
Abstract

A 53-year-old man was diagnosed with p16-negative oropharyngeal squamous cell carcinoma, cT4bN2bMb, stage IVb. He received definitive concurrent chemoradiotherapy (CCRT) with conventional daily fractionation (2 Gy per day) radiotherapy (RT), which was later shifted to hyperfractionated mode (1.2 Gy twice a day) because of poor response. The total RT dose was 74.8 Gy and the concurrent chemotherapy was weekly cisplatin and 5-fluorouracil. Partial response was achieved and because of this poor condition, the patient did not undergo salvage surgery. However, the tumor progressed 5 months after completion of the CCRT was finished. Thus, the patient was enrolled into the MEDI-4736 clinical trial and received single agent anti-programmed death ligand 1 (PDL1) immunotherapy, durvalumab, every 2 weeks for total 21 doses. The optimal response that was achieved was stable disease (Figure 1A). During anti-PDL1 therapy, the patient presented with a rapidly growing exophytic tumor with necrosis and airway compromise (Figures 1B and 2A). After withdrawing from the clinical trial, hyperfractionated RT was again administrated to the growing tumor (total dose of 55.2 Gy). Rapid shrinkage of the neck mass was observed within 2 weeks after starting RT. Cetuximab was added to the treatment in the middle of RT and persisted was used consistently as maintenance therapy for 3 months. Complete resolution of the tumor was observed with relapse-free complete remission for the past 2 years until now (Figures 1C and 2B).

Contrast-enhanced axial computed tomographic scan of the (A) neck metastatic tumor, which achieved disease stability after 10 months of immunotherapy, (B) rapid tumor enlargement with airway compromise developed during the immunotherapy trial, and (C) complete remission of the neck tumor after receiving immunotherapy followed by hyperfractionated radiotherapy.
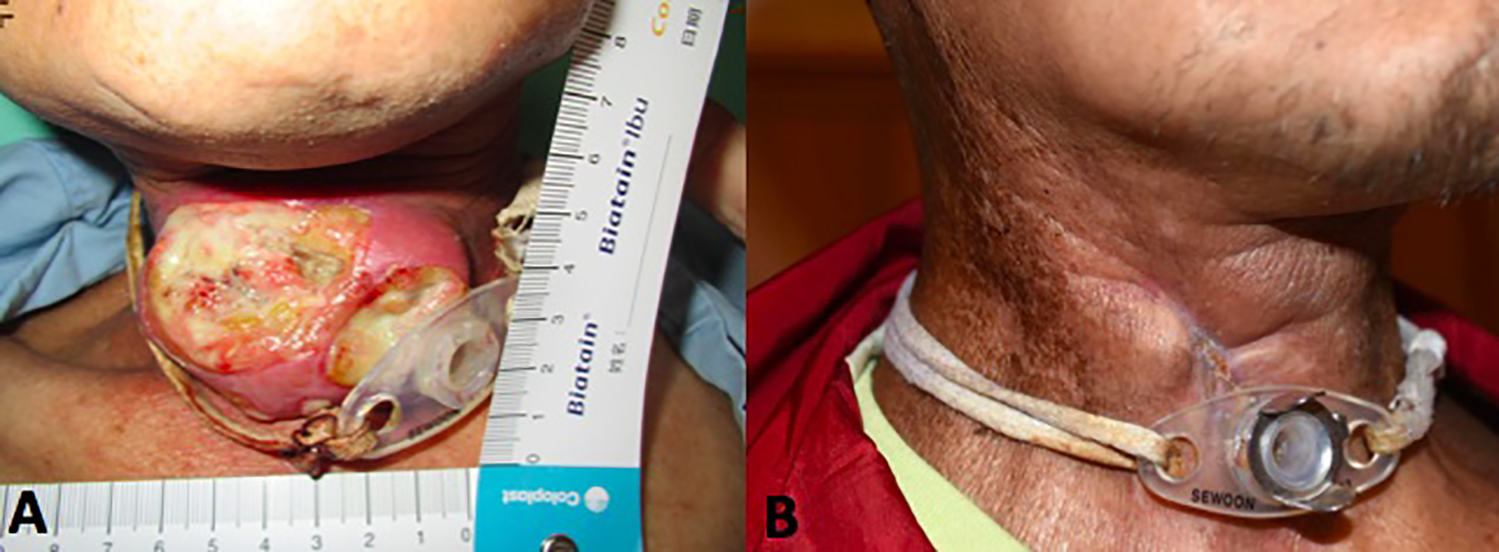
A, Exophytic tumor with necrosis and airway compromise that develop during the immunotherapy trial (B) complete remission of the neck tumor after receiving immunotherapy followed by hyperfractionated radiotherapy.
Recent advances in immune checkpoint blockade (ICB) therapy for squamous cell carcinoma of the head and neck have brought new hopes into this field. The overall response rate of anti-PDL1 agents was approximately 10% to 15%, 1 which is rather limited. From reviewing preclinical studies, we understand that combined immunotherapy and RT might have synergistic effects by increasing tumor-antigen presentation, the expression of immune checkpoint molecules expression and tumor microenvironment modulation. 2 However, from bench to bedside, uncertainty remains regarding the dose per fraction, irradiation volume, and timing of RT. A variety of clinical trials testing combined RT and immunotherapy are under active enrollment. 3 For this patient, single-agent anti-PDL1 therapy achieved prolonged results (10 months) but in stabilizing the disease. Hypofractionated stereotactic body radiotherapy is considered the most promising mode of RT to be combined with immunotherapy. 4 We adopted the reirradiation strategy with hyperfractionated RT which resulted in a remarkable response. We hypothesize that the anti-PDL1 treatment sensitized and reversed the growth of RT-resistant tumor cells. The use of cetuximab may have also contributed to disease control through antibody-dependent cell-medicated cytotoxicity.
In summary, our patient achieved long-term disease control through anti-PDL1 treatment followed by hyperfractionated RT despite having a radiation-resistant and platinum-refractory tumor. We postulate that the ICB treatment played a role in radiosensitization. The optimal method of delivery of ICB and RT combination still warrants further study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.