
Abstract
There are many factors that result in the treatment of deep neck infection (DNI). This study aims to compare the results of DNI treatment between referred and walk-in patients. This retrospective cohort study reviewed the data of 282 DNI patients. The peritonsillar abscesses and limited intraoral abscesses were excluded. The outcome of treatment such as duration of hospital stay, the expense of treatment, morbidity, and mortality were reviewed during staying in the hospital. A total of 282 patients were included in this study, there were 152 referred patients and 130 walk-in patients. Patients who were sent to have treatment results were not significantly different from those who had come directly to the hospital regardless of the length of stay, the cost of medical treatment, complications, and death due to complications with sepsis (P = .013). However, the referred patients exhibited a risk to have sepsis 1.1 times more than the patients who went straight to the medical specialists (univariate analysis risk ratio [RR]: 1.1, 95% confidence interval [CI]: 0.8-1.3; P = .620). The results were confirmed in the multivariate analysis after adjusting for age, gender, diabetes, chronic renal failure, cirrhosis, and dental care. It was found that the risk to have sepsis in the “refer in” group was 1.1 times more than the other group (multivariate analysis RR: 1.1, 95% CI: 0.8-1.3; P = .658). In conclusion, the results of treatment in referred patients were not different from walk-in patients. Deep neck infection patients at hospitals that do not have a specialized doctor will receive appropriate treatment because of the effective DNI referral system according to public health systems. However, in referred patients, sepsis should be maintained prior to delivery.
Introduction
Deep neck infection (DNI) is found in all ages and can cause complications and death. 1,2 The success of treatment of DNI depends on many factors. Rapid diagnosis and prompt treatment will reduce complications and death. 3 The controlled comorbidity of the patients and the effective antibiotics also play a role to reduce the complication and mortality. 3,4 The mortality rate of DNI patients was reported as 0% to 2.4% in published papers 2,5 and 1.0% to 8.3% in Thailand. 6,7 However, no mortality was found in any patients with submandibular space. 8
Most hospitals did not have specialized doctors who could treat DNIs. In this scenario, patients who went to the hospital were sent to a center hospital that had specialized doctors according to the public health system. Patients were treated in a small hospital with no specialized physicians without having the opportunity to receive a delayed diagnosis and delayed treatment. These were the causes of complications and death. However, the results of the treatment of the referred patients were not studied.
This study aimed to compare the results of DNI treatment in referred patients with walk-in patients, to assess whether people in areas that do not have specialized physicians have access to quality and effective medical care. This study reported the expense, duration of hospital stay, treatment, complications, and mortality.
Patients and Methods
This study was a retrospective cohort study and conducted at Chiangrai Prachanukroh Hospital, Thailand. This hospital is the regions central hospital with 788 inpatient beds. There are about 1000 patients a year in the Ear, Nose, and Throat (ENT) ward. The hospital has 5 ENT doctors. This study gathered information on patients who came to the hospital from October 2013 to March 2016. The peritonsillar abscesses and limited intraoral abscesses were excluded. This study reviewed the data of every patient from admission to discharge. The patients were divided into 2 groups. The “refer in” patients were the patients referred from general physicians. The “walk in” patients were the patients who came to see the medical specialist in this hospital directly. Potential confounders such as demographic characteristics, health-care insurance, duration of symptom, location of abscess, and underlying disease were reviewed. Between the 2 groups, exposure factors such as surgical treatment and airway management were compared. Outcome parameters were used to assess duration of hospital stay, expense of treatment, morbidity, and mortality. The outcome of treatment was reviewed during their stay in the hospital. The bias in this study was controlled using the same eligibility criteria, exclusion criteria, and diagnostic outcome criteria.
Statistical Analysis
The sample size was calculated as a pilot study. Thirty patients in each group were compared. The outcome parameter was death, but no death was found in either group. With the outcome parameter being sepsis, the proportion of sepsis in the “refer in” group and “walk in” group were 0.1 and 0.0, respectively. The calculated sample size number was 93 in each group using α = .05 and power of test = 0.8.
Exact probability tests and independent t tests were used to compare the characteristics between the “refer in” group and the “walk in” group. A 2-tailed P value of less than .05 was considered statistically significant. Significant therapeutic outcomes were calculated for univariate risk regression analysis to evaluate the crude effect of risk of sepsis between the “refer in” group and the “walk in” group. Multivariate risk regression analysis allowed adjustment for age, gender, and comorbidities.
Results
There were 282 DNI patients admitted in the hospital during October 2013 to March 2016. Eighteen hospitals sent patients to the central hospital. There were 152 patients in the “refer in” group and 130 patients in the “walk in” group. No missing data were found. This study encompasses patients of diverse ages and races. The duration of illness in walk-in patients was 1 to 12 days, mean 5.3 day (±2.0). Referred patients had an illness duration of 1 to 10 days. The mean duration was 5.3 days (±2.2). Dental caries, hypertension, and diabetes were a common disease in patients with a DNI, while HIV infection is very rare in DNI patients. No difference was found in gender, age, race, and duration of symptoms between the 2 groups. But there were statistical differences in the patients’ residences, health insurance, and location of the lesion in masticator space, dental caries, and malignant disease (Table 1).
Characteristics of Deep Neck Infection Patients.
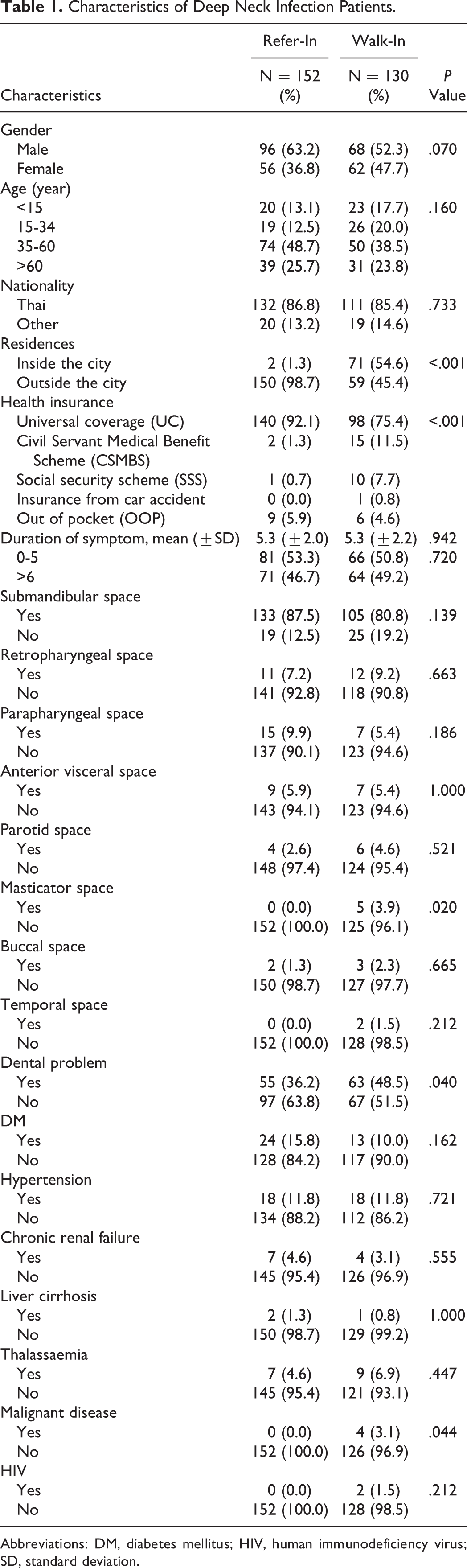
Abbreviations: DM, diabetes mellitus; HIV, human immunodeficiency virus; SD, standard deviation.
In this study, maximal follow-up time of referred patients was 52 days. Patients in the “walk in” group had a tracking time of up to 20 days. Both groups were treated by antibiotic injections and surgeries. Surgical drainage of DNI had external or intraoral surgery and could have required repeat surgery. Postoperative tracheostomy or postoperative intubation prevented airway obstruction. Other complications found in this study were sepsis, mediastinitis, pulmonary complication with respiratory failure, and death. There was no difference with regard to duration of hospital stay, medical expenses, remedy, airway management, morbidity, and mortality between 2 groups. However, sepsis was different in both groups (P = .013; Table 2).
The Results of Treatment of DNI Between “Refer in” Group and “Walk in” Group.
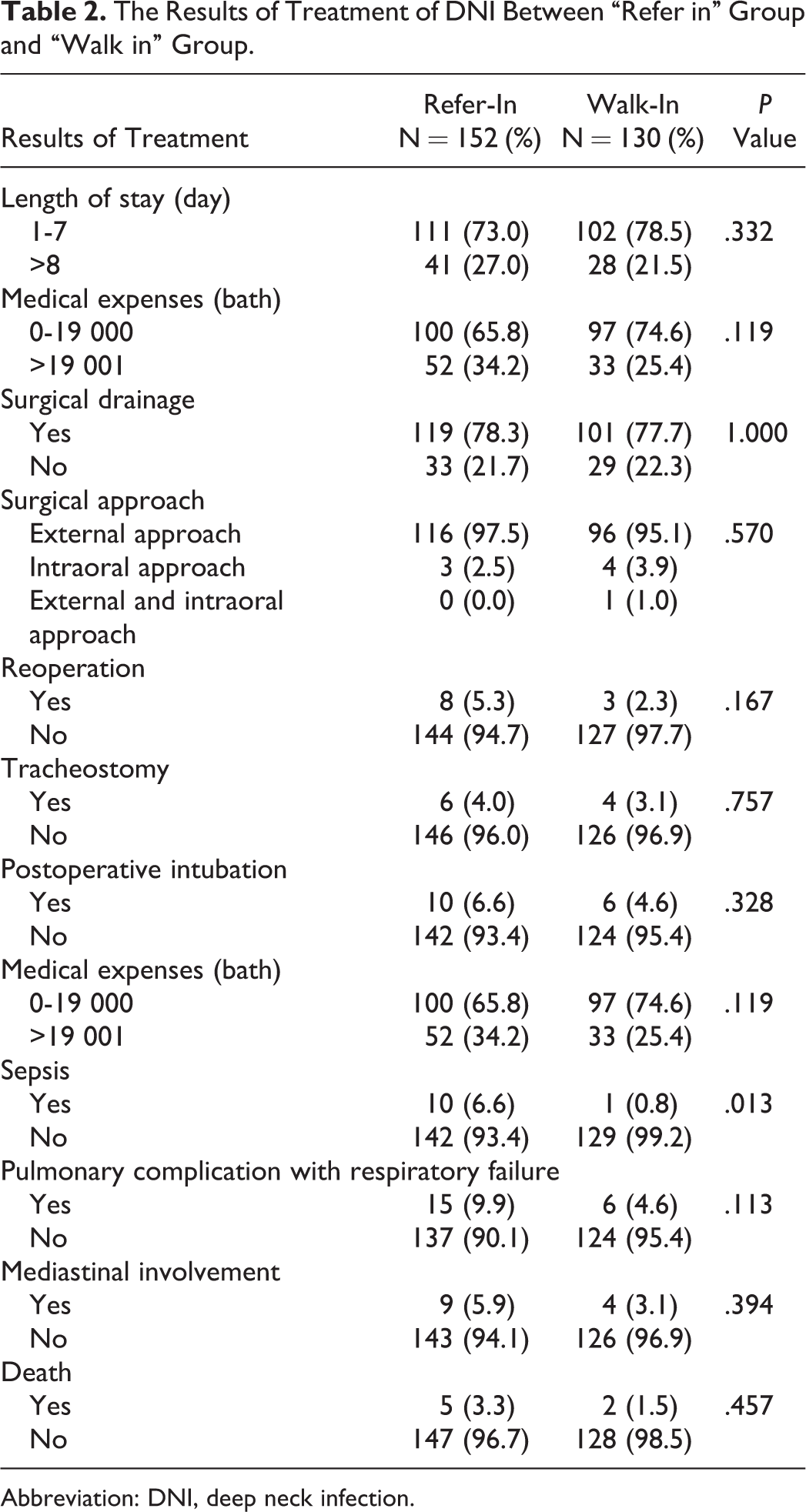
Abbreviation: DNI, deep neck infection.
The referred patients had risks to have sepsis 1.1 times more than the patients who went directly to the medical specialists (univariate analysis risk ratio [RR] = 1.1, 95% confidence interval [CI]: 0.8-1.3; P = .620). After analyzing age, gender, diabetes, chronic renal failure, cirrhosis, and dental care, it was found that the risk to have sepsis in the “refer in” group was 1.1 times more than the other group (multivariate analysis RR: 1.1, 95% CI: 0.8-1.3; P = .658).
Discussion
This study was retrospectively examined in a large number of DNI patients. Two hundred eighty-two patients attended the study. Deep neck infection patients usually see a general doctor before meeting a specialist doctor, which is common in many hospitals around the world, thus causing delayed treatment problems. But the results of treatment in referred patients were not different from walk-in patients. People in areas that do not have specialized doctors can access quality and effective medical care. Key factors that made the referred patients have good and satisfactory results of treatment were the speed of handling. When a patient arrives at a community hospital, they will receive immediate medical attention and referral. The duration of symptoms of both groups before coming to hospital was not different. The development of the referral system was the reason for the rapid transfer of patients. Ear, Nose, and Throat doctors visited and educated physicians in community hospitals to ensure the diagnosis of DNI. This also included the creation of a DNI patient care handbook and consultation system through mobile application to increase the speed of referral and treatment.
Although the result of treatment of the 2 groups was not different, the referred patients appeared to be more severe due to patients with sepsis in the referred groups having more than walk-in groups (P = .013). Sepsis represents a serious life-threatening complication of DNI. Sepsis was one of the causes of death of DNI patients. 9 Patients with sepsis died 17% to 40%. 10 -12 Sepsis is a part of systemic inflammatory response syndrome caused by infection. This study used the International Sepsis Definitions Conference to define sepsis. 13 Another study found that sepsis in DNI patient was 0.4% to 16.8%, 14 -16 but this study showed 3.9%. This study showed that DNI patients had an underlying disease and both groups of the DNI patients had no different underlying diseases. The underlying disease does not affect the mortality of patients with sepsis. 17 Most referred patients were outside the city. They did not have access to appropriate medical services. They faced a shortage of specialist medical personnel. They may lack effective medical instruments to diagnose the disease and a lack of effective drugs to control the underlying disease. Therefore, referred patients had the opportunity to control the underlying disease but that was not good enough when infection occurred, resulting in a high probability of sepsis easily setting in.
The participants in this study had limitations in access to health care for several reasons. But when it is needed to be treated in a central hospital, the referral system can send DNI patients with sepsis to the central hospital quickly. This study had good sepsis treatment results, although the number of patients with sepsis in the group of referred patients and walk-in patients were unequal. This was an opportunity to improve the effectiveness of DNI treatment. Prior to delivery of DNI patients, they should be assessed for sepsis and primary management, especially for patients with underlying diseases who are treated with sepsis differently from those who are normal. 18 Patients should be given proper antibiotics before being sent to the referral hospital because adequate antibiotic therapy in the early stages of sepsis will improve survival. 12 A delay in receiving antibiotics resulted in an increase in the death rate of patients with severe infection 19 or with the severe underlying disease. 20 Identification of the microbiologic by gram stain of the pus will help in deciding proper antibiotics. If DNI patients have septic shock, early goal–directed therapy was an approach used in patients and reduced mortality. 21 Crystalloid replacement is resuscitation targeted to a central venous pressure of 8 to 12 mm Hg. Patients should receive a vasopressor to achieve mean arterial pressure greater than 65 mm Hg, which is appropriate for systemic organ perfusion. 22 When patients arrived at center hospitals, continuous intravenous fluid delivery and vasopressor should be used to benefit in reducing the death rate of patients.
Thai public health system had major 3 health insurance. The patient being referred or treated in a hospital directly depends on the health insurance of each patient. Patients with universal coverage needed to go to the primary care hospital in their hometown first. Then, the patients would be transferred to the central hospital such as Chiangrai Prachanukroh Hospital. On the other hand, patients with Civil Servant Medical Benefit Scheme had rights to get the health service from any government hospital. Therefore, those patients would choose to go to the central hospital directly. The same applies to patients with a social security scheme (SSS) who could also get the service from Chiangrai Prachanukroh Hospital directly because this hospital is the only government hospital in Chiangrai that accepts a SSS. Therefore, both groups of the patients had different health insurance coverages.
Dental care was one of the most important causes of DNI. There was a difference in the dental problems between the 2 groups. Patients living in the city are generally “walk in” patients. And it was more difficult to provide dental care programs to the people in the city because the proportion of the population and the dental care staff in the city is more than that in the rural areas. Although there were many department stores and shops in the city, the sweet candies and food which caused dental care issues were more available to affect dental issues. In the right to treat patients, the SSS provided a limited budget (600-900 baht a year) for the oral and dental care program. Most SSS insurance patients were in the “walk in” group. Some were afraid to get the dental checkups annually because they did not want to spend over the budget. The dental examination was not very likely and can result in tooth decay.
Patients with masticator space abscesses were different in both groups, as most masticator space abscesses were caused by the degree dental care. 23 This group of patients had the same characteristics as patients with care, including masticator space abscess patients who could not open their mouths. This was a serious concern of the patients. This encourages patients to come directly to the large hospital.
It was reported that patients with head and neck cancer could present symptoms such as DNI, 24 but it was not found in this study. This study found that one patient with head and neck cancer and 3 with cancers from other parts had clinical follow-up at central hospital regularly. Therefore, these patients came to the central hospital directly when they had DNI. According to this study, the numbers of patients with cancer were different in both groups.
Lacking in this study was a randomized design, because the health insurance was limited to patients being admitted directly or transferred from community hospitals. This caused the group of patients considered to be comprised in a manner that is not the normal distribution.
Although the factors of treatment outcome in DNI patients were discussed in previous studies, most studies showed the factors relating to the underlying disease and health status of the patients. The study of the management and care of the DNI patients was not significant. The results from different countries could not be used because of the different health-care systems. Moreover, there had been no study about the effect of a referral system to the outcome of treatment DNI patients yet. The outcomes of treatment in DNI patients were not different between the referred patients and the direct patients even when they had differences in residences, health insurance, and the space of infection. Even so, the referred patients had more severe symptoms especially with sepsis. This was an opportunity to improve the effectiveness of DNI treatment.
Conclusion
The results of DNI treatment of patients between referred and walk-in were not different in terms of cost, duration of hospital stay, treatment, complication, and mortality. Deep neck infection patients at hospitals that do not have a specialized doctor will receive appropriate treatment because of the effective DNI referral system according to public health systems. However, the referred patients had more severe symptoms, especially sepsis, which is a risk factor for mortality. Therefore, sepsis care should be added to the referred patients to achieve better outcomes.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Internal Ethical Committee of Research in Human Subject, Chiangrai Prachanukroh Hospital. (Ref. no. CR0032.102/34114).
Acknowledgments
The author thanks Dr Patcharee Ruangwongroj (Department of Physical Medicine and Rehabilitation, Chiangrai Prachanukroh Hospital, Thailand) for her help in the statistical analysis. The author would like to show gratitude to Professor Dr Kittipan Rerkasem (Faculty of Medicine, Chiang Mai University, Thailand) and Professor Nathorn Chaiyakunapruek (Faculty of Pharmacy, Naresuan University, and Monash University Malaysia), who gave excellent advice for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.