
Abstract

A 4-year-old male presented for management of recurrent craniopharyngioma. He was previously found to have a suprasellar mass and underwent left pterional craniotomy and subtotal resection for diagnosis and decompression. On 6-month follow-up, there was clinically decreased vision in the patient’s only-seeing eye and noted progression with a primarily sellar component (Figure 1). Due to recurrence, location, and threat to vision, expanded endoscopic endonasal approach (EEA) was indicated to optimize decompression of the optic apparatus.
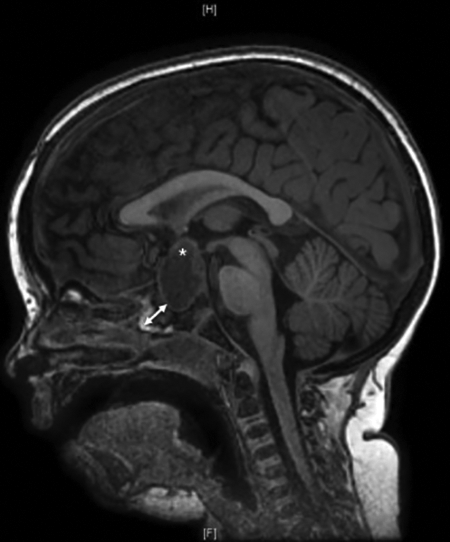
This sagittal T1 magnetic resonance imaging (MRI) of a 4-year-old male was obtained 4 months following subtotal resection of sellar craniopharyngioma via pterional craniotomy. The asterisk illustrates the suprasellar extension of the craniopharyngioma. The double-sided arrow highlights the extent of nonpneumatized sphenoid that would be drilled during endoscopic resection.
The patient underwent trans-sellar EEA with elevation of a right-sided nasoseptal flap and left-sided reverse flap. The sella was exposed by drilling the nonpneumatized sphenoid bone away and entered in a standard fashion. The craniopharyngioma was completely resected. Dura was repaired with inlay collagen matrix and onlay of the nasoseptal flap secured with cellulose packing, carboxymethylcellulose foam, and nonabsorbable sponges (Figure 2).

Displayed is the initial cranial base repair in a 4-year-old male after expanded endonasal approach and resection of a craniopharyngioma with inlay collagen matrix (not seen) and nasoseptal flap (outlined with dashed line).
The patient’s postoperative hospitalization was prolonged due to issues with sodium homeostasis secondary to diabetes insipidus. He demonstrated frustration with frequent blood draws and medication administration manifesting in emotional outbursts with breath holding and screaming. In this setting, on the 14th postoperative day, he experienced sudden onset of clear rhinorrhea and subsequently returned to the operating room for exploration and revision.
Nasal endoscopy revealed viable nasoseptal flap without necrosis. There was slight migration of the right superior corner of the flap with resultant exposure of the dural defect. The flap was taken down and collagen matrix replaced. The depth of the defect was attenuated with abdominal fat and the flap redraped with excellent coverage of the fat. This was again bolstered with cellulose packing and nonabsorbable sponges.
Following revision surgery, the patient continued to have worsening agitation with hospitalization and nursing care. Maximum noninvasive efforts were employed including utilizing distraction, limiting lab draws, and enlisting the assistance of occupational therapy, child life, and therapeutic recreation. These efforts were met with minimal success, and the patient experienced another episode of clear rhinorrhea 15 days after revision.
A second revision surgery followed by continued intubation and sedation for 96 hours was then carried out. Endoscopy revealed a recurrent cerebrospinal fluid (CSF) leak in the superior right corner of the sella at the location of the initial leak and was addressed with a small abdominal fat graft that was used in “bath-plug” technique. 1 This was bolstered with repositioning of the original fat graft and tissue sealant to affix these materials in place (Figure 3). The nasoseptal flap was replaced and bolstered with cellulose packing, nasopore, duraseal, and nonabsorbable sponges. The patient was then transferred to the PICU, intubated, and sedated for further care.

Demonstrated here is the revision cerebrospinal fluid leak repair in a 4-year-old male after expanded endonasal approach and resection of a craniopharyngioma. At the depth of the photo (asterisk) is the onlay collagen matrix dural repair. A “bath-plug” collagen matrix repair of the focal leak (star) is also seen. In the foreground (arrow) is an abdominal fat graft used to bolster the repair. This was covered with the nasoseptal flap visualized in Figure 2 (not seen in this image).
On second-look endoscopy, the circumference of the flap was investigated with no evidence of leak. The patient was extubated, weaned off sedation, and discharged over the following 5 days. The patient experienced no further sequelae and remains free of disease recurrence at 2-year follow-up.
Although EEA has increasing use in pediatric patients, controversy remains over appropriate application in the youngest patients. 2 -4 Use of EEA faces unique challenges in children, including variability in sphenoid pneumatization, smaller anatomical space, and closer proximity to vital structures such as the carotid arteries and optic chiasm. 2,5,6 Additionally, pediatric patients pose challenges postoperatively with compliance and tolerance of hospitalization. 7
In this case, numerous factors may have contributed to the postoperative CSF leak, including flap inadequacy or contraction, surgeon’s experience, and patient’s behavior. 5,8,9 One likely contributor was poor adherence to nasal precautions and behavioral struggles. Emotional outbursts and bearing down initiate a Valsalva maneuver with associated increase in intracranial pressure, applying stress to the dural repair. 10 Our patient’s persistent agitation resulted in the decision for sedation after revision surgery. Postoperative sedation with mechanical ventilation is a technique routinely implemented in other pediatric surgeries such as cardiac and airway reconstruction surgery. 11 -14 This technique ensures pain is managed appropriately and movement is minimal to allow proper healing without disturbances. Prolonged intubation and chemical sedation carry a variety of risks. As such, decisions to pursue these measures should be made on a case-by-case basis.
In summary, care of pediatric patients after endonasal skull base surgery presents challenges not encountered in adults. We believe thorough preoperative assessment is beneficial to identify factors that could decrease adherence to nasal precautions. Planned sedation after surgery is an option, but risks and benefits must be weighed for each situation. The authors suggest a graded approach with a trial of standard nasal precautions, utilizing distraction techniques and therapeutic recreation as available, with possible chemical sedation in the setting of surgical failure without another clear etiology.
Footnotes
Authors’ Note
Portions of this work were presented as an oral presentation at the American Society for Pediatric Otolaryngology Annual Meeting, May 21, 2017, Austin, TX.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Charles A. Elmaraghy is a consultant for Smith and Nephew.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.