
Abstract
Ménière disease is a disorder of the inner ear, characterized by rotational vertigo, hearing loss, tinnitus, and vegetative symptoms. The aim of the present research is to examine the effectiveness of betahistine and piracetam in the reduction of vertigo attacks in Ménière disease. To verify our hypothesis, 105 (31 male and 74 females, mean age [standard deviation], 57.4 [11.05]) adult patients with definite Ménière disease were enrolled in this investigation. Beside the analysis of the hospital records, the subjective complaints of the patients and the completed vertigo diaries were taken into consideration too. The statistical analysis was completed using the IBM SPSS version 24 software. Retrospective analysis, including a 12 years period was conducted. Based on our results, betahistine was successful in the reduction of attacks. Statistically significant decrease was achieved in frequency of dizziness (P = .000331) and vertigo (P < .00001) and in the duration of them (P = .000098), although in the mean power of them was not (P = .0887). The mean dose in the symptomatic treatment was determined as 87.5 ± 27.2 mg per day; however, there was no connection detected between the dose of the agent and the effectiveness of the symptomatic control. By using dual therapy (betahistine and piracetam), vertigo episodes appeared significantly less often (P = .027, Odds ratio: 4.9, 95% confidence interval: 1.2-20.2). Finally, it can be concluded that betahistine is effective in Ménière disease, but the daily dose of it should be set up for every patient individually. The advantage of the dual therapy was also confirmed.
Introduction
Ménière disease (MD) is a disorder of the inner ear, characterized by episodic rotational vertigo, sensorineural hearing loss, tinnitus, aural pressure, and vegetative symptoms, such as nausea and vomiting. 1 The pathophysiologic entity of the disease is the endolymphatic hydrops of the inner ear. There seem to be multifactorial causes for MD (of anatomic and genetic origin, allergy, viral infection, etc) and the exact etiology can rarely be determined in an individual patient. 2 Migraine is the most common differential diagnosis and should be thoroughly checked and excluded in every patient with MD. 3,4
It is difficult to estimate the real figures of MD, the literature reports about a prevalence of around 3.5 to 513/100 000, depending on the geographical location. 5 A strong dominance of females is presented in MD, just like in the other peripheral vestibular disorders. 6 Although the disorder is not explicitly frequent, the importance of the topic stems from the influence of the symptoms on the patients’ quality of life. The disease seems to be incurable, so the symptomatic, conservative pharmacologic management is an important issue. The main aim of the conservative treatment is to keep the patients at the lowest possible (I and II) stages of the disease and to minimize or eliminate the rate of attacks. The present investigation study was conducted to find out how steady symptomatic control can be maintained.
Possible Agents of the Conservative Therapy
Betahistine dihydrochloride
Betahistine dihydrochloride is widely used in Europe as a first-line treatment in the symptomatic control for MD, however it is not widespread in the United States. 7 Betahistine is a histamine-like drug that acts as both a partial histamine H1 receptor agonist and a histamine H3 receptor antagonist. 8 It is assumed that the efficacy of betahistine results from its vascular effects, inducing increase in blood flow of the inner ear, shown for example in guinea pig. 9 However, betahistine was also found to be effective in vestibular syndromes not related to the vascular insufficiency of the inner ear, so other effects on the central vestibular system have been also supposed. In a study of Tighilet et al, it was stated that histamine analogues increase the synthesis of the histamine, mostly through the blockade of the H3 autoreceptors. 10 The effects of betahistine were confirmed in a recently published study too. 11 According to their results, the histaminergic activity in the tuberomammillary’s neurons of vestibular neurectomized cats was significantly decreased under higher dose treatment of betahistine (2 mg/kg/d), whereas it did not occur with lower doses, nor did it work in combination with monoamine oxidase-B inhibitor selegiline (enzyme, which plays role in the catabolism of betahistine). Lower doses of betahistine had only acute symptomatic effect, but no on postural function. However, higher doses of the pharmacotherapeutic agent had control on both of them. Here, a very important clinical relevance emerges, that is, when daily doses are setup in MD, the metabolic features (slow or fast metabolism) have to be taken into consideration as well. This fact is a significant topic of a later part of our study.
The side effects of the agent are negligible, like headache, nausea, and gastrointestinal symptoms, such as distension. In case of pregnancy, where available clinical data are insufficient and allergy it is not applicable. Some generics contain lactose, so they are not recommended in lactose intolerance. 12
During the International Federation of ORL Societies (IFOS) Congress in 2017, a minimal consensus was attained and summarized in an algorithm. 13 According to their recommendation, the first line of treatment is lifestyle counselling, diuretics, and betahistine. Although several clinical studies have shown significant reduction in the symptoms of the disorder, an agreement referring to the effectiveness and the advantages of the treatment is still to be obtained. 14
Nootropic agents
Nootropics are widely used in our clinical practice in the conservative treatment of MD. The possible effect of them is complex such as vasodilator effects, influence on the rheologic quality of blood, and influence over the blood cells. 15 The application of these agents is based more on experience than evidence, but the treatment seems to be effective. 12 One admissible indication of nootropic use is the symptomatic treatment of peripheral vertigo. Earlier it was also found that dual therapy is more efficient in the treatment of peripheral vestibular disorders than the betahistine monotherapy. 16
Patients and Methods
In the course of our research, the complete documentation of 105, clinically diagnosed definite patients with MD, being presently under constant monitoring, was analyzed. The usual monitoring periods were 56.8 ± 31.5 months, with 5 checkups in the process on average.
Patients were included on the basis of the diagnostic criteria for MD in accordance with the diagnostic criteria of the Committee of the Bárány Society. 17
Beside the assessment of the complete clinical case history (the medical letters of about 1098 attendances at our otoneurologic center), the subjective report of the patients and vertigo diaries about the symptoms, especially those of the attacks, were taken into consideration too and contrasted to the characteristics of the conservative medication since the previous checkup. Patients were divided into 3 grades based on the rate of attacks and the various complaints in the attack-free period (grade I: rare attacks, II: severe and frequent attacks, III: severe constant hearing loss, disabling balance problems, severe attacks). The distribution of the patients between the 3 groups is as follows: 54 patients in grade I, 44 patients in II, and 7 patients in III. The dose of betahistine was set up for every patient individually, based on the symptoms since the previous medical checkup, using anamnestic data and vertigo diaries.
The research project had the consent of Semmelweis University Regional and Institutional Committee of Science and Research Ethics: 47/2018.
The statistical analysis was completed using the IBM SPSS version 24 software. As most of the studied parameters did not show normal distribution, we applied nonparametric tests. The correlation between the variables was determined using the Fisher and 1-way analysis of variance tests, the significance level was specified as P < .05. To illustrate our results, survivorship curves, the so-called Kaplan-Meier curves were included as well. Moreover, the connection between the different symptoms and the therapy was analyzed using the log-rank test as well.
Results
Epidemiological Surveys at Our Tertiary Referral Otoneurologic Centre
The mean age of the patients was 57.38 years (11.07 standard deviation) and the age distribution in MD peaked in the middle-aged groups (40-60 years). Group of patients is consisting of 31 (29.5%) males and 74 (70.5%) females, so it follows that a strong dominance of females is presented in MD, just like in the other peripheral vestibular disorders. In this population, most of the patients having MD were found in the age-group of 61 to 70, however, the frequency of occurrences rises from the middle of the age lines unequivocally. It is a remarkable fact which is important because this interval covers the patients’ most important active years economically.
The Monitoring of the Subjective Strength of Symptoms Recorded in the Vertigo Diaries
As shown in Table 1, by completing the vertigo diaries, our patients can take account of the characteristic of their symptoms. In cases of the vertigo attacks, the duration of the episodes is specifically important. We can talk about MD attack only if the vertigo is described as rotary and if its duration lasts at least 20 minutes long (according to the criteria of Bárány Society).
Vertigo Diary Used in our Clinical Practice.
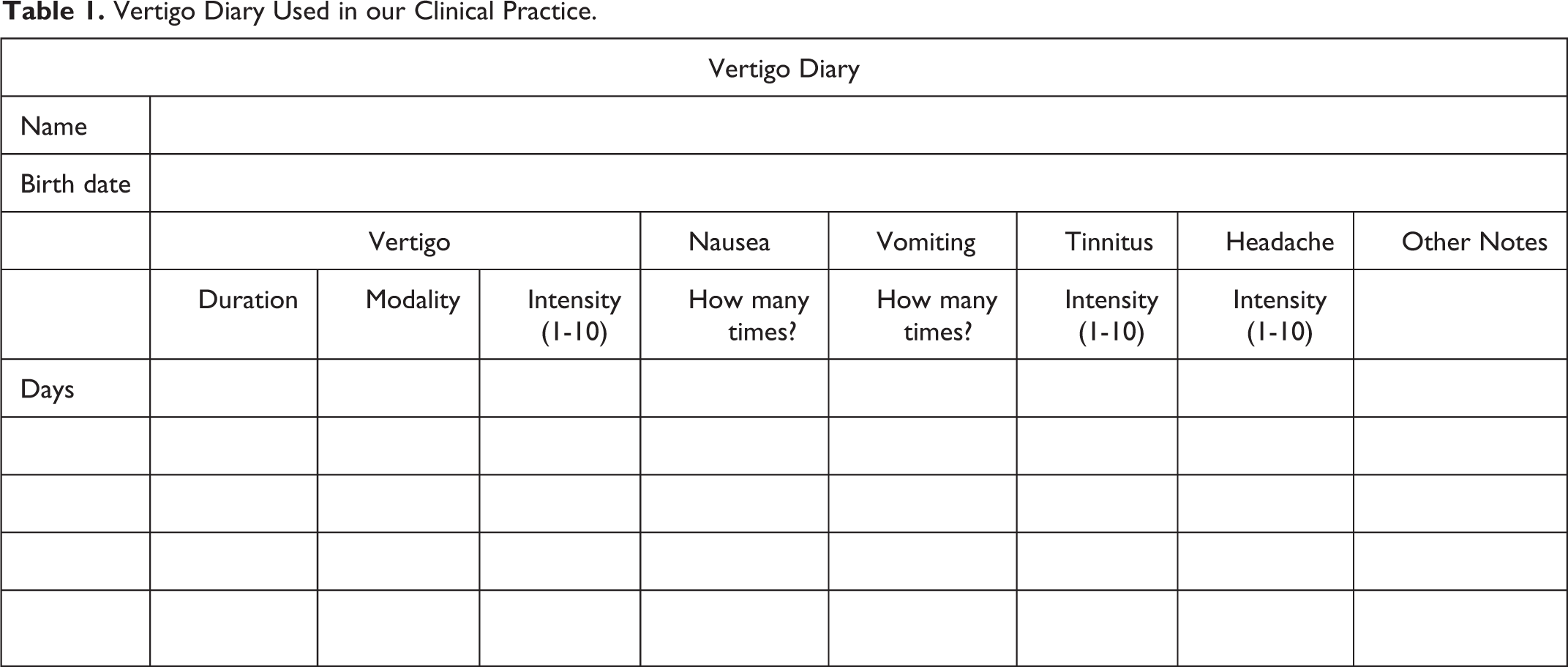
The typical characteristics of the symptoms were defined using the completed diaries, collected from our patients with MD. According to the diaries, our patients (n = 105) reported about 1552 episodes of dizziness and 52.7% of these episodes can be described as rotational vertigo, the others were tilting sensations with Tumarkin crisis but not imbalance or lightheadedness. The frequency of the episodes was 2.35 ± 1.4 attacks per month on average. The intermittent attacks of vertigo lasted 6.16 hours, and their strength was around 5.46 ± 1.7 on a scale of 1 to 10. The mean value of the intensity of the tinnitus appeared to be 4.46 ± 2.3 on a scale of 10, and headache was associated with the episodes in 82% of the cases (mean intensity: 3.43 ± 2). The associated vegetative symptoms are important too: nausea appeared in 98.1%, while vomiting in 89.5% of the cases.
The vertigo diaries are helpful in the analysis of the patients’ subjective symptoms: we can make sure that the characteristics of the attacks meet the requirement of the criteria and using the diaries, the observation of the effectiveness of the pharmacologic treatment is easier as well.
The Effectiveness of Betahistine Therapy
We wanted to clarify the potential role and efficiency of betahistine in the control of the vertigo attacks and to find whether there is a connection between the dosage of the agent and the symptomatic control. To accomplish it, 3 analyses were carried out.
Based on the completed vertigo diaries, the following analysis was carried out:
Due to the treatment with betahistine in an adequate dosage, the decrease in the frequency of the dizziness was 1.5/month on average; while in the vertigo attacks, 2.1/month on average. The duration of the episodes was reduced too (2.9 hours on average), although, on the other hand, the reduction of the mean power of the episodes of vertigo was not significant (0.3 on a scale of 1 to 10). Our results imply that that oral administration of betahistine has major effects on the frequency and duration of vertigo and dizziness, but no explicit effect on the intensity of the vertigo episodes (Table 2).
Changes for Betahistine Treatment in the Parameters of Vertigo.a
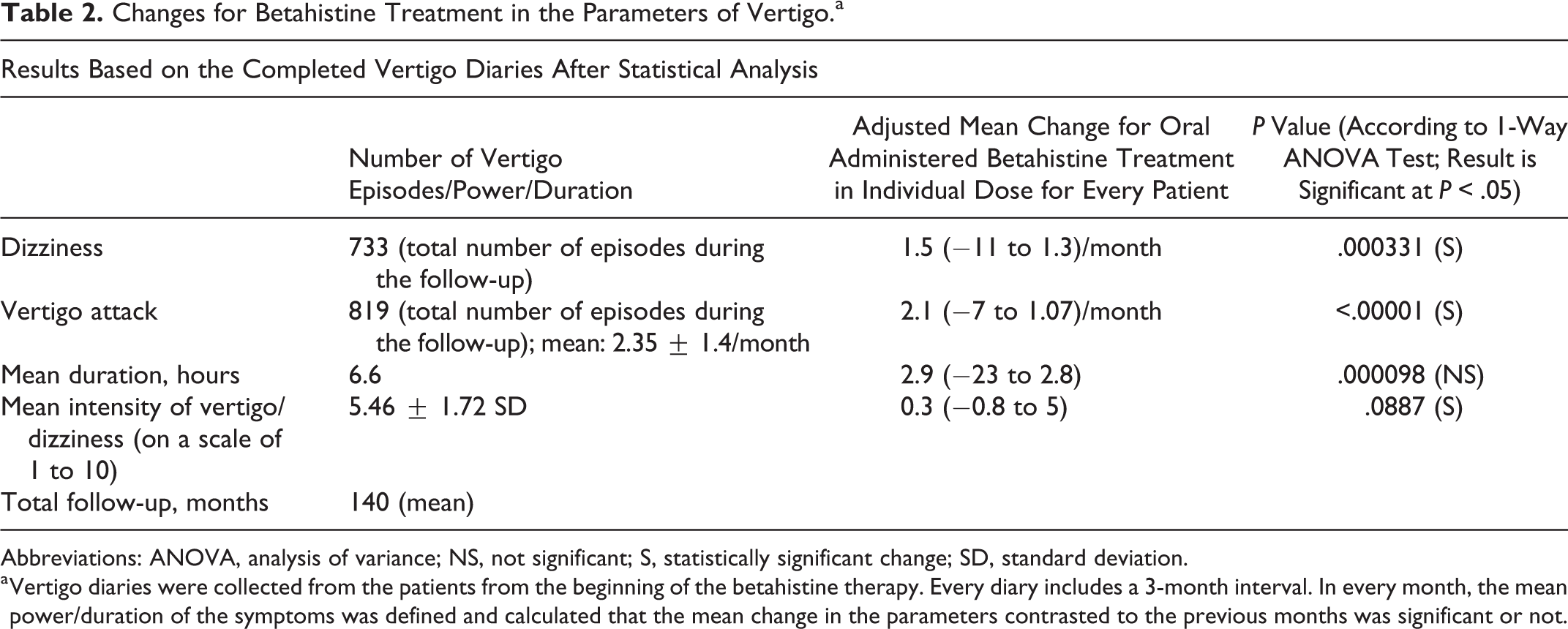
Abbreviations: ANOVA, analysis of variance; NS, not significant; S, statistically significant change; SD, standard deviation.
a Vertigo diaries were collected from the patients from the beginning of the betahistine therapy. Every diary includes a 3-month interval. In every month, the mean power/duration of the symptoms was defined and calculated that the mean change in the parameters contrasted to the previous months was significant or not.
After processing the data by the Kaplan-Meier analysis, the following results came up:
As shown in Figure 1, under betahistine treatment, the vertigo attacks appeared significantly (P = .001; Odds ratio: 2.75 [95% confidence interval, CI: 1.068-4.442]) less frequently than among those patients who were not treated (because of allergy, pregnancy, or arbitrary reducing of the dosage of the medicine). It is very different when the beginning of the therapy was performed, not all patients were on no treatment for the first 60 to 70 days. The therapy was initiated after the first complete otoneurologic examination at our clinic. Of course, the spontaneous reduction of the symptoms could be never ruled out, which is always a limitation.
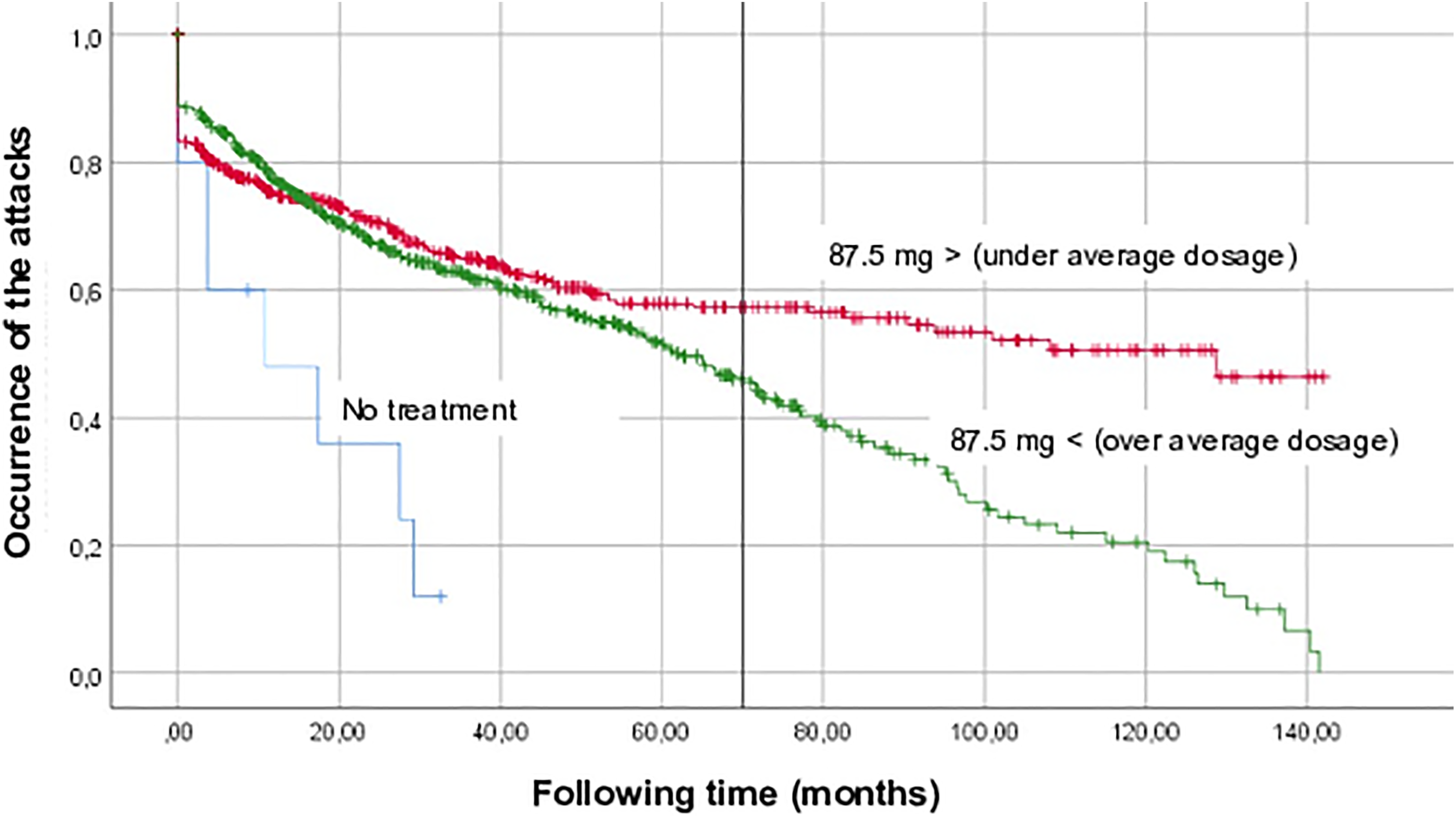
Connection between betahistine therapy and vertigo attacks. Please note that the number of the cases does not mean the number of the individuals, but it consists of the attendances (5 controls per patients on average). Using the diaries, appearance of vertigo attacks was observed. In SPSS, the number of events (ie, vertigo attack) that happened at time (following time) was determined as follows: 0, if 3 or less attacks/month and 1, if more than 3 attacks/month. To analyze the connection between the dose of betahistine and the control of attacks, the average daily dose of the agent was determined (87.5 ± 27.2 mg per day) and patients were divided into 2 groups according to it: treated with betahistine under and over the average dosage. The third group consists of the patients who were not treated (allergy, pregnancy, or arbitrary reducing of the dosage of the medicine).
Categorical analysis (ie, treatment with betahistine or not and attack appeared or not) was carried out too (using Fisher exact test). The P value was determined as .0001, which implies a strong statistical difference as well (more attacks in case of no treatment and less in treated patients).
The mean dose in the symptomatic control has the appearance of 87.5 ± 27.2 mg per day, the minimal average dose was determined as 24.6, while the maximal as 170.5 mg per day. However, statistically no apparent connection was found between the dose of the agent and the symptomatic control. Accordingly, it is important to set up the dosage for every patient individually. The most frequent dosing pattern characteristic was established as 144 mg, broken down into 48 mg 3 times a day.
Betahistine Plus Piracetam Dual Therapy
We wanted to investigate the advantages of the dual therapy (betahistine plus nootropics) over the betahistine monotherapy. Our results are the following:
Drug effects were studied based on the occurrence of vertigo attacks during following time. During Kaplan Meier analysis, 2 cohorts of patients were created based on whether a patient was treated with monotherapy or dual therapy. From the curves (Figure 2), it can be stated that in case of dual therapy using betahistine in individual dose and 2400 mg piracetam (1-1-0 tablets a day), the vertigo episodes appeared significantly less often in comparison with those treated by betahistine only. The vertical axis (y) represents the probability of the defined event (ie, vertigo attack): at 1.0 the probability of attack-free period is 100%, and when the curve drops down the occurrence of vertigo attacks is more frequent. When compared using the logistic regression, a statistically significant difference was observed between the betahistine monotherapy and betahistine plus piracetam dual therapy (P = .027; Odds ratio: 4.9 [95% CI: 1.2-20.2]), which also implies that attacks were occurred less often in case of dual therapy.
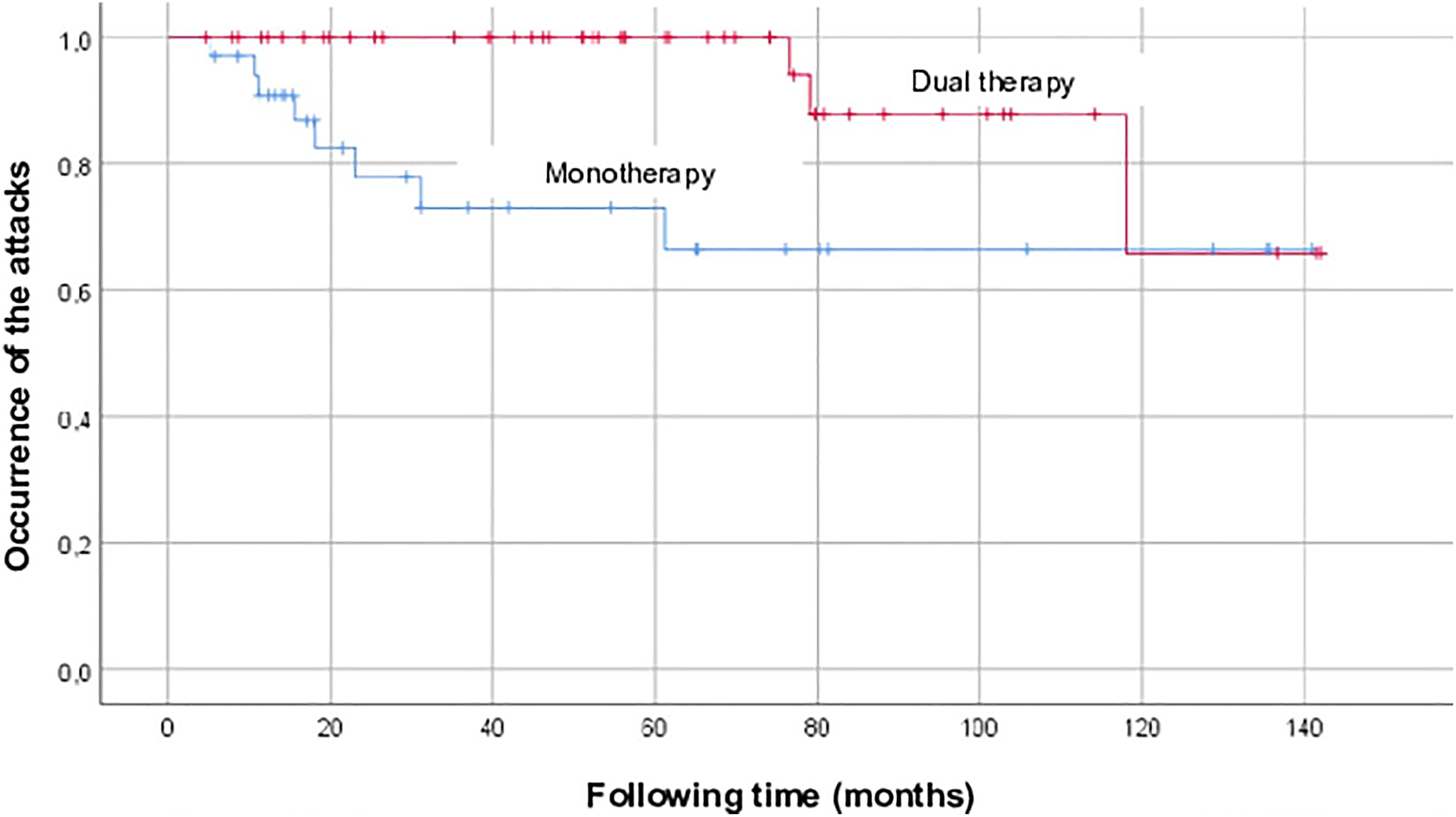
Comparison of the effectiveness of the monotherapy and dual therapy. In SPSS, the events that happened in time (following time) were defined as appearance of vertigo attacks, monotherapy means that patients received betahistine only (n = 54 patients), while in case of dual therapy (n = 51), betahistine (in individual dose) + piracetam (2400 mg per day) was used.
The application of piracetam in case of 51 patients was necessary, because these patients belong to the grade II and III groups; and according to our clinical practice, the use of nootropics is recommended in case of worse vestibular status (II and III grades, severe and frequent attacks).
Discussion
A broad range of therapies has been proposed for MD, however, a consensus has yet to be made considering the effectiveness and advantages of them, and the evidence of their benefits is still to be verified. 14 This article confirms that betahistine in appropriate daily dose, especially in combination with nootropics is a potent, noninvasive and safe treatment option. In 70% of our patients with MD, vertigo attacks have been resolved, symptom-free periods could be achieved. Betahistine was effective on all individual groups; however on the grade II and III groups, it is often less effective, that is the reason why using of nootropics is important in that cases. Although, the mean dose of betahistine on the 3 groups was not significantly different, because it has been set up for every patient individually.
Admittedly, there are some limitations of our study. Vertigo diaries, which are filled by the patients with MD, show a subjective judgment of the patients about the strength of vertigo and tinnitus on a scale of 1 to 10. Nevertheless, vertigo diaries are helpful in the analysis of patients’ subjective symptoms: We can make sure that the characteristics of the attacks meet the requirement of the criteria and using the diaries, the monitoring of the effectiveness of the pharmacologic treatment is easier as well. The diaries are also helpful to decide that changes in the treatment, involving more invasive procedures, such as intratympanic dexamethasone or gentamycin are necessary or not. Some parts of the study were retrospective, but this way of investigation facilitates the long-time following of patients, which is important because of the chronic nature of the disorder and the long-time efficiency of the conservative therapy. Nevertheless, using the vertigo diaries, prospective approach has been also realized. There was also no placebo involved in this study. The application of placebo came not into consideration, because in our opinion, it is not ethical to withdraw the symptomatic control from some patients with MD. On the other hand, due to the nature of placebo-controlled trials (short-term application of the agent, the ranking of the patients into random groups according to the applied doses), the validity of their results is limited. The features of the trial are not suitable for the basic principles of the treatment. However, our results are encouraging.
Concerning placebo, 3 years ago, a double-blind, randomized, and placebo-controlled trial was carried out in Germany. According to their results, the appearance of vertigo attacks in patients with MD did not differ between the 3 groups, 1 treated with low dose (2 × 24 mg/d), 1 with high dose (3 × 48 mg) betahistine, and the third with placebo. 18 Considering these clinicians’ conclusion drawn from their research, that is, betahistine has no greater effects than placebo, so it is not worth using betahistine in the clinical practice, the study presented by our team has no interest. Our point of view is a little bit different, based on our clinical data. First of all, the ranking of patients with MD into random groups according to the applied doses does not meet the requirements of the characteristic of the treatment. According to our clinical expertise and to the article referenced earlier, 10 the daily dose of betahistine should be set up for every patients individually, this fact could be explained by the characteristic of the metabolism of betahistine (low or fast metabolizers), so the dosage needed for the stage without complaint is very different. Of course, in the clinical practice, the features of the metabolism cannot be traced for every individual, this is why the long-term following, and the necessary changes in the doses of the treatment are of great importance. On the other hand, during the placebo-controlled trial maximally 144 mg (3 × 48 mg/d) betahistine was administered. There are also some limitations regarding the follow-up time, too. Their maximal period was 9 months. Because of the chronical nature of the disease and the fluctuating, episodic pattern of the symptoms, the long-term following and effectiveness of the pharmacotherapeutic agent are primary. In our analysis, the mean follow-up time of the individuals was specified as 56.8 ± 31.5 months on average, maximum with the longest monitored patients was 143 months (about 12 years).
In a former publication of Strupp et al, the dose-dependent effect of betahistine in the control of vertigo attacks was identified. 19 According to our analysis, statistically no apparent connection was found between the dose of the agent and the symptomatic control, so it is important to set up the dosage for every patient individually. Previously, it was found by Mira et al that betahistine has a great effect on frequency, duration, and also intensity of vertigo attacks. 20 According to our results, oral administration of betahistine has major effects on the frequency and duration of vertigo and dizziness, but no explicit effect on the intensity of the vertigo episodes.
According to the vertigo diaries, the most tormenting symptoms are the vertigo attacks, so the symptomatic treatment of these episodes seems to be prominent. The second most determining symptom is the tinnitus, so it is important to talk about that too. The high rate of headache reported in the diaries hints that among these cases, a great number of vestibular migraine is hidden. According to the recommendation of the Bárány Society when criteria for MD are met, it should be diagnosed as MD even if symptoms of migrainous headache are presented during the vertigo attacks. Only if 2 types of vertigo, 1 typical for MD and 1 for vestibular migraine, occur at the same patient, is it possible to diagnose the 2 disorders simultaneously. This statement can be supported by the fact that migraine symptoms such as headache, photophobia, and migraine auras frequently appear during vertigo attacks of MD. 4 Nevertheless, none of the patients in the examined population met the criteria to diagnose the co-occurrence of MD and vestibular migraine.
Betahistine, the agent widely used in Europe as a first-line treatment for MD was successful in the conservative treatment of the symptoms according to our observations. The mean dose in the symptomatic treatment was determined as 87.5 ± 27.2 mg per day. Although in the everyday practice we can see relationship in some of the cases between the dose of betahistine and frequency of attacks, there is not statistical correspondence between the dose of the agent and the symptomatic control. Nonetheless, when administering dual therapy (betahistine and piracetam), the vertigo episodes appeared significantly less often as compared to cases treated by betahistine only. The control of vestibular symptoms was significantly better among the treated patients, this may indicate the efficiency of the nootropics; however, it is questionable whether is more beneficial to use them in a tablet form or as intravenous infusions.
In what follows we would like to propose our own guidelines for the use of 2 basic agents of the conservative medical management. An initial dose of 74 mg (3 × 24 mg) betahistine is appropriate at first. But because there are a lot of influential factors, the dose of betahistine should be determined and set up individually, what is giving the explanation for the importance of the patients’ following. To succeed in achieving this well-managed patients’ following, vertigo diaries are important and quite useful. Continuously filling in and managing the vertigo diaries is a cognitive behavioral therapeutic pathway. It benefits the patient because they feel more in control of their own illness, but it also benefits the treating doctor because this way—with adequate patient education—the modification and tweaking of the dosage can be done by the patients themselves. Beside the individual dosing characteristic, it is also important that in lower stages (especially in grade I) in symptom-free periods reduction in the daily dose is possible, and in symptomatic periods just as easily increased until another symptom-free period is achieved. Based on our expertise, a maximal dose of 144 mg per day could be applied without any adverse effects, these doses were well tolerated. In case of advanced stages (grade II and III), the use of nootropics (2400 mg piracetam per day) as adjuvant therapy is highly beneficial and recommended.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by EFOP-3.6.3-VEKOP-16-2017-00009 Project for Scientific Research from the Ministry of Human Resources, State Secretariat for Higher Education, Hungary.