
Abstract

A 60-year-old woman with a 5-month history of slow, progressive right nasal obstruction was referred to our hospital. She had no other health problems or history of nasal surgery. Nasal endoscopy showed a protruding polyp in the right middle meatus extending toward the posterior choana (Figure 1A). Computed tomography of the nose and paranasal sinuses showed a soft-tissue density with calcifications in the right maxillary sinus and a large mass occupying the right middle meatus, extending to the posterior choana (Figure 2). Right endoscopic sinus surgery (ESS) was performed under general anesthesia. An uncinectomy and middle meatal antrostomy were then performed. During the polypectomy within the maxillary sinus, a dark brownish mass was detected and removed (Figure 1B). The pedicle of the polyp was attached to the posterolateral wall of the right maxillary sinus. The origin site of the polyp was removed using giraffe forceps and curved debriders. The removed samples were analyzed for pathologic confirmation. The findings were compatible with aspergilloma and antrochoanal polyp (ACP), respectively. The postoperative course was uneventful. Complete resolution of the nasal obstruction was achieved approximately 3 weeks after the ESS.
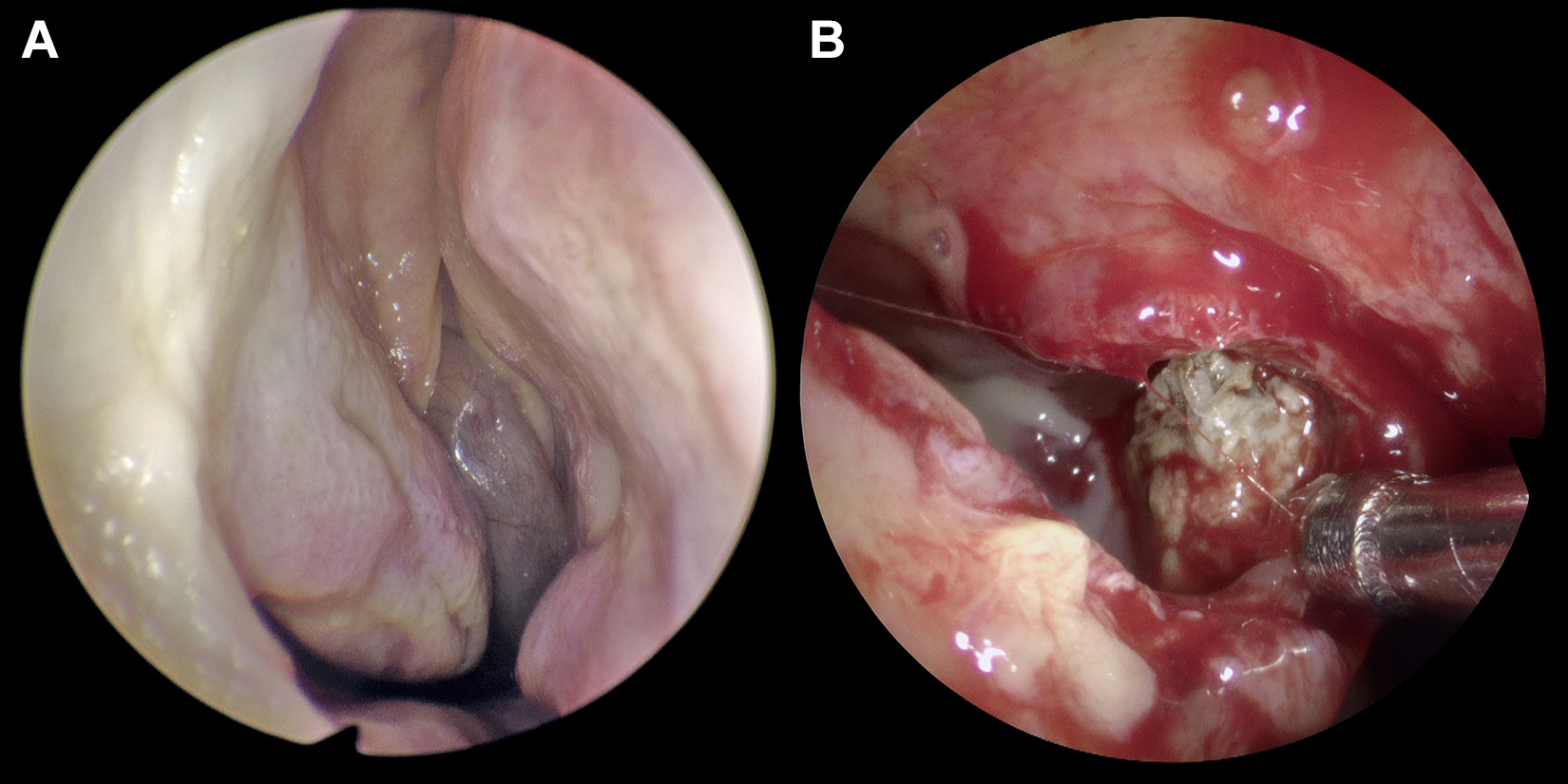
A, Endoscopy showing a protruding polyp in the right middle meatus extending toward the posterior choana. B, During polypectomy within the maxillary sinus, a dark brownish mass was detected and removed.
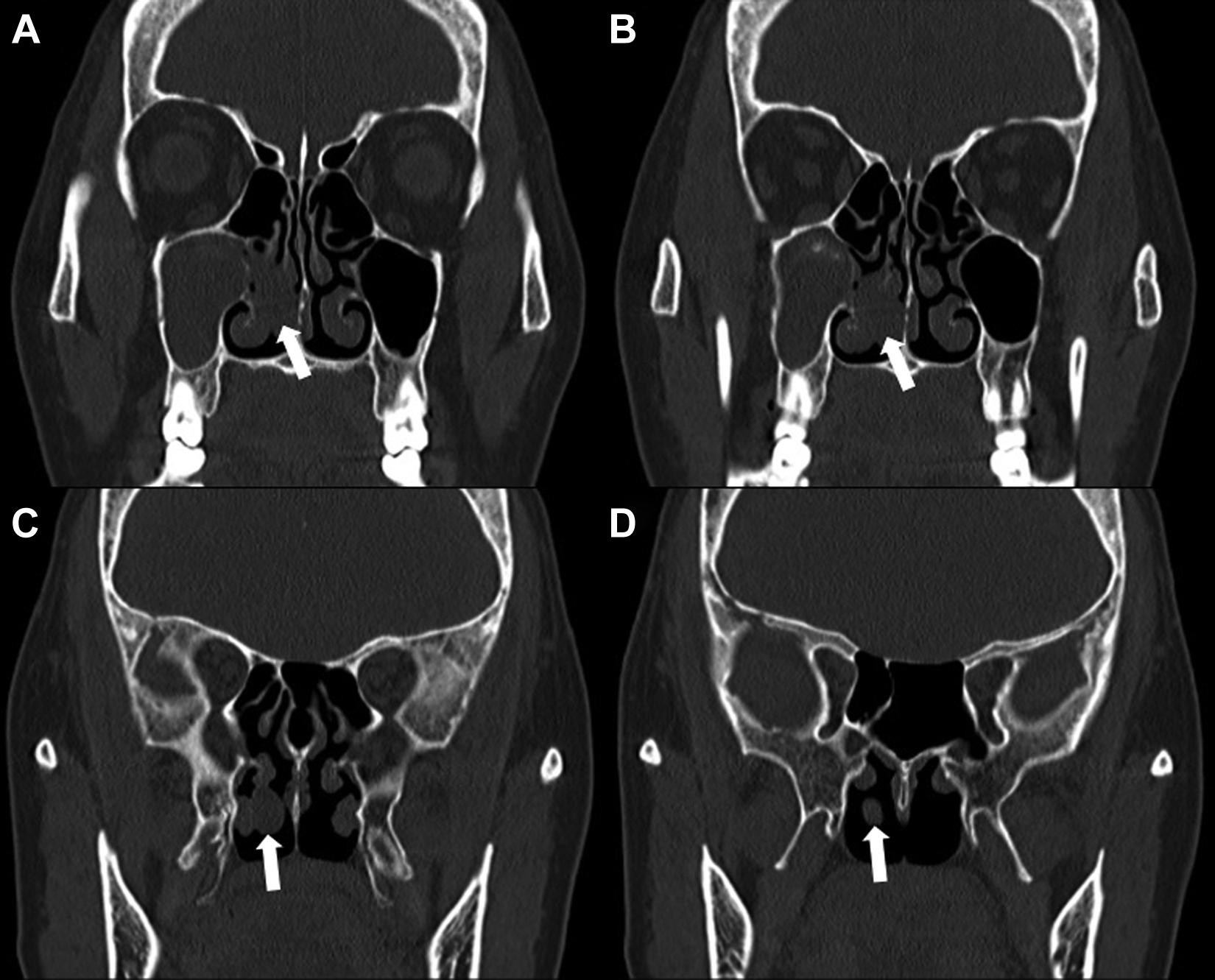
A, Coronal CT of the nose and paranasal sinuses showing a soft-tissue density in the right maxillary sinus and a large mass (arrow) occupying the right middle meatus. B, Calcifications in the right maxillary sinus and the mass (arrow). C and D, The mass (arrows) extending to the posterior choana. CT indicates computed tomography.
Unilateral maxillary opacification, a common finding in chronic rhinosinustis (CRS), may be caused by many diseases. It is often associated with conditions that require surgical intervention. In 2004, Kaplan et al investigated the etiology of complete unilateral maxillary sinus opacification in 64 patients. 1 All patients in the series were diagnosed with one of the following: CRS (without polyps; 42%), mucocele (25%), CRS with nasal polyps (18%), inverted papilloma (10%), or mycetoma (3%). In 2010, Chen et al evaluated 116 patients with unilateral opaque maxillary sinuses based on pathological conditions and clinical features. 2 The frequent diagnoses were as follows: CRS (52.6%), fungus ball (29.3%), ACP (2.6%), benign tumor (10.4%), and malignancy (5.1%). Fungus ball was the most common diagnosis in the patients after CRS. Fungus ball has recently received increased attention as a potential cause for unilateral sinus disease. When a unilateral problem is seen, one has to consider the increasing likelihood of fungal sinusitis. In the presence of isolated unilateral maxillary sinus opacification, older patients should generally be considered to have fungus balls or a neoplastic lesion, whereas younger patients with a unilateral polypoid mass are most likely to have ACP. 2
However, the concomitant appearance of an ACP and fungus ball in a unilateral maxillary sinus, such as in the present case, is a very rare event. It is difficult for clinicians to distinguish between these 2 diseases when the findings are present simultaneously before surgery. In a review of the literature, we found no previous case reports of concomitant ACP and fungus ball in unilateral CRS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.