or the function of the maxillofacial bone, 543 were treated with internal fixation and the remainder were treated conservatively. Patients with maxillofacial trauma fractures were treated with an individualized treatment program that was developed according to the cause of the injury and the clinical characteristics of injury, using small titanium and micro titanium plates for fixation. The facial nerve branches were empirically positioned according to the markers that corresponded to the conventional facial nerve surface position. The conventional pathway of the facial nerve was avoided during fixation. In some cases, the facial nerve branch near the area of the fracture surgery was dissected out and protected according to markers corresponding to the conventional facial nerve surface position (facial nerve monitoring). This allowed damage to the facial nerve to be avoided during fixation (Figure 1).
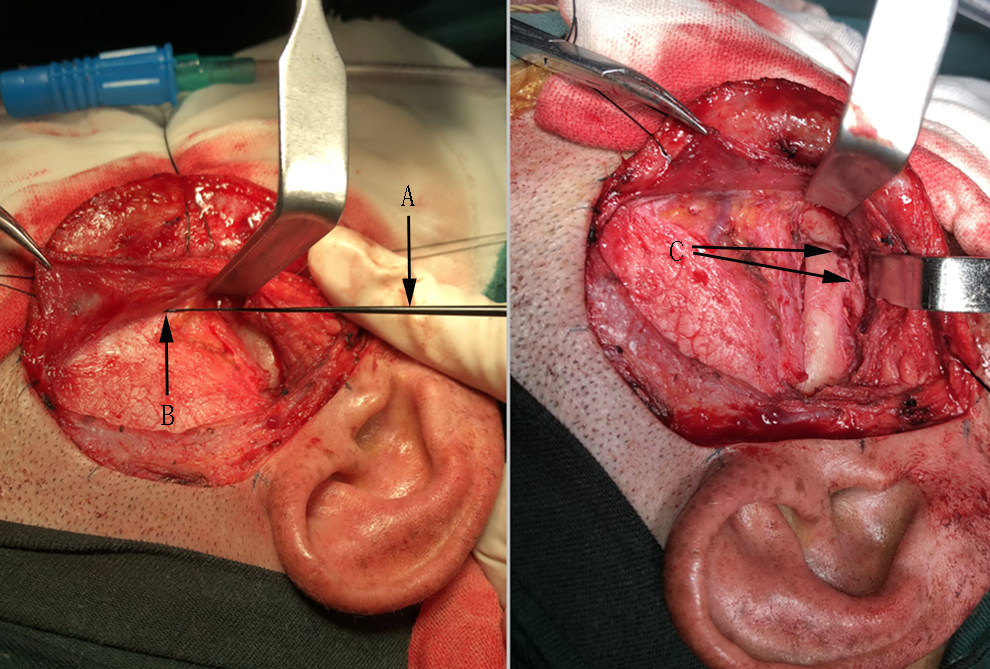
Modified excision and exposure of the zygomaticomaxillary complex fracture site with facial nerve monitoring: (A) facial nerve monitoring probe, (B) facial nerve branch, and (C) site of the zygomatic arch and zygomatic maxillary process fracture.
Preoperative X-ray and CT examinations can be used to select a reasonable surgical approach for the patient after identifying the patient’s maxillofacial fracture site and type. Treatment for 119 patients with mandibular body and symphysis fractures involved internal fixation using the intraoral vestibular groove approach. For 33 patients with mandibular angle and mandibular ascending ramus fractures, fixation was achieved through the posterior molar incision, exposing the lateral mandibular angle and fracture lines, and fixation of the mandibular small bone fracture plate along the external incisions after the reduction in bone segments, followed by restoration of the occlusal relationship and internal fixation. The fracture reduction can be conducted by the medical staff in the surgery to obtain the correct occlusal relationship and remove the free broken bone fragments and soft tissue at the fracture site.
Teeth on the fracture line that would affect healing of the fracture could be removed at this time, and a titanium plate can be used for shaping and internal fixation. It is important to ensure that the titanium plate conforms closely to the bone surface.
Among the 45 cases with condylar fractures, an anterior tragus to posterior jaw incision and a submandibular incision was selected according to the elevation of the fracture site, to create a layered incision that can be peeled away to expose the fracture site, explore the condylar process after fracture displacement, reset it into the acetabulum, and conduct internal fixation with a small bone plate. Conservative treatment was conducted in 17 cases with intracapsular fractures and in 5 cases with condylar fractures. Condyle treatment was conducted in 10 cases with condylar fracture.
Treatment for 315 cases of zygoma, zygomatic arch, maxilla, and lower orbital wall fractures consisted of either a small modified angle incision in the hairline or a small local periorbital incision and intraoral vestibular groove incision. The small modified angle incision extends in an anterior superior direction in an arc shape for approximately 3 cm along the hairline before the tragus and ends 2 cm in front of the midline hairline. The shallow layer of deep temporalis fascia flaps down to about 1 cm from the upper edge of the zygomatic arch to expose the superficial temporal fat layer. The tissue is separated from the superficial temporal fat layer to the zygomatic arch, and the periosteum is cut on the inner side of its upper edge and separated to expose the fractured zygoma and zygomatic arch segment. The fracture is internally fixed with a titanium plate and titanium screws after satisfactory reduction.
The small local periorbital incision and intraoral vestibular groove incision can fully expose a zygomatic arch fracture, lateral orbital fracture, malar and zygomatic arch fractures, and maxillary sinus anterior lateral wall fracture, allowing complex zygomatic fractures to be reset with rigid internal fixation with a titanium plate to restore middle facial appearance and function.
Treatment of 21 cases of open fractures of the maxilla, zygoma, and zygomatic arch involved open reduction and internal fixation through the original incision (Figures 1 –3).
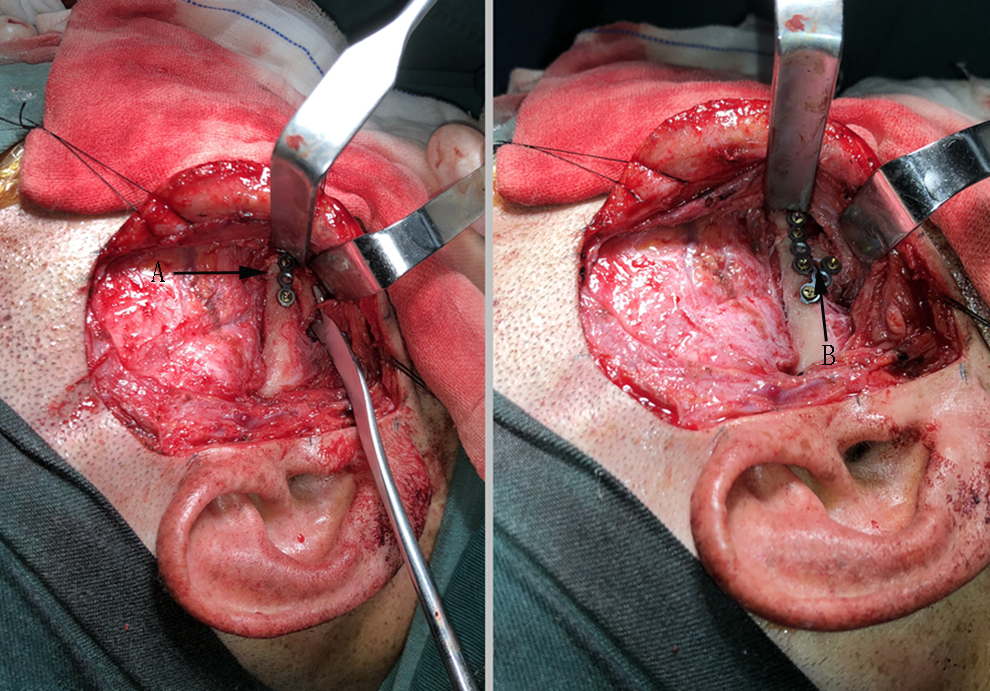
The zygomatic arch fracture is fixed first, followed by fixation of the zygomatic maxillary process fracture. A, Titanium plate fixation for the zygomatic arch fracture and (B) titanium plate fixation for the zygomatic maxillary process fracture.
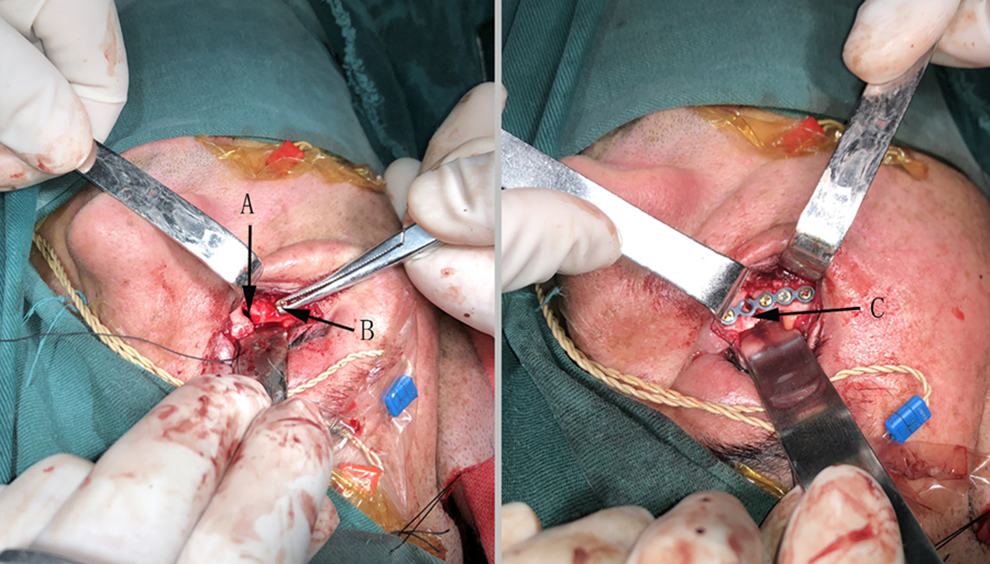
Alignment and titanium plate fixation of a complex lower orbital wall fracture that is difficult to align, using screwed titanium screw pull-ups. A, The lower orbital wall fracture site, (B) the screwed titanium screw, and (C) the fracture site fixed with a titanium plate.
The upper midsurface area included the zygomatic arch, the zygomatic bone, the orbit, and the naso-orbital-ethmoid area. The focus of the surgical reduction in the fracture in this area was to reconstruct the orbit and restore the anterior protrusion, face width, and local morphology of the naso-orbital-ethmoid area. The zygomaticomaxillary complex fracture fixation was usually fixed at the frontozygomatic suture, the lower edge of the orbit, and the zygomaticomaxillary buttress. The vertical struts were fixed with 8-mm titanium nails with L-shaped 7-hole titanium plates. The horizontal struts were 6-mm titanium nails and curved 6-hole titanium board fixation. Panfacial fracture was often accompanied by comminuted fractures in the naso-orbital-ethmoid area; due to the loss of support of the medial orbital margin, they were fixed with 8-mm micro titanium plates.
Statistical Analysis
The information was accurately entered into an Excel spreadsheet and statistically analyzed, and the data of each item were analyzed using descriptive statistics.
Results
General Characteristics
In 610 patients with oral and maxillofacial fractures, there were 412 males and 198 females, with a male-to-female ratio of 2.08:1. The 20- to 49-year group was the most common age-group (347 cases, 56.8%), followed by the 49- to 65-year group (200 cases, 30.2%) and the 0- to 18-year group (63 cases, 10.3%). The number of patients of workers was highest (236 cases, 30.8%), followed by farmers (180 cases, 20.9%), then without a fixed occupation (128 cases, 20.09%).
Etiological Analysis
Oral and maxillofacial fractures were mainly caused by traffic accident injuries (motor vehicle and bicycle injuries), accounting for 52.6% (317 cases), followed by falls (drops and trips), accounting for 22.7% (138 cases); facial blows, accounting for 21.9% (134 cases); and other injuries, accounting for 3.44% (21 cases).
Types of Fracture
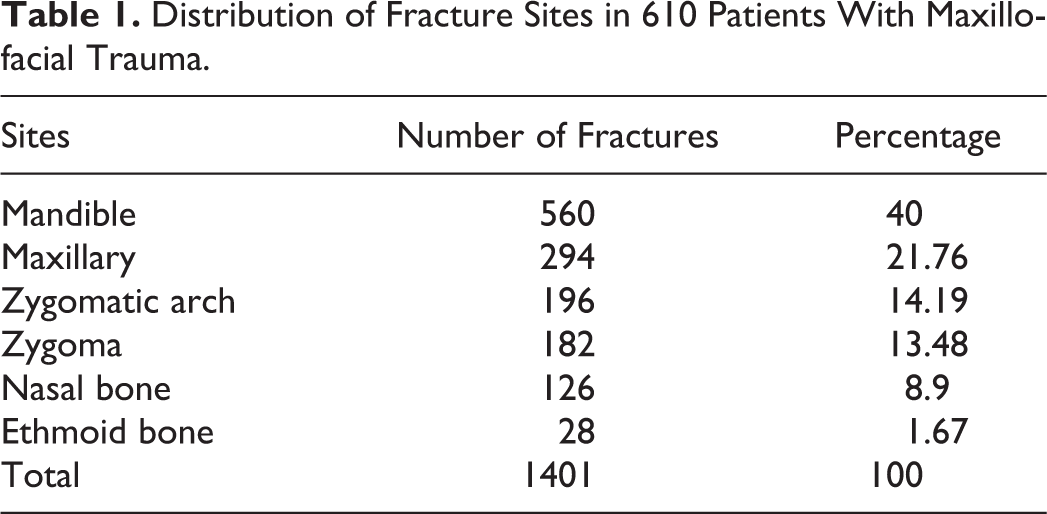
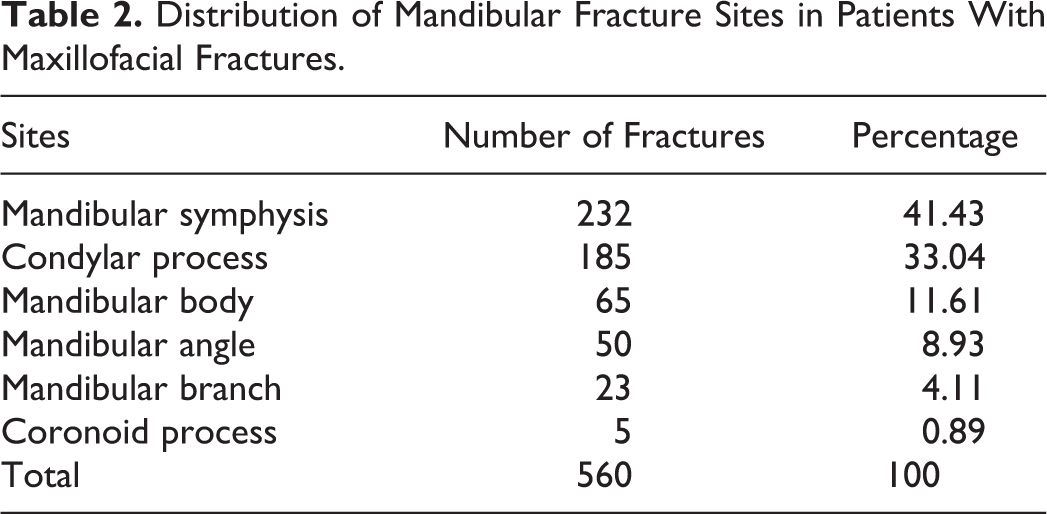
Among the 610 patients, fractures most frequently occurred in the mandible, followed by the maxilla, zygomatic arch, zygoma, nasal bone, and ethmoid bone (Table 1). Mandibular fractures were the most common, accounting for 41.19%, followed by condylar process, mandibular angle, and mandibular body fractures. Mandibular branch and coronoid fractures were rare (Table 2). Among the cases with maxillary fractures, the Le Fort II type had the highest incidence, accounting for 52.25%, followed by Le Fort III and Le Fort I, accounting for 27.93% and 19.82%, respectively. Among all patients with fractures, 439 had multiple fractures, accounting for 72.46%, and 170 had single fractures, accounting for 28.54% (ratio of 2.5:1). A total of 1401 fractures occurred in 610 patients with maxillofacial fractures, and the number of fractures per capita was 2.3.
Distribution of Fracture Sites in 610 Patients With Maxillofacial Trauma.
Distribution of Mandibular Fracture Sites in Patients With Maxillofacial Fractures.
Postoperative Effect and Follow-Up
Computed tomography 3D-mediated precision modified incision internal fixation was used in 73.39% of cases, and 4 cases failed after internal mandibular fixation. These failures occurred after mandibular body, paramedian mandibular, and mandibular angle internal fixation, and all the patients were male. In 3 of these patients, the failed fixation may have resulted from the individual’s oral health condition (gingivitis, dental calculus, gingival recession, and mobile teeth), 1 case was immunocompromised as a result of AIDS, and the surgical incision used was the second most common type of incision in which nonunion occurs.
Our findings suggest that CT 3D-mediated precision modified incision can obtain satisfactory results. Maxillofacial appearance is normal, mouth opening; occlusal relationship and function are normal. Classic preoperative and postoperative controls of incisions for internal fixation of fractures of the maxilla, the zygoma, and the zygomatic arch are shown in Figure 4. The maxillofacial images of internal fixation of comminuted mandibular and zygoma fractures before internal fixation is shown in Figure 5E and F. The maxillofacial images of internal fixation of comminuted mandibular and zygoma fractures 6 months after internal fixation is shown in Figure 5 (images G and H). Considering that the fracture fixation time was sufficient and the fracture had completely healed, so 8 months after internal fixation with mandibular comminuted fractures and zygomatic arch fractures, the titanium plate had been removed, and the maxillofacial images of internal fixation of comminuted mandibular and zygoma fractures after titanium plate removal is shown in Figure 6.
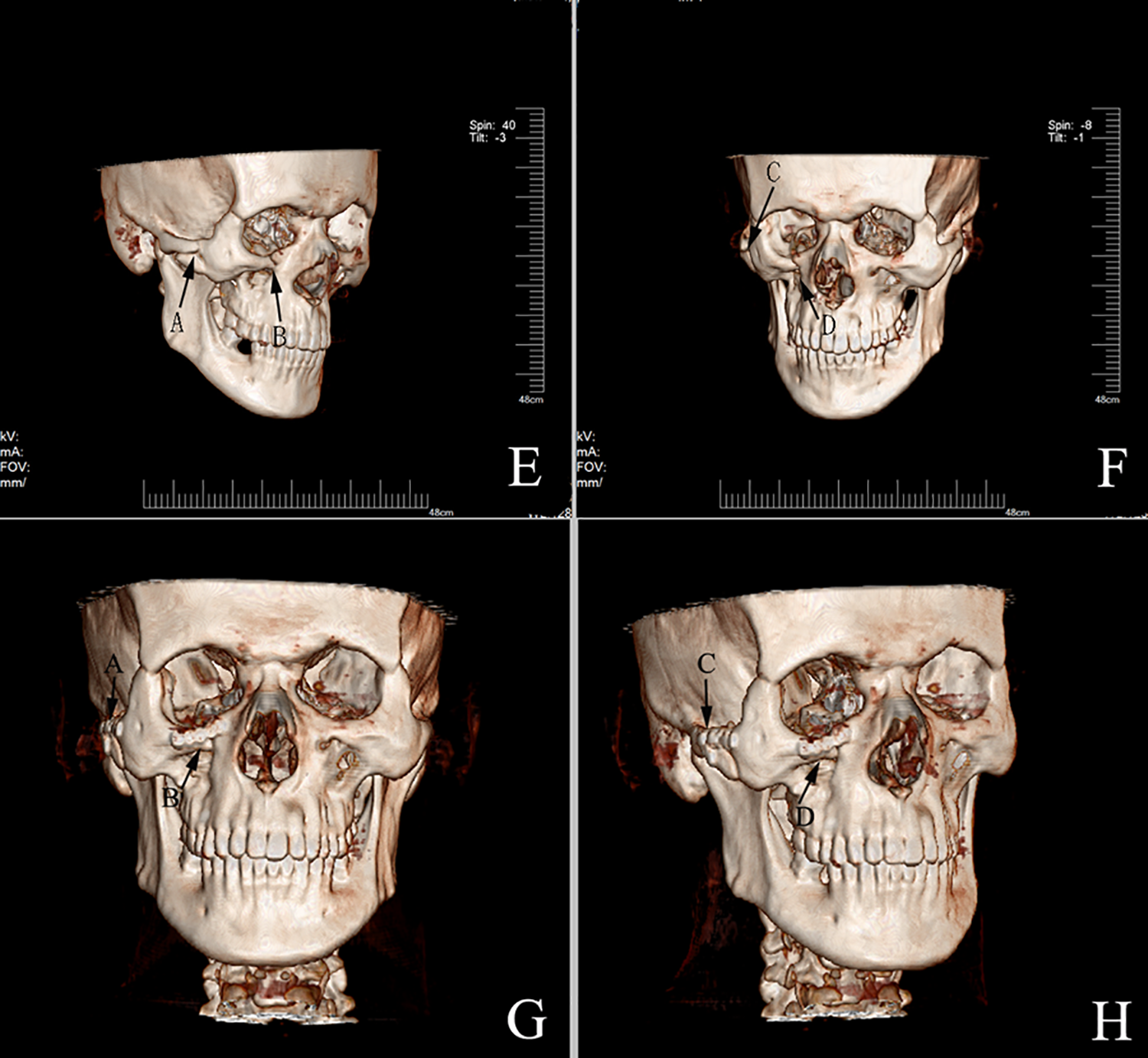
Preoperative image (E and F) of incisions for internal fixation of fractures of the maxilla, the zygoma, and the zygomatic arch. (A and C) Fracture sites of the zygomatic arch and zygomatic maxillary process, and (B and D) fracture site of the lower orbital wall and maxilla. Postoperative image (G and H) of incisions for internal fixation of fractures of the maxilla, the zygoma, and the zygomatic arch.
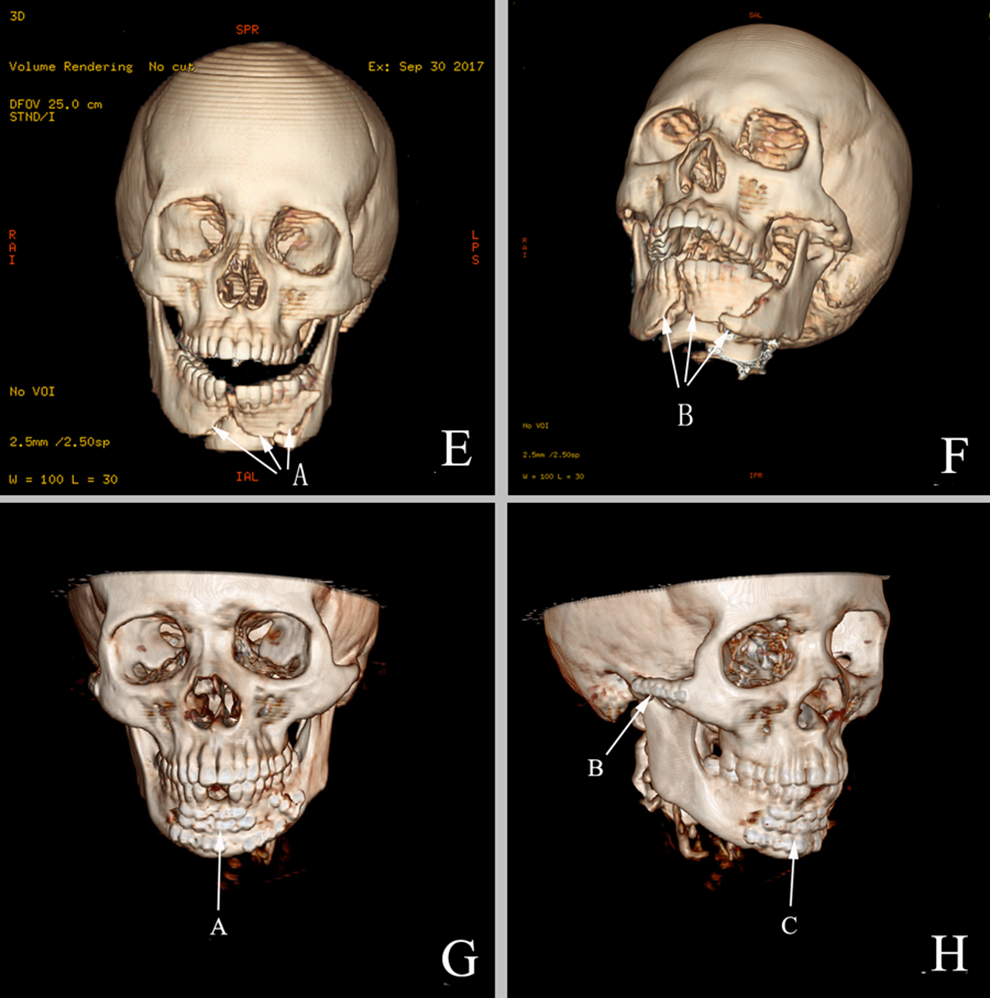
Preoperative image (E and F) of comminuted mandibular and zygoma fractures. A and B, Comminuted mandibular fracture sites. Postoperative image (G and H) of incisions for internal fixation of comminuted mandibular and zygoma fractures. A and C, View after fixation with a titanium plate of comminuted mandibular fractures, and (B) titanium plate fixation site for zygomatic arch fracture.
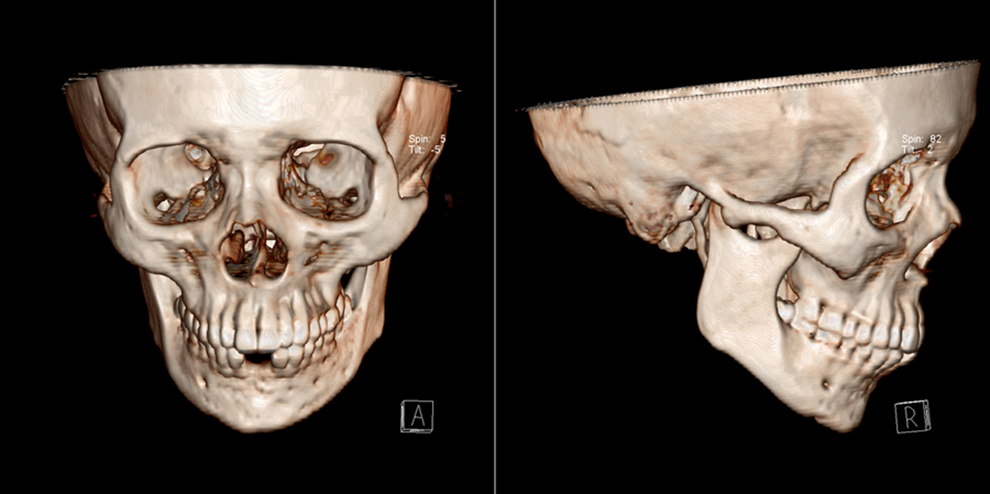
The maxillofacial images of internal fixation of comminuted mandibular and zygoma fractures after titanium plate removal.
Discussion
d’Avila et al’s systematic review and meta-analysis showed including 402 339 patients, traffic accidents especially in Africa and Asia corresponded to the main etiology agent of maxillofacial trauma (34%), followed by falls (31%), especially for schoolchildren, violence such as assaults, fights, weapons, and firearms was more evident in the Americas (11%), sports (4%), and others (5%). 3
This study shows that maxillofacial trauma accounts for a significant proportion of total body trauma, making it a major contributor to the number of maxillofacial surgery cases. In recent years, the incidence of maxillofacial trauma has increased, and injuries have become more severe and more complex. 4,5 Among all causes for maxillofacial trauma, traffic accidents take the lead, accounting for 52.6% in this survey, which is 5.18% higher than the corresponding survey data for 1986 to 1995 (47.42%). 5 The next most common causes were assault, and fall and tumble injuries. These figures are similar to those reported by Bo et al, 6 Zhu et al, 7 and Adebayo et al. 8 Traffic accident injuries are the leading cause of death in people younger than 35 years, and the incidence of maxillofacial trauma in all traffic accidents is as high as 60%. In recent years, China has been involved in the development of the high-speed transportation and automobile industries, but individual awareness of traffic safety and accident prevention is still relatively weak. Many new drivers of private cars are on the road, so the incidence of traffic accident injuries has been increasing year by year. Therefore, strengthening education about road traffic regulations and raising people’s awareness of traffic safety are extremely important for reducing the incidence of maxillofacial trauma. Maxillofacial trauma occurs predominantly in adults, and 56.8% of the cases we studied were in patients between the ages of 20 and 49 years, which is consistent with the statistics reported by Bo et al, 6 Zhu et al, 7 Adebayo et al, 8 and Sastry et al. 9
The age of patients with maxillofacial trauma is gradually decreasing, which may be related to the increasing proportion of minors participating in social activities in recent years. The ratio of males and females experiencing maxillofacial trauma in our study was 2.08:1, which is lower than the results reported by Bo et al (4.31) 6 and Adebayo et al 8 (4.71). This is largely related to the increased participation of women in social activities in recent years in modern society.
The incidence of maxillofacial trauma according to season was highest in summer and lowest in February. This may be related to the heat in summer, making it difficult for motorists to concentrate, and the long holiday for Spring festival in February. Maxillofacial bones develop different injuries because of their specific anatomical structure and location. The mandible is one of the most complex bones in the body in terms of structure and function. It holds a prominent position and occupies one-third of the face. Therefore, it is the site most likely to fracture and accounts for 40% of maxillofacial fractures. The maxilla is the largest bone in the face and is the second most common site of maxillofacial fracture, followed by the zygomatic arch, zygoma, nasal bone, and ethmoid bone. Because of the complicated anatomical structure of the mandible, we found that the incidence of fractures differed for the different locations: the mental region, condylar process, mandibular body, mandibular angle, mandibular branch, and coronoid process. This is consistent with the results of investigations by Bo et al, 6 Zhu et al, 7 and Adebayo et al. 8 The incidence of Le Fort II fractures was the highest of the maxillary fractures, accounting for 52.25%, followed by Le Fort III and Le Fort I fractures, which is consistent with the findings of Bo et al, 6 Adebayo et al, 8 Motamedi, 10 and Gassner et al. 11 A major feature of maxillofacial fractures is the high incidence of multiple fractures. Among all fracture cases, 439 patients had multiple fractures, accounting for 72.46%, and 170 patients had single fractures, accounting for 28.54%; the ratio between the 2 was 2.5:1.
A total of 1401 fractures were found in 610 patients with maxillofacial fractures, and the number of fractures per capita was 2.3, which is higher than the figure of 1.7 reported by Bo et al. 6 This may be caused by 2 factors: first, with the recent increase in the number of patients facing traffic accidents and fall injuries, maxillofacial injuries have become more complex and often feature full facial fractures of multiple anatomical structures; and second, with the development of imaging technology such as 3D spiral CT examination, there is less likelihood of maxillofacial fractures going undiagnosed, and the types and sites of fractures has become clearer. In the treatment of patients with maxillofacial trauma, one should first consider the brain symptoms and treat brain complications and then treat the maxillofacial trauma after stable vital signs are established. With a standardized entry system to record clinical cases, our retrospective analysis has complete scientific data and indicators, few biased and confounding interference factors in the analysis results, and strong research power.
For the traditional surgical incisions in the treatment of zygoma and zygomatic arch fractures, a coronal scalp incision was selected to create a flap under the fascia head, and a pull hook was used to pull it as far as possible to expose the fracture site. In fact, for complex zygoma, zygomatic arch, maxillary, and lower orbital wall fractures, it is difficult to fully expose the fracture site and difficult to fix it with titanium plates. We used modified incisions for extremely complex zygoma, zygomatic arch, maxillary, and lower orbital wall fractures, with small modified angle incisions in the hairline or small local periorbital incisions. If necessary, an intraoral vestibular groove incision could be added to fully expose fractures of the zygomatic arch, lateral orbit, malar and zygomatic arch, and maxillary sinus anterior lateral wall, and the zygomatic complex fracture could be reset with rigid internal fixation with a titanium plate to restore the middle face appearance and function. Advanced postprocessing of preoperative CTs represents an important technique that potentially offers enhanced options in preoperative assessment and subsequent treatment, particularly in patients affected by severe fractures of the mandible. A prior knowledge about the 3D fracture pattern and the spatial positioning, size, and displacement of each fragment provides useful information and enables the surgeon to carry out a preoperative customized fracture reduction plan. 12 Facial nerve branches were empirically positioned according to the markers corresponding to the conventional facial nerve surface position. The conventional facial nerve pathway was avoided and the fracture fixation was conducted. In some cases, facial nerve monitoring was implemented, in that the facial nerve branch near the fracture surgery was dissected out and protected according to markers corresponding to the conventional facial nerve surface position. Facial nerve branches were avoided, and the fracture fixation was conducted. In this study, 73.39% of patients were treated with CT 3D-mediated precision modified incision internal fixation and achieved satisfactory results.
Analysis of the 4 patients in whom fixation failed showed that the failure generally occurred after internal fixation of the mandibular body, paramedian mandible, and mandibular angle, and all 4 failed cases occurred in male patients. The failure may be caused by (1) the patients’ individual oral condition (gingivitis, dental calculus, gingival recession, and mobile teeth); (2) use of the second most common type of surgical incision in which nonunion occurs; (3) the decreased immune function that affects the incision healing of some patients, especially those with AIDS; and (4) individual-specific rejection of titanium plates and screws.
The surgical approach for treating mandibular condylar fractures could affect the rate of seventh cranial nerve injuries. 13 Preoperative maxillofacial thin-slice CT and 3-D reconstruction is conducted to determine the exact location of the fracture. The facial nerve branches are empirically positioned according to the markers corresponding to the conventional facial nerve surface location. In some patients, facial nerve monitoring can be used to assist the surgeon in avoiding facial nerve branches during fracture fixation. The use of CT 3D-mediated precision modified incision internal fixation can achieve satisfactory results.
The upper midsurface area included the zygomatic arch, the zygomatic bone, the orbit, and the naso-orbital-ethmoid area. The focus of the surgical reduction of the fracture in this area was to reconstruct the orbit and restore the anterior protrusion, face width, and local morphology of the naso-orbital-ethmoid area. The zygomaticomaxillary complex fracture fixation was usually fixed at the frontozygomatic suture, the lower edge of the orbit, and the zygomaticomaxillary buttress. The vertical struts were fixed with 8-mm titanium nails with L-shaped 7-hole titanium plates. The horizontal struts were 6-mm titanium nails and curved 6-hole titanium board fixation. Panfacial fracture was often accompanied by comminuted fractures in the naso-orbital-ethmoid area; due to the loss of support of the medial orbital margin, they were fixed with 8-mm micro titanium plates.
We believe that well understanding and identification of the etiologies of maxillofacial fracture could provide a reference for the prevention and optimized treatment of maxillofacial fractures.
Conclusions
There is a high incidence of maxillofacial fractures among young men, especially in summer, with the most common injuries being traffic-related injuries and multiple and closed fractures. The most common site is the mandible, followed by the zygomatic arch, zygomatic complex, and maxilla. Computed tomography 3D-mediated precision modified incision internal fixation can achieve satisfactory results.
Footnotes
Authors’ Note
Drs Yusu Ni and Zhifei Zhang contributed equally to this work. Zenare Ubulksm and Mehreban Turhun contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant 17ZR1404600 from the Nature Science Foundation of Shanghai Science and Technology Committee, grant 18695840500 from Shanghai 2018 Annual “Science and Technology Innovation Action Plan” Domestic Science and Technology Cooperation Project, Shanghai Science and Technology Committee, and grant 2018E02110 from Xinjiang Uygur Autonomous Region Scientific and Technological Assistance Program.