
Abstract
Objective:
To assess whether nasal nitric oxide (nNO) levels differ between healthy and sick sinuses in chronic rhinosinusitis (CRS). A secondary aim was to assess whether nNO levels change after treatment of CRS and whether there is an association with radiological findings or symptoms.
Method:
Three groups of 12 participants each were examined: patients with CRS without polyposis (CRS group), patients with symptoms of CRS but radiologically normal sinuses (symptoms-only), and healthy controls. Measurements of nNO were carried out using aspiration method and humming maneuver. All participants completed the Sino-Nasal Outcome Test (SNOT-22). A second nNO measurement was done after treatment in the CRS group (n = 9) and the healthy control group (n = 12).
Results:
Nasal NO did not differ between any of the groups with any of the measurement techniques. There was a trend toward lower nNO values in the CRS group compared with the symptoms-only group and healthy controls, but it did not reach statistical significance. The SNOT-22 demonstrated inferior values for the CRS and symptoms-only groups compared with the healthy controls. At follow-up, no statistically significant change was found for the nNO measurements in either group.
Conclusion:
Irrespective of occluded or open ostiomeatal complexes, no statistically significant differences in nNO were found in CRS compared with healthy controls using aspiration and humming methods. Treatment of CRS improved sinus patency without accompanying a significant change in nNO. This study can therefore not conclude that nNO can be used as a diagnostic tool for CRS without polyposis.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is fairly common, with a prevalence of at least 2% to 6% in the general population and a higher prevalence in women. 1 It often starts in previously healthy persons after a common cold; however, the underlying cause is unknown. 2,3 Chronic rhinosinusitis is a complex of symptoms lasting at least 12 weeks. According to the European Position Paper on Rhinosinusitis and Nasal Polyps, 2007 and 2012, CRS is an inflammation of the nasal and sinus mucosa with or without polyposis, with 2 or more symptoms, one of which should be nasal blockage/obstruction/congestion or nasal discharge. Additional symptoms may be facial pain/pressure, decreased sense of smell/taste, or more unspecific symptoms such as headache, coughing, and tiredness. Patients with this combination of symptoms are common in the clinic, but not all of them have inflammation of the nasal or sinus mucosa and, hence, not all fulfill the criteria for rhinosinusitis, and CRS is hence difficult to diagnose just by clinical examination because facial pain or pressure and “sinus headache” can have a variety of explanations, as rhinologic symptoms, for example, are often present in primary headache disorders. 3 -5 To properly diagnose CRS, a radiological examination is often required and a computed tomography (CT) of the nose and sinuses is the primary choice. 6
In healthy sinuses, there are normally high levels of nitric oxide (NO). 7 Lower levels of NO have been found in patients with CRS; however, this has been reported as significant only in CRS with polyposis. 8,9 Ragab et al 10 and Dabholkar et al 11 both found low levels of nasal NO (nNO) in CRS and an inverse relation between CT scores and paranasal sinuses and nNO. In both studies, surgical treatment resulted in an increase in nNO, which was associated with a decrease in symptom score. 10,11 These results support the importance of NO production in the pathophysiological processes of the upper airway. It is, however, uncertain whether the low nNO levels measured are a result of reduced maxillary NO production and/or are due to obstruction of the sinus ostia. 9,12,13
There are different methods for measuring nNO. Six different approaches were compared by de Winter-de Groot et al, who concluded that 2 of these were superior: aspiration of air from one nostril during breath holding, and the humming maneuver, as they had the highest short- and long-term reproducibility and the lowest within-subject variation. 14 Nasal NO measurements without humming are assumed to reflect the basal NO production in the nasal mucosa, but most probably also NO from the paranasal sinuses also contributes to the measured levels. 7 Measurement using the humming maneuver is likely to more specifically reflect the ventilation and the concentration of NO in the paranasal sinuses. 15,16
There are reports that treatment with intranasal corticosteroids, compared with placebo, is favorable in CRS without nasal polyposis compared with placebo. 3 Randomized controlled studies are, however, few, with differences regarding the type of delivery device as well as the ability of the drug to reach the paranasal system. The latter probably depends on the surgical status, and it seems difficult to reach the sinuses when the ostia are occluded. 3 Treatment with macrolides has been shown to be beneficial, possibly due to their anti-inflammatory effects. In randomized controlled trials by Wallwork et al 17 and Ragab et al, 10 improvements in both subjective and objective outcomes were found after 3 months of low-dose treatment with macrolides in patients with CRS, both with and without polyps. Ragab et al also measured nNO with the aspiration method and found a statistically significant increase after treatment. 10
Since CRS is a common clinical problem, it would be of great help to have an easy screening method for the diagnosis, other than CT scan, and thus decrease both radiation and costs. It can be hypothesized that measured nNO levels using the aspiration method reflect both the ventilation status and the actual NO production in the paranasal sinuses, whereas the humming method better reflects the ventilation of sinuses.
This is an explorative pilot study aiming to assess whether nNO levels differ between healthy and sick sinuses, comparing the aspiration and humming methods. A secondary aim was to assess whether nNO levels change after treatment for CRS, and if so, whether the change is associated with changes in radiological findings and symptoms. Additionally, the aim was also to investigate the relationship between CRS and patient-reported outcome (PRO).
Materials and Methods
Patients
Consecutive patients with symptoms of CRS lasting 12 weeks or more, attending the Ear–Nose–throat Department at Sahlgrenska University Hospital and Frölunda Hospital, Gothenburg, Sweden, were invited to participate in the study. Only nonsmoking patients in the age-group 20 to 65 years were included. “Symptoms of CRS” was defined as 2 or more symptoms, one of which should be nasal blockage/congestion or colored secretion from the nose. All possible participants underwent a nasal endoscopy prior to inclusion. Exclusion criteria were nasal polyposis, previous sinus surgery, systemic chronic diseases affecting the upper airways, infection in the upper airways during the last 6 weeks, oral steroids, immunodeficiency, and current symptoms of pollen allergy.
Three groups consisting of 12 patients each were included in the study: (1) patients who experienced symptoms of CRS with radiological signs of sinus sickness (CRS group), (2) patients with symptoms of CRS but with radiologically proven healthy sinuses (symptoms-only), and (3) healthy controls with no symptoms from the nose or sinuses and with radiologically proven healthy sinuses.
All included participants underwent a CT scan and performed an nNO measurement and filled out PROs. At the first visit, all patients in the CRS group were prescribed treatment with nasal steroids for 3 months. In addition, nasal saline irrigation was recommended. If there was no improvement in symptoms at the follow-up after 3 months, a secondary choice of treatment was offered, namely a low-dose, long-term (3-month) treatment with macrolides (erythromycin or azithromycin). 3,10 After 3 months of treatment, a follow-up was performed for the CRS group, which included nNO measurement, CT scan, and PROs. The healthy control group performed a follow-up nNO measurement within 2 weeks of their first measurement.
Computed Tomography—Lund-Mackay Score
The Lund-Mackay (LM) scoring system 18 -21 was used to grade the CT scan (Table 1) and assessed by 2 independent radiologists. One of the radiologists rated 50% of the material twice, allowing for calculations of intra-rater reliability.
Radiological Findings Were Graded Based on the Lund-Mackay (LM) Scoring System Ranging From 0 = Complete Lucency of all Sinuses to 24 = Complete Opacification of all Sinuses.a
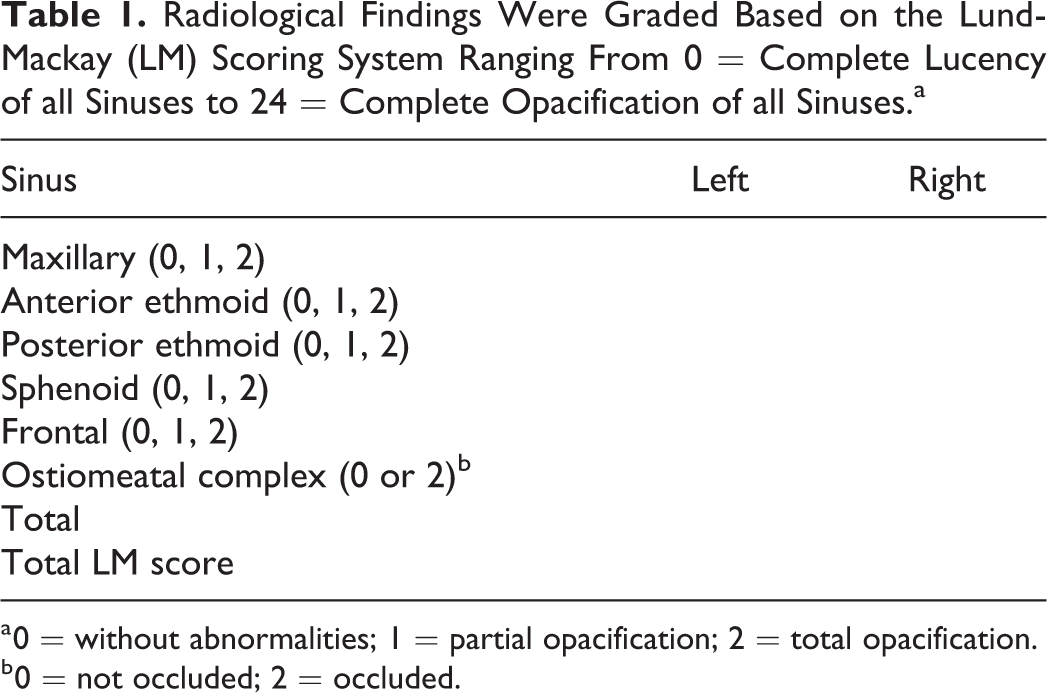
a 0 = without abnormalities; 1 = partial opacification; 2 = total opacification.
b 0 = not occluded; 2 = occluded.
Pathological sinuses were defined as LM score ≥6 with or without occluded ostiomeatal complex (OMC). Healthy sinuses were defined as LM score ≤4 with open OMC based on the findings of Ashraf and Bhattacharyya. 22 Patients with LM score 5, with or without occluded OMC, were therefore excluded from the study.
The healthy controls were recruited from the Radiology Department. These patients were eligible for inclusion if they had undergone a CT scan of the sinuses for reasons other than the suspected pathology of the sinuses. If they did not report symptoms from the nose and sinuses and met the inclusion criteria, they were invited to participate in the study.
Measurements of nNO
All measurements were performed with a chemiluminescence analyzer (NIOX; Aerocrine AB, Stockholm, Sweden). All NO measurements were carried out outside the pollen season and none of the patients had current allergy symptoms. The patients were instructed not to use nasal decongestants, not to eat and drink 1 hour prior to the examination, and to not eat nitric-rich food within the 4 hours prior to the examination. The ambient NO was recorded, and if the level exceeded 20 ppb, measurements were postponed to another occasion.
Aspiration Method
Nasal NO was collected during breath holding with an olive fitted against 1 nostril for 10 seconds, with an aspiration flow of 2.0 L/min. Two measurements were performed in each nostril. The mean nNO concentration (ppb) was registered during the 7 to 10 seconds (Figure 1).
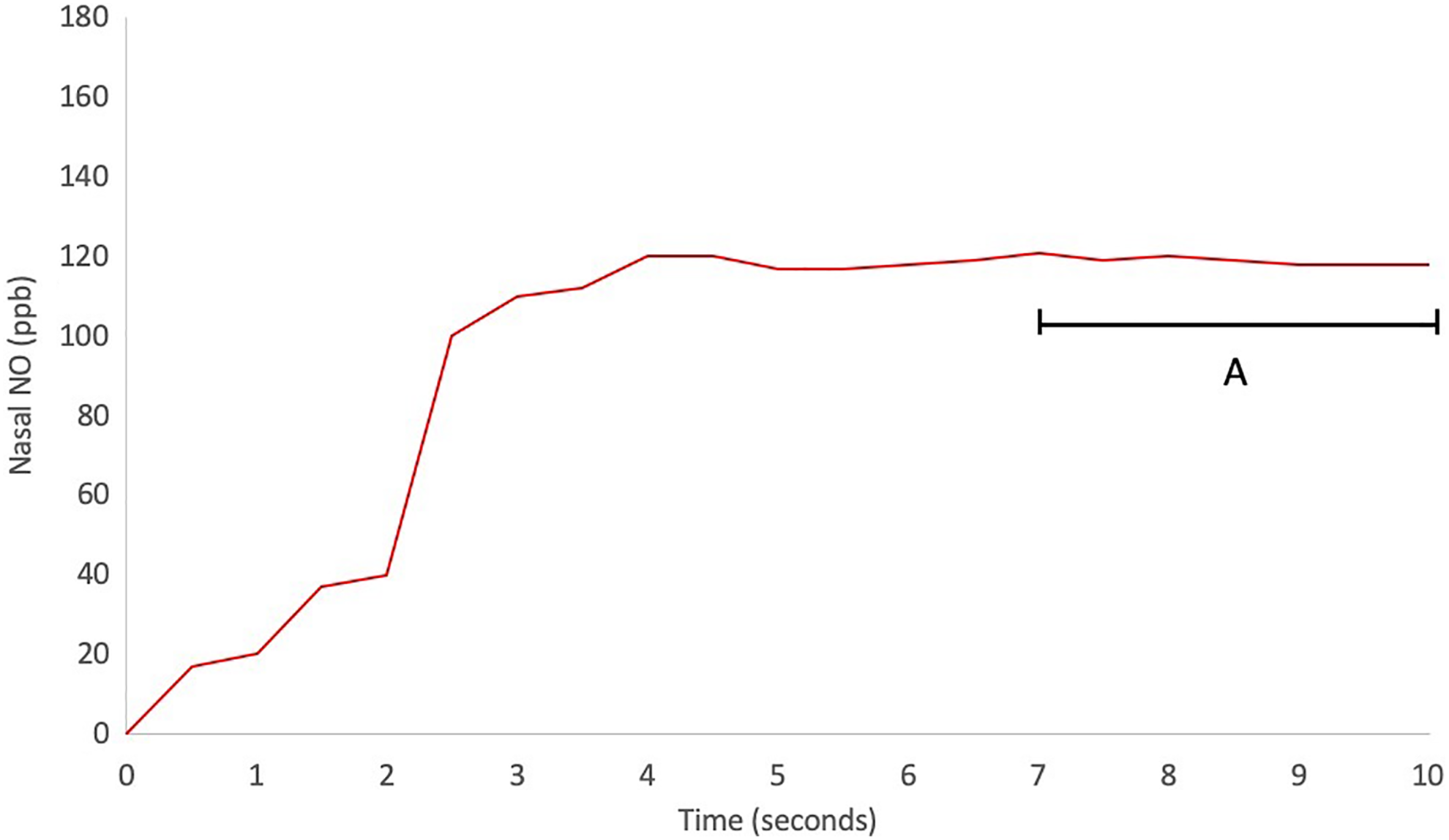
Schematic figure of an online nasal nitric oxide (nNO) measurement using aspiration method in a healthy control during 10 seconds of breath hold. A, The nNO concentration (in ppb) was registered as the mean value for 7 to 10 seconds.
Humming Maneuver
An olive was fitted in the same way as in the aspiration method. The patient was asked to take a deep breath through the mouth and then make an M- or N-sound as loudly as possible with their mouth closed for 8 seconds. The NO concentration was registered during the whole time. An aspiration flow rate of 2.0 L/min was used during this maneuver. Nasal NO was measured 3 times in each nostril. To regain the basal NO concentration in the sinuses after 1 measurement, the patient was instructed not to talk and to breathe at a normal rate for 2 minutes between the measurements. Nitric oxide was registered as (A) the area under the curve (AUC), (B) the peak value (the highest value or the top of the curve), and (C) the NO level at the end of the measurement, that is, after 8 seconds (humming at 8 seconds; Figure 2). Similar to Struben et al, 23 a peak was defined as being prevalent if the NO value at the peak was 1.5 times higher than the value at 8 seconds. A value <50 ppb of the humming at 8 seconds was considered as an absence of a peak since the peak value consequently would be very low.
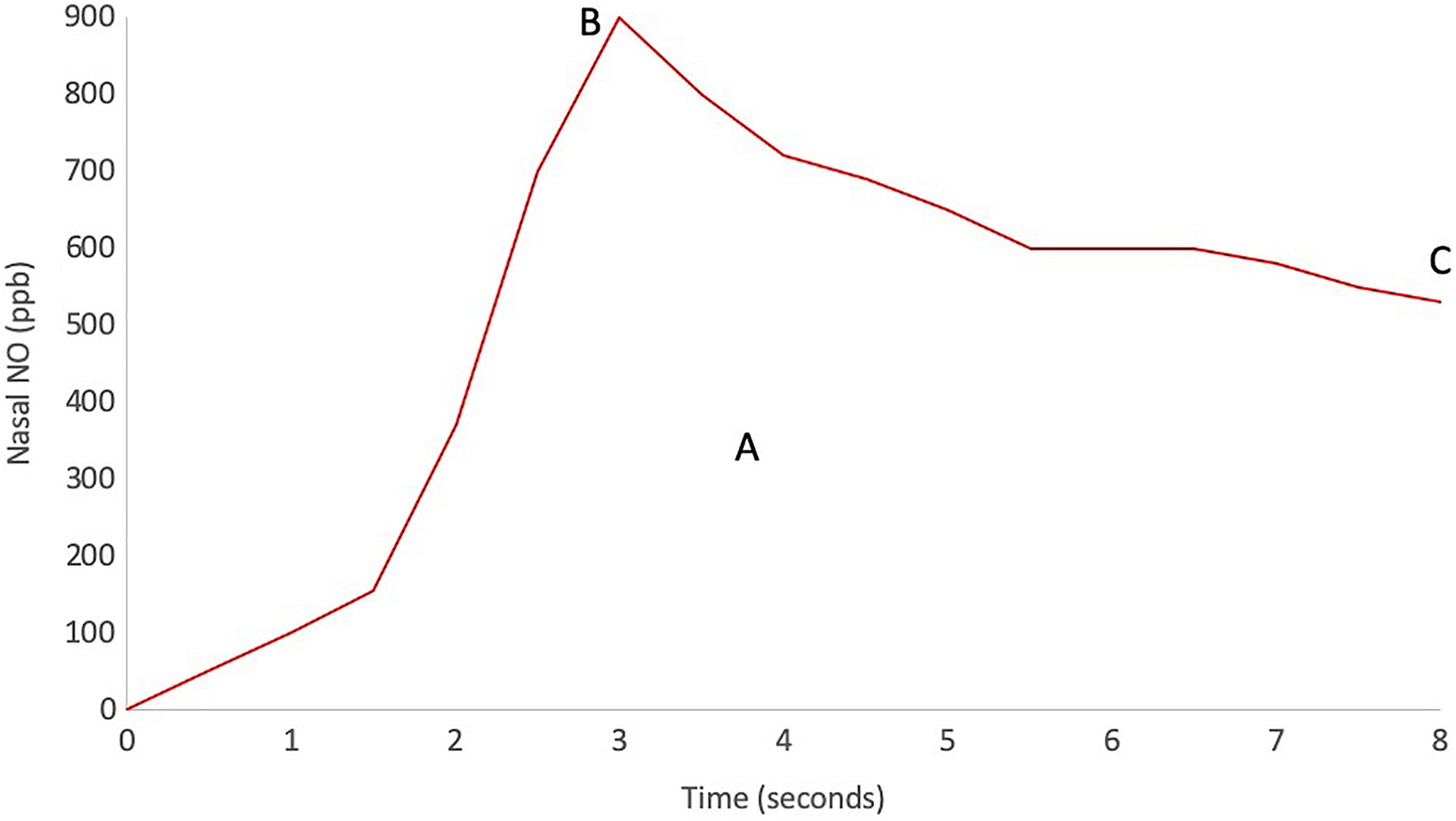
Schematic figure of an online nasal nitric oxide (nNO) measurement in a healthy control during 8 seconds of humming. A, Area under the curve (AUC). B, Peak value, that is, the top of the curve and the highest registered concentration. C, The value measured at 8 seconds, that is, at the end of the measurement.
Patient-Reported Outcome
The disease-specific health-related quality of life instrument for use in CRS, the 22-item Sino-Nasal Outcome Test (SNOT-22), is a modification of a preexisting instrument, the SNOT-20 developed by Piccirillo et al. 24 The items nasal blockage and loss of sense of taste and smell have been added by Browne et al 25 and psychometrically tested by Hopkins et al. 26 The instrument has been translated into Swedish following international recommendations. 27 The SNOT-22 contains 22 items, scored from 0 = “no problem” to 5 = “problem as bad as it can be”. In addition, the patients are asked to mark the 5 most important items affecting their health. A total score is calculated through simple addition of each item, with scores therefore ranging from 0 to 110.
Statistical Analysis
The SPSS version 20.0 for Mac and IBM SPSS Statistics 21 for PC was used for the statistical analyses. Median and range are presented for continuous variables; frequency and percentage are used for categorical variables. Differences between the groups were compared using the χ2 test for categorical variables and the Kruskal-Wallis for continuous variables. For the variables that produced statistically significant differences, post hoc analyses were performed with the Mann-Whitney U test for continuous variables and Fisher exact test for categorical variables, in order to determine between which groups the differences occurred. Spearman correlation coefficient was used for the analysis of association between variables. Intraclass correlation coefficients were used to calculate inter- and intra-rater reliability. All significance tests were 2-sided and conducted at a .05 significance level.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Regional Ethical Review Board in Gothenburg, Sweden. Before inclusion, all patients gave their informed consent to participate.
Results
Patients
In total, 36 patients in 3 different groups were included in the study. There were no statistically significant differences in patient characteristics between the groups (Table 2). Nine patients from the CRS group were included in the follow-up; 3 were excluded from follow-up because of technical problems with the NO instrument. The healthy control group completed their follow-up 2 weeks after their first measurement of nNO.
Patient Characteristics.a
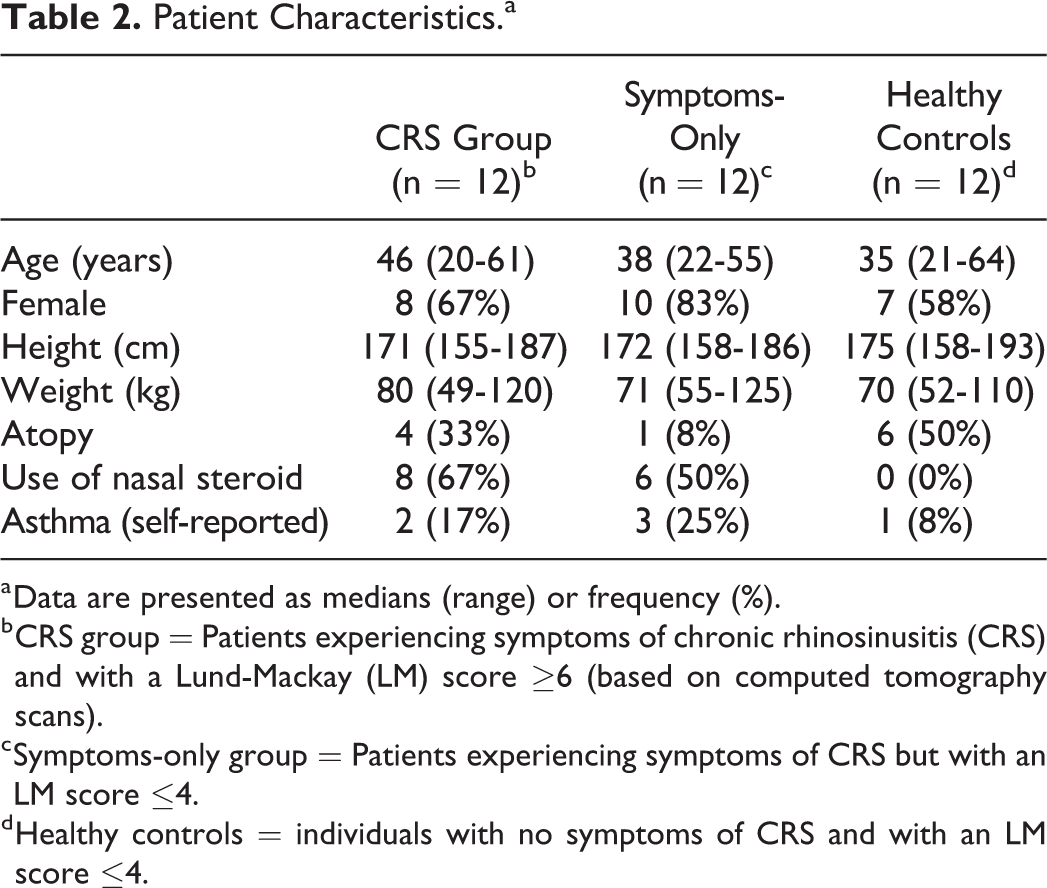
a Data are presented as medians (range) or frequency (%).
b CRS group = Patients experiencing symptoms of chronic rhinosinusitis (CRS) and with a Lund-Mackay (LM) score ≥6 (based on computed tomography scans).
c Symptoms-only group = Patients experiencing symptoms of CRS but with an LM score ≤4.
d Healthy controls = individuals with no symptoms of CRS and with an LM score ≤4.
Lund-Mackay Scores at Baseline
LM scores for all 3 groups are presented in Table 3. In the CRS group, OMCs were occluded in 15 of the 24 possible OMCs. All participants in the healthy control group and the symptoms-only group had open OMCs. The ICC indicated an inter- and intra-rater reliability of 0.92 and 0.98, respectively.
Measurements for all 3 Groups at Baseline.a
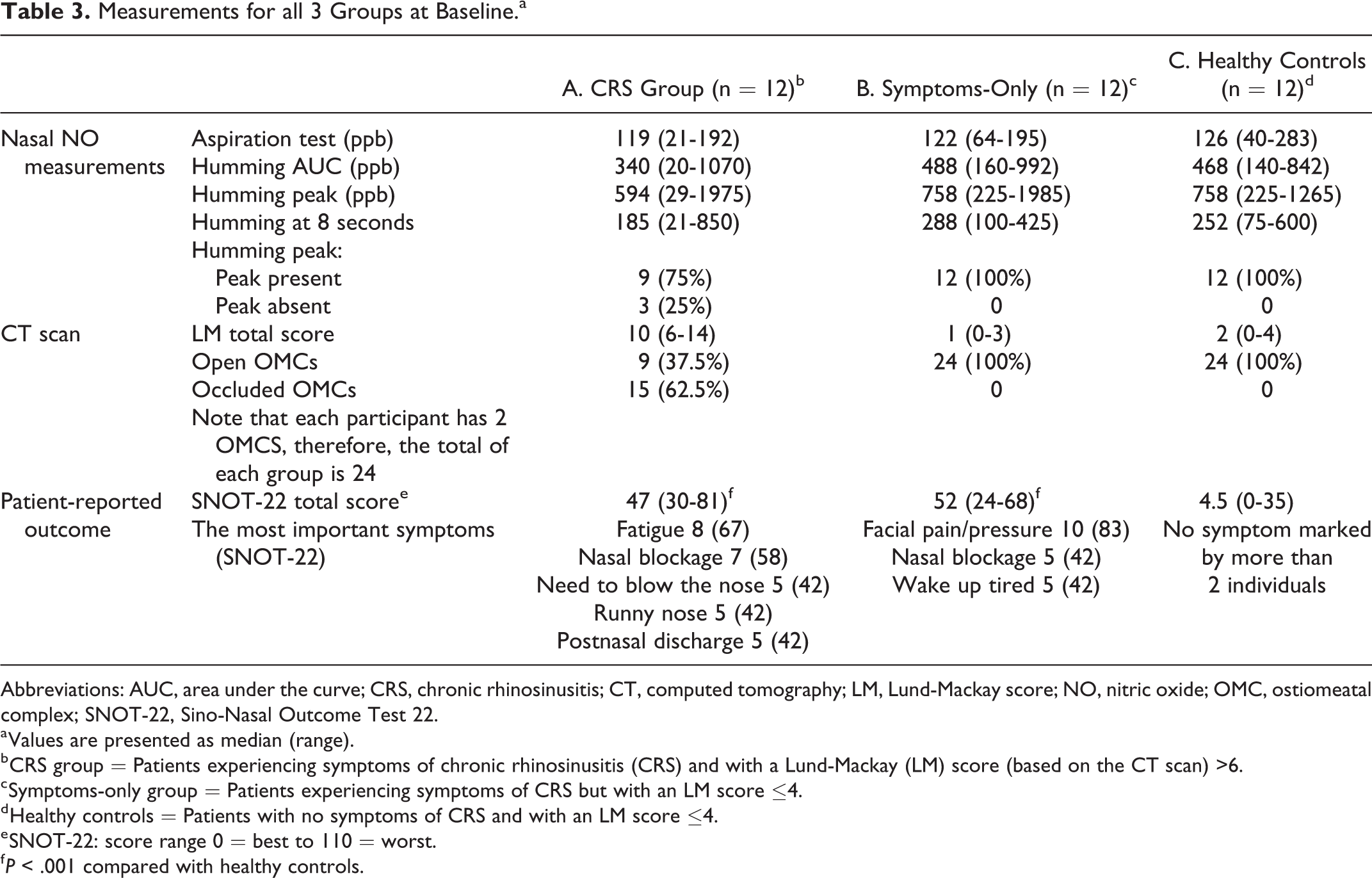
Abbreviations: AUC, area under the curve; CRS, chronic rhinosinusitis; CT, computed tomography; LM, Lund-Mackay score; NO, nitric oxide; OMC, ostiomeatal complex; SNOT-22, Sino-Nasal Outcome Test 22.
a Values are presented as median (range).
b CRS group = Patients experiencing symptoms of chronic rhinosinusitis (CRS) and with a Lund-Mackay (LM) score (based on the CT scan) >6.
c Symptoms-only group = Patients experiencing symptoms of CRS but with an LM score ≤4.
d Healthy controls = Patients with no symptoms of CRS and with an LM score ≤4.
e SNOT-22: score range 0 = best to 110 = worst.
f P < .001 compared with healthy controls.
Nasal NO Measurements at Baseline
Nasal NO measured using aspiration or humming did not differ between the groups (see Table 3) where the medians of nNO for both nostrils are reported, as they were similar. Nasal NO measured using aspiration or humming did not differ between the groups. There was a trend toward lower values using the humming maneuver in the CRS group compared with the symptoms-only group and the healthy controls, but the differences did not reach statistical significance.
In the CRS group, 58% had a peak in both nostrils. In both the healthy controls and the symptoms-only group, a peak was present in both nostrils in all except 1 patient (92%). Within-subject coefficient of variation (CV) of repeated measurements at the same occasion was calculated for all patients at baseline. Mean CV of both sides is presented: aspiration 7%; humming AUC 21%; humming peak 26%; and humming at 8 seconds 18%.
In the CRS group, 58% had a peak in both nostrils. In both the healthy controls and the symptoms-only group, a peak was present in both nostrils in all except 1 participant (92%).
Lund-Mackay Scores at Follow-Up
A second CT scan was performed for the 9 patients in the CRS group who were included in the follow-up. The total median LM score demonstrated a statistically significant improvement from 10 (6-13) to 7 (1-13; P = .035). Six patients demonstrated an improvement in LM score; 3 of them had improved humming measurements and 5 had improved aspiration measurements. Two patients had deteriorated regarding the LM score, with no change in humming measurements but with decreased nNO levels using aspiration. One patient demonstrated no change in LM score but had lower nNO measurements.
Measurements of nNO at Follow-Up
Treatment with nasal steroids for at least 3 months was prescribed and evaluated in the 9 patients from the CRS group who were included in the follow-up. One of the patients was additionally treated with oral steroids for 3 weeks and was symptomatically improved. Five of the patients received additional treatment with low-dose, long-term macrolides. Three improved while 2 were further evaluated for sinus surgery.
There was no change in nNO in the CRS group between baseline and follow-up (Table 4). Numerically, there was a trend toward higher nNO levels using aspiration (median change 25.5 ppb) and humming at 8 seconds (median change 33 ppb), but the change did not reach statistical significance. For the healthy controls, there were no statistically significant changes in the different nNO levels between baseline and follow-up; however, during the humming maneuver, there was a trend toward a higher peak at follow-up (median change 33 ppb). The peak value during humming was also analyzed as a dichotomous variable, that is present or not present. At baseline, the peak was absent in 8 of the 18 measured sinuses. At follow-up, no peak was found in 5 sinuses.
Nasal Nitric Oxide (nNO) Measurements, in ppb, and Other Measurements at Baseline and Follow-Up for the CRS Group and Healthy Controls.
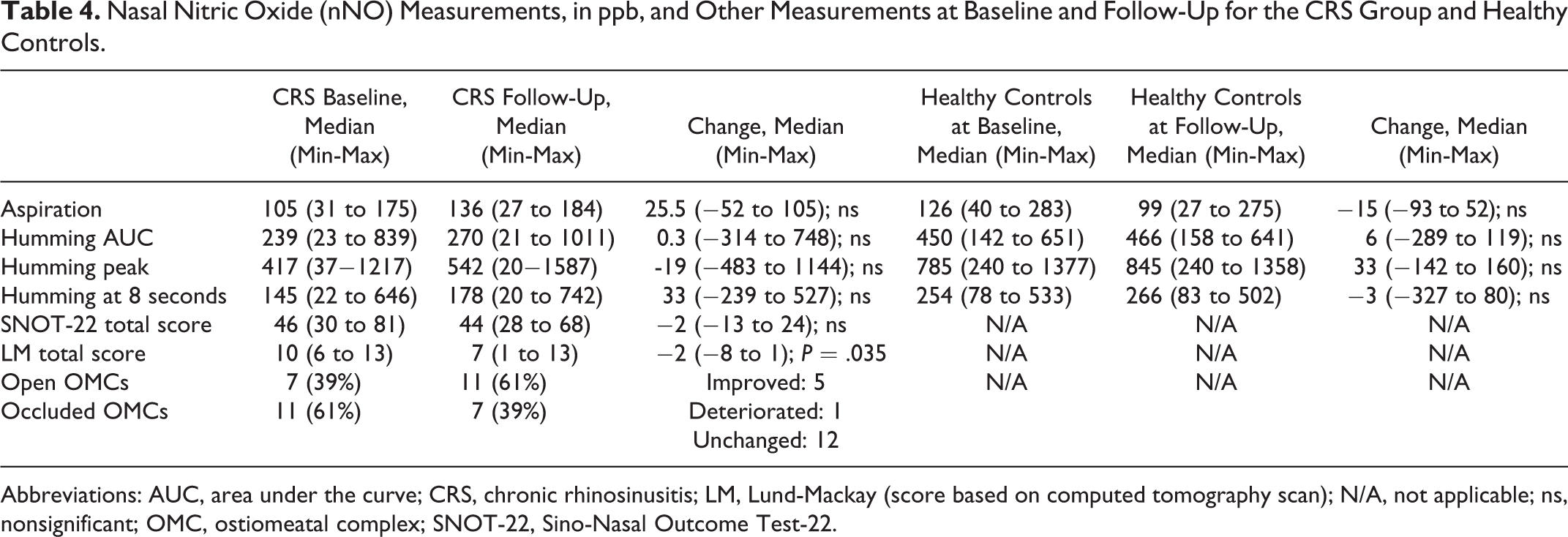
Abbreviations: AUC, area under the curve; CRS, chronic rhinosinusitis; LM, Lund-Mackay (score based on computed tomography scan); N/A, not applicable; ns, nonsignificant; OMC, ostiomeatal complex; SNOT-22, Sino-Nasal Outcome Test-22.
Ostiomeatal Complex and nNO
The OMCs of the patients in the CRS group were divided into 2 groups according to OMC status: occluded (n = 15) or open (n = 9). Descriptive data on baseline values are reported in Table 5. There was a trend toward lower humming AUC and peak nNO values in the group with occluded OMCs, but without statistical significance. The aspiration method demonstrated a reverse trend, with occluded OMCs resulting in higher nNO values. The peak level during humming was also analyzed as a dichotomous variable in the 2 OMC groups. There was no significant difference regarding the peak, although a somewhat larger proportion of occluded OMCs demonstrated no peak (40%) compared with unoccluded OMCs (22%). At follow-up, there was an improvement in LM scoring, with 7 OMCs being occluded compared with 11 at baseline. Also, a humming peak was absent in 5 sinuses, 4 (80%) of which demonstrated OMC occlusion. A peak was found in the remaining 13 sinuses, 10 (77%) of which demonstrated open OMCs.
Comparisons Between the Ostiomeatal Complexes (OMCs) Evaluated as Open Versus Occluded (n = 24) at Baseline.a
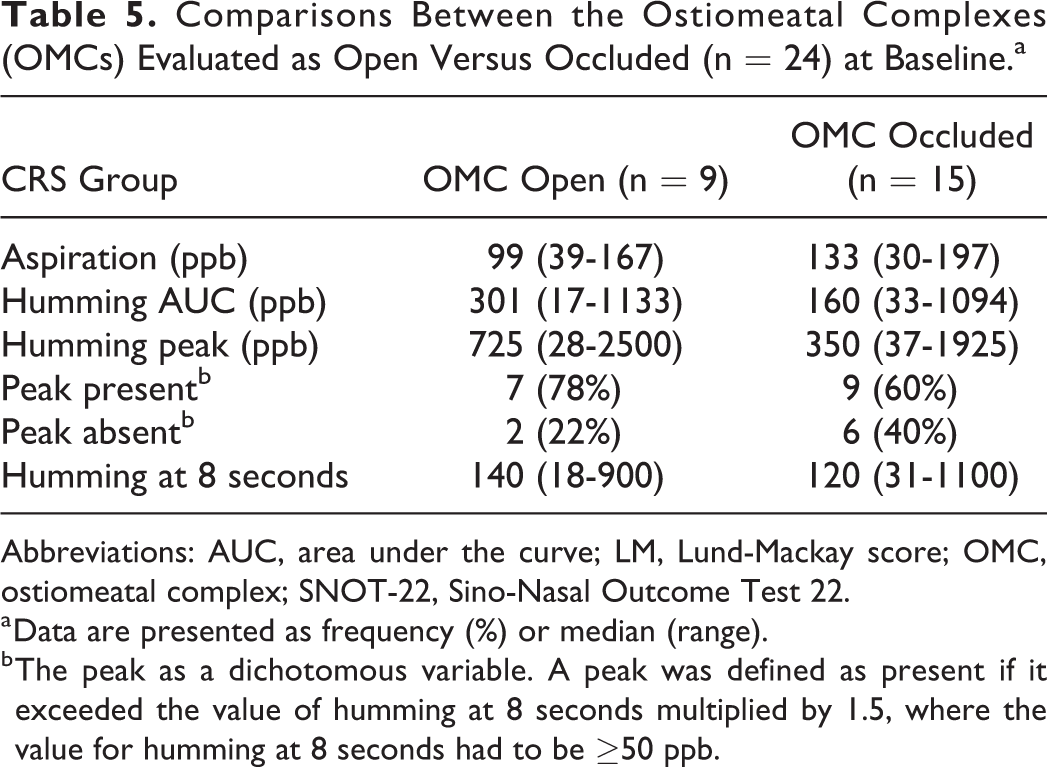
Abbreviations: AUC, area under the curve; LM, Lund-Mackay score; OMC, ostiomeatal complex; SNOT-22, Sino-Nasal Outcome Test 22.
a Data are presented as frequency (%) or median (range).
b The peak as a dichotomous variable. A peak was defined as present if it exceeded the value of humming at 8 seconds multiplied by 1.5, where the value for humming at 8 seconds had to be ≥50 ppb.
Patient-Reported Outcome
The CRS and symptoms-only groups had similar SNOT scores (median values 47 and 52, respectively), both higher than the scores of healthy controls (median 4.5; Table 3). For the CRS group, there was no statistically significant change in SNOT-22 score at follow-up. The changes in SNOT scores are presented in Table 4.
Correlations Between Methods
At baseline, the 3 groups were merged for calculation correlations between methods to measure nNO as well as LM scores and PROs. Strong correlation coefficients were found between the different humming measures (rs = 0.935-0.943, P < .01; data not shown). Moderate correlations were found when comparing aspiration levels with the different humming measures (rs = 0.473-0.532; P < .01). There were no statistically significant correlations when comparing LM scores, SNOT-22 scores, and nNO measurements.
For the healthy controls, correlations were calculated between baseline and follow-up. The baseline and follow-up measurements were expected to correlate strongly since no change was expected to have occurred. Humming AUC (rs = 0.825; P < .01) and humming peak (rs = 0.951; P < .01) demonstrated strong correlations between the 2 measurement points. A moderate correlation was found for humming at 8 seconds (rs = 0.65; P < .01). No significant correlation was found for aspiration between baseline and follow-up.
Discussion
This explorative pilot study aimed to evaluate whether nNO levels in CRS without polyposis differ between healthy and sick sinuses and to assess whether treatment and changes in symptoms are associated with a change in nNO over time. We did not find any statistically significant differences in nNO between healthy controls and patients with occluded sinuses, using both humming and aspiration methods to assess nNO. There was a trend toward lower nNO values measured with the humming method in patients with radiologically proven occluded sinuses—however, not reaching statistical difference. At follow-up, although only comprising 9 patients, there was a trend toward increasing nNO levels in the CRS group—however, without statistical significance. In addition, no correlations were found between the PROs and the nNO measurements. In healthy controls, nNO measurements were relatively stable over time, indicating that they are reproducible in healthy controls.
The humming peak was hypothesized to reflect the degree of ventilation of the sinuses as suggested by Weitzberg and Lundberg, 15 that is, a low or absent peak would indicate an occluded OMC. The results of the present study could, however, not support this, as the results in the CRS group were contradictory and difficult to interpret; a peak could be present even if CT indicated an occluded OMC and, contrarily, in some instances, no peak was detected even if the OMC was classified as open. At follow-up, when a peak was absent, the OMC was occluded in 75% of instances, but only in 44% of the cases where a peak was present, an open OMC was demonstrated. On the other hand, significant improvement in LM score was found and the OMC status also showed a trend toward improvement, from 11 OMCs with occlusion at baseline to 7 occluded OMCs at follow-up. The humming method also only showed a trend toward increased values of nNO after treatment.
We do not consider our results to be due to technical difficulties, as the measurements were highly reproducible in healthy controls, and all measurements were performed by the same investigator (C.A.). Other reasons must hence explain these contradictory results, where differences in pathological mechanisms behind CRS are likely. We can also not exclude variations in mucosal swelling or variations in the obstruction of the sinuses due to mucus.
Our results contradict a previous study by Maniscalco et al, 28 which showed that the absence of an nNO peak during humming was associated with endoscopic findings suggestive of sinus ostial obstruction. Our results are, however, limited by the low number of included patients but could not fully support these findings. On the other hand, we could compare with findings from CT scans, the gold standard to diagnose CRS. Bommarito et al and Lee et al showed significantly lower levels of nNO, however, in only patients with CRS having nasal polyps, not in those with nasal polyps compared with healthy controls. 8,29 Dabholkar et al found statistically significant differences between a healthy control group and patients with CRS, but the study did not distinguish between CRS with or without polyposis. 11
We did not find any correlations between nNO and radiological findings graded by LM score. Dabholkar et al, by contrast, found that nNO concentration measured with the Aspiration method was strongly correlated with CT scores. 11 This discrepancy in results may be explained by higher LM scores and lower nNO values due to the inclusion of patients with CRS having polyps in Dabholkar et al.’s study. 11
The measurements with the aspiration method were performed twice in each nostril and showed stable values when repeated. We also repeated the humming measurements in the healthy controls and show moderate to strong correlations between baseline and follow-up, indicating that the measurements are stable in sinuses where no changes are expected to occur. The different methods to measure nNO (humming and aspiration) correlated only moderately.
The results of the SNOT-22 showed almost equal scores (47 and 52, respectively) for the 2 symptom groups, that is, the CRS group and the symptoms-only group, highlighting the profound influence on the quality of life also in the group without any objective measures of occluded sinuses and the need for improved treatment of both groups. No statistically significant change in SNOT-22 scores was found at follow-up for the CRS group, indicating that these patients did not experience a relief of symptoms despite the treatment, and even though a statistically significant difference regarding the LM-score was found, further supporting the complex nature of this disease. The median level of SNOT-22 score was 4.5, which is close to the findings in a recent study by Lange et al who reported a median score of 7 in the general population. 30 It was also hypothesized that the SNOT-22 scores would reflect the levels of nNO; however, no correlations between these measurements were found and the hypothesis had to be rejected. So far, the only way to improve PROs is surgery, demonstrated by Ragab et al, who evaluated the medical and surgical treatment in CRS both with and without polyposis and found a statistically significant improvement in SNOT-20 score. 10
This study is limited by the low number of participants, particularly in the CRS group, where 3 individuals at follow-up are missing because of technical difficulties. However, we included only patients with CRS without polyposis, unlike other studies that might be limited by their inclusion of patients with CRS with and without polyposis. 7,8,11 A strength of this study is that the same researcher (C.A.) has performed all nNO measurements; therefore, the results of the measurements should be valid.
To our knowledge, this is the only study aiming to evaluate the aspiration and the humming methods in CRS without polyposis, by comparing a group with CRS symptoms and healthy controls. In our hands, measurements of NO using humming seem only to a minor extent to reflect the level of sinus ventilation. Other, yet unknown, factors are likely also to be of high importance. This leads us to conclude that measurements of nNO are less useful as a screening tool to identify patients with occluded sinuses, something which is highly asked for. Our results confirm that CRS is a complex disease to monitor. The monitoring probably involves more than the detection of open versus occluded sinuses.
Conclusions
No statistically significant differences in nasal NO were found in CRS, irrespective of occluded or open OMCs, compared with healthy controls using both aspiration and humming methods. Pharmacological treatment of CRS with occluded sinuses improved sinus patency, but this was not accompanied by any significant change in nNO, further suggesting that nNO is not of clinical use in CRS.
Footnotes
Acknowledgments
The authors would like to thank Dr Martin Bonnier and Dr Peter Kälebo at the Department of Radiology, Sahlgrenska University Hospital, Gothenburg, Sweden, for their contribution regarding radiological examinations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.