
Abstract

Thirty-seven-year-old man came to our attention with a 2-month history of painless right neck mass and fatigue. Neck ultrasound showed a 2.5-cm wide solid mass in supraclavicular right fossa and multiple enlarged lymph nodes at right neck levels III to IV. Otolaryngological examination, even with narrowband imaging, was negative except for the neck mass. Fine-needle aspiration cytology (FNAC) revealed high-grade epithelial malignancy. Total body computed tomography (CT) evidenced multiple right cervical enlarged lymph nodes at levels Ib to II, a 5-cm wide packet at levels IV to V and few enlarged lymph nodes in mediastinum (Figure 1). Abdomen, retroperitoneum, and central nervous system were negative. A positron emission tomography was performed in the hypothesis of nodal metastases from unknown primary. It showed elevated radioactivity in the neck and mild activity in mediastinum and right oropharyngeal tonsil. Intraoperative frozen section on cervical node biopsy showed epithelial malign neoplasm, so we proceeded to panendoscopy with multiple biopsies, tonsillectomy, and right neck dissection as per protocol for unknown primary tumor of the head and neck. Definitive histology on mucosal biopsies was negative, while nodal dissection pathology and immunohistochemistry were consistent with embryonal carcinoma. Laboratory studies revealed a serum beta-human chorionic gonadotropin (β-HCG) of 5.1 mUI/mL (normal: β-HCG < 2.6 mUI/mL). Urological evaluation showed normal testis. Scrotal and testicular sonography showed atrophic left testicle with macrocalcification (Figure 2) and 2 small nonpalpable nodules (4 and 5 mm), but hard at elastography, under the tunica albuginea (Figure 3), consistent with a burned-out testicular tumor. The patient underwent orchiectomy and subsequent chemotherapy and is now disease-free at 2-year follow-up.
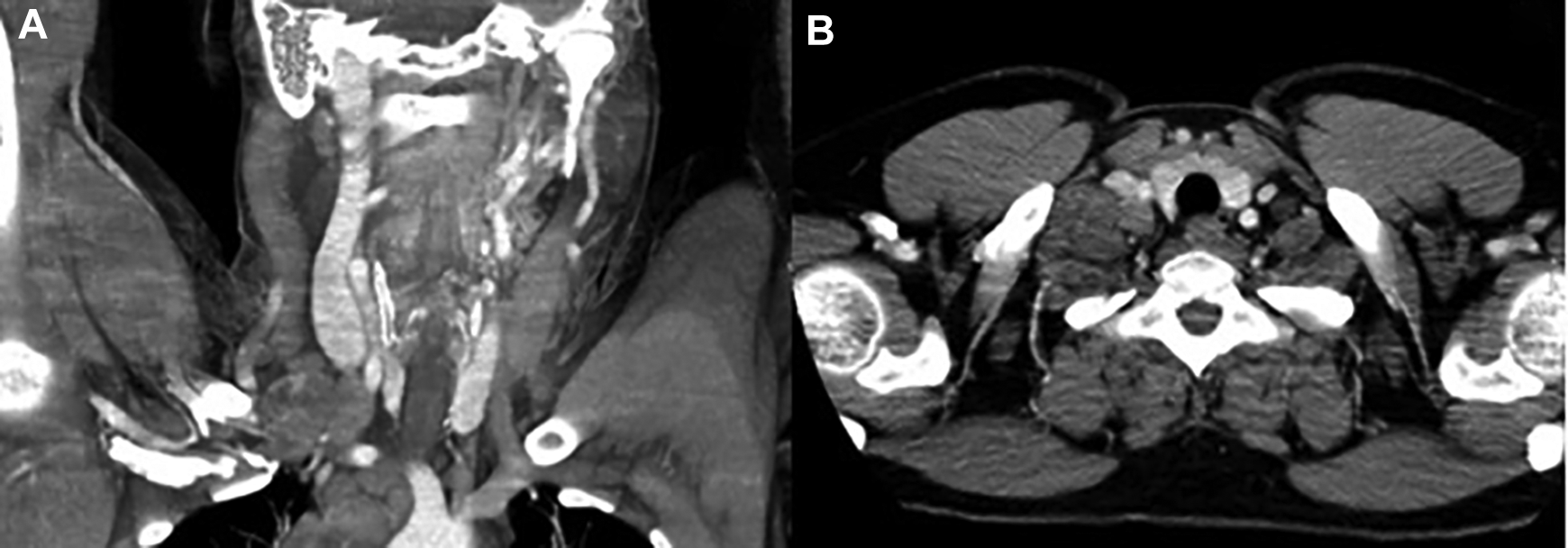
Coronal (A) and axial (B) computed tomography images showing a 5-cm packet at levels IV and V of the right neck.
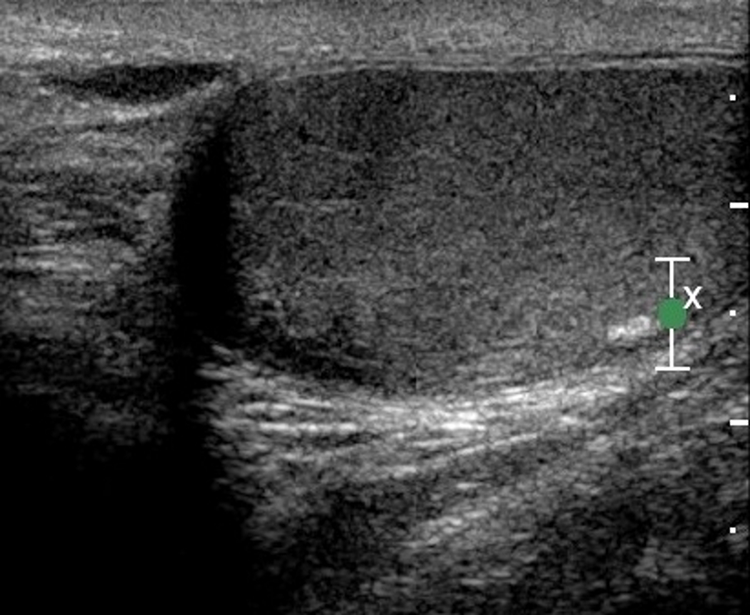
Ultrasound images of the left testicle showing macrocalcification under the tunica albuginea.
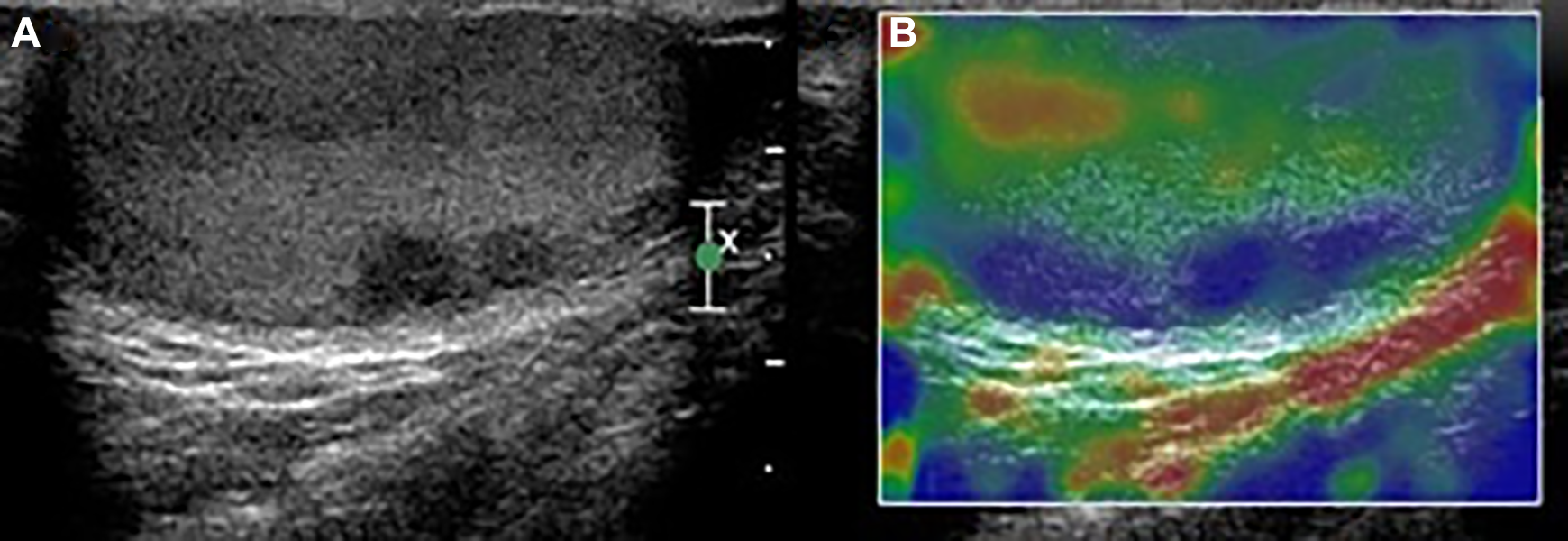
Ultrasound (A) and elastography (B) images showing 2 small hyperechoic, nonvascularized, elastographically hard nodules under the tunica albuginea.
Germ cell neoplasms are relatively uncommon but highly curable when recognized and treated properly. They most commonly present as a testicular mass and have high tendency to hematogenous spread; thus, more than 70% of patients have metastases at the time of diagnosis. Usually they develop retroperitoneal lymph node metastasis, then spread into the thoracic region and reach the cervical region finally. 1 Burned-out testicular tumor is a rare form of testicular germ cell neoplasia (2% among testicular cancers). 2 It indicates a testicular tumor undergoing spontaneous and complete regression and presenting by its distant metastasis. Since the first description, 3 urologists reported few cases with cervical involvement, usually with simultaneous retroperitoneal lymph nodes that drove to investigate for a testicular primary. The diagnosis is sonographic and histological. 4 Histological features include scar formation, intratubular calcifications, lymphoplasmacytic infiltrate, and testicular atrophy. 5 Metastasis in the neck first prompt the clinician to investigate for possible primary tumors of the head and neck. 6 In its absence, FNAC plays a key role in the initial workup of a neck mass; however, the cytological features of germ cell tumors are indistinguishable from those of poorly differentiated malignancies such as carcinoma, melanoma, or lymphoma. Furthermore, immunohistochemistry is fundamental in the diagnosis of metastatic germ cell tumors. Excisional biopsy is then required. 7 In our case, the frozen sections and the preoperative imaging have led us to think about an epithelial cancer of unknown origin. Only definitive immunohistochemistry revealed the presence of an embryonal carcinoma.
In the previous literature, several cases of burned-out tumors are reported, but usually the presence of retroperitoneal masses guided the diagnosis to the testicular origin. 2 -5 The presence of a cervical mass as the only initial clinical sign of disease had also been reported, 4,6,8 but the abdominal CT scan allowed for the identification of retroperitoneal masses; therefore, a possible testicular origin was considered. In young male with laterocervical node swelling, the possible testicular origin should be considered despite a normal physical examination of the testis and the absence of retroperitoneal involvement on imaging. An ultrasound of the testis should be performed, as it is the only examination that could exclude a diagnosis of burned-out testicular tumor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.