
Abstract

A 65-year-old man without significant medical history presented with a 5-year history of a slowly enlarging, painless, midline mandibular mass. He denied pain, paresthesia, dysphagia, or difficulty breathing. Clinical examination revealed a nontender expansion of the anterior mandibular alveolus associated with extrusive displacement and increased mobility of the anterior teeth. The overlying mucosal was slightly erythematous.
Panoramic radiograph showed a multilocular radiolucent lesion extending from the left first molar to the right second premolar, causing root resorption of the left canine and premolars (Figure 1A). Computed tomography of the face showed a multicystic internal structure with presence of coarse bony septa, giving the appearance of a honeycomb pattern (Figure 1B and C). The lesion has caused extensive expansion and thinning/perforation of the buccal and lingual cortical plates. Incisional biopsy revealed an ameloblastoma.
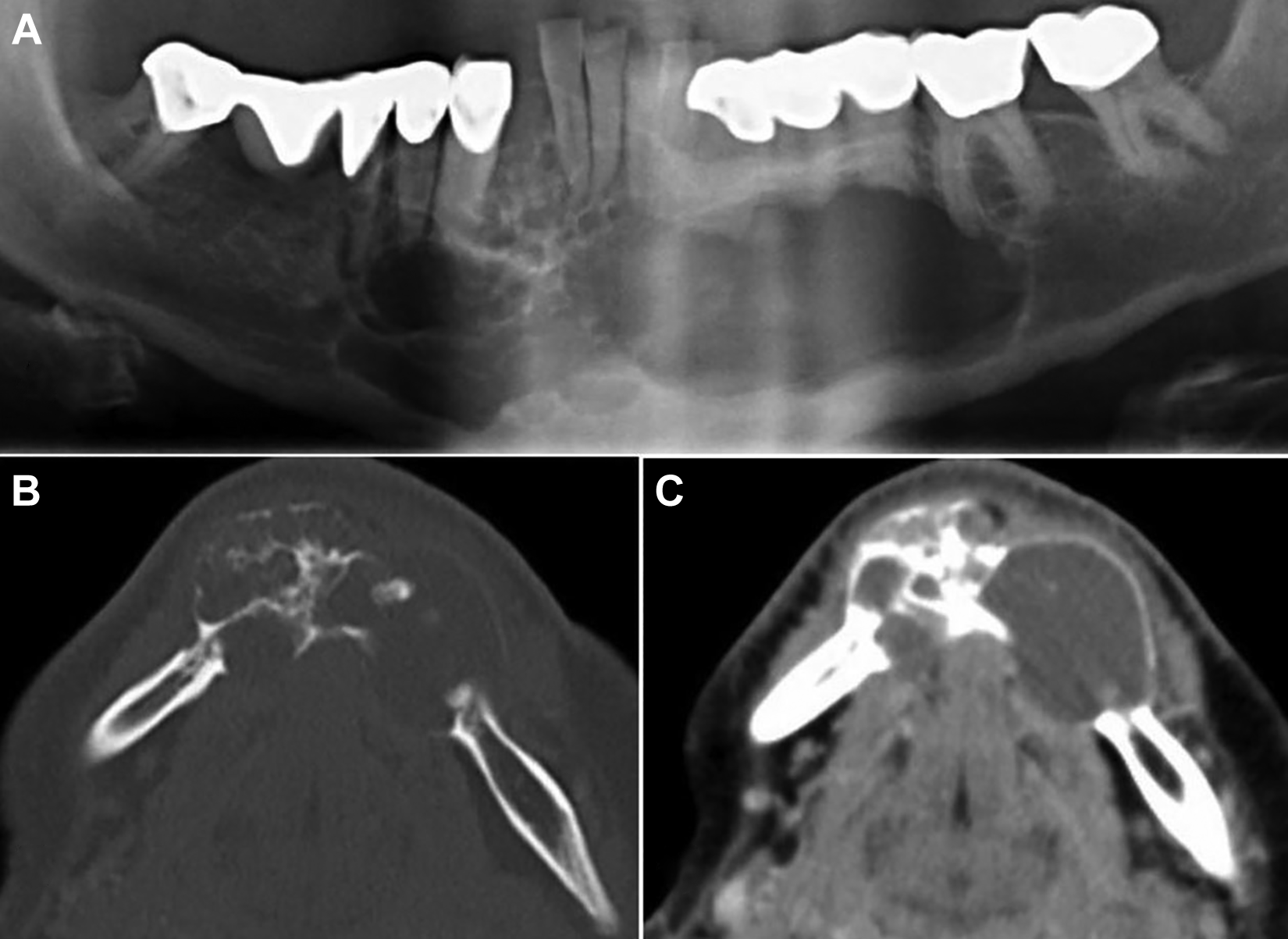
A, Cropped panoramic image of an ameloblastoma with a “honeycombed” multilocular appearance. Note the root resorption of the left canine and premolars. B, Axial CT image using bone algorithm details the multilocular internal structure. The expanded cortex shows a tumor effect, with the greatest degree of expansion occurring along the vector of tumor growth. C, Contrast-enhanced axial soft tissue algorithm CT image demonstrates the multicystic shape of the internal structure. Note the low-attenuation regions of the internal structure representing fluid density. CT indicates computed tomography.
Ameloblastoma is a benign, locally aggressive, epithelial odontogenic tumor of the jaws. Ameloblastomas account for about 18% of odontogenic tumors and 1% of all oral tumors; 81% are located in the mandible, and the remaining 19% are found in the maxilla. 1 Two-thirds of the mandibular lesions occur in the molar-ramus region. It has a peak incidence in the third and fourth decades of life, and is present as a slow-growing, painless swelling of the jawbone. 2 There is no significant sex predilection.
Ameloblastomas are classified into 4 types: solid/multicystic type, unicystic type, desmoplastic type, and extraosseous/peripheral type. 1
The lesion presents radiographically as a well-corticated unilocular or multilocular radiolucency. 2 The multilocular form is often described as having a “honeycomb” appearance (when the loculi are small) or “soap bubble” appearance (when the loculi are large). There is a pronounced tendency for ameloblastomas to cause extensive destruction of bone with marked cortical expansion and root resorption. Most cases of unicystic ameloblastoma are associated with an unerupted tooth, most often a mandibular third molar tooth. This type may be mistaken for a dentigerous cyst because of its pericoronal appearance. In the desmoplastic variant, the radiologic picture may yield a diffuse mixed radiolucent-radiopaque pattern, suggesting a fibro-osseous lesion. 3
The differential diagnosis of ameloblastoma include odontogenic keratocyst, odontogenic myxoma, and central giant cell granuloma. Odontogenic keratocyst and odontogenic myxoma do not expand bone or resorb teeth to the same degree as ameloblastoma. Additionally, the septa in odontogenic myxoma are straight, thin, elongated, and lacy. These septa have been described as making a tennis racket appearance. Central giant cell granulomas occur in a younger age-group and have wispy, ill-defined internal septa.
The treatment of choice for ameloblastoma is marginal or segmental resection depending on the size of the lesion. Because of its tendency to recur, careful follow-up is necessary for at least 10 years. 4 Nodal and pulmonary metastases have been reported only rarely. 5
This patient underwent a segmental mandible resection, and fibula free flap reconstruction followed 1 year later by placement of endosseous implants for dental rehabilitation. The additional 2-year follow-up of the patient was uneventful with good mandibular function, but he was lost to follow-up afterward.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.