
Abstract
The goal of this prospective cohort study was to characterize the ability of teachers to identify schoolchildren at risk of hearing loss in order to maximize hearing screening efficiency in low-resource settings. At 4 semirural schools in Malindi, Kenya, preselected schoolchildren perceived as hearing impaired were compared to children thought to have normal hearing using portable audiometry. Eight of 127 children (54% male) failed hearing screening, all of who were identified by schoolteachers as having a high risk of hearing loss. Thus, for every 5 children prescreened by schoolteachers, an average of 1 child would be identified as having hearing loss. Overall, teacher prescreening had a 100% hearing loss identification rate and a 20% referral rate. In conclusion, in resource-limited settings, where universal hearing screening is challenging, teachers can effectively identify children with hearing loss for early intervention.
Keywords
Introduction
The burden of hearing loss (HL) in the developing world is overwhelming, with nearly 90% of the estimated 34 million children affected born in countries with limited resources. 1 Not only are low- and middle-income countries (LMICs) least able to overcome the pervasive effects of HL, but they are also severely limited in the number of hearing providers with the ability to provide early identification, intervention, and hearing services. 2 -4 Recently, tablet and cell-phone audiometry has made it possible to screen children for HL in resource-poor environments. 5 -7 There remain, however, an extraordinary number of individuals at risk of hearing impairment, and there still have been limited attempts to increase the efficiency of screening in these settings.
Teachers have been shown capable of identifying children at risk of mental health issues and autism; reduced visual acuity; and poor attention, executive function, and adaptive skills. 8 -14 Similarly, HL may be particularly difficult to manage in the classroom setting, manifesting as inattention, disruptive behavior, poor focus, and speech impairment, and even unilateral HL may lead to impaired long-term cognition. 15 Furthermore, in the developed world, it is appreciated that teachers provide valuable referrals for hearing evaluation. 16 -18 Given the amount of time children spend in school and the significant communication and interactions between these students and their teachers, we sought to exploit the natural insights of the teacher–student relationship in LMICs.
In the developing world, where resources are limited and universal hearing screening is not a feasible option, we hypothesized that teachers could accurately identify at-risk children. Thus, the intent of this study was to characterize schoolteachers’ ability to identify children at risk of HL while still allowing high-quality hearing screening with the hopes of early identification and the maximization of resources in the developing world.
Patients and Methods
Children aged 2 to 16 years with no history of HL underwent hearing screening at 4 semirural prekindergarten, primary, and secondary school classes located 15 to 20 km from Malindi, Kenya. Teachers were asked to identify “at-risk” children who they perceived as having trouble hearing. There was no formal training, and teachers were asked to identify children based on subjective concerns of HL, inattention, difficulty learning, poor classroom participation, poor speech, and disobedience. Children who exhibited discomfort during the examination or were unable to tolerate hearing screening were excluded from the study (n = 0). These prescreened children were compared to a similar group of children who were not thought to be “at risk.” This project was institutional review board approved by the Vanderbilt University Medical Center.
The technology-based platforms, HearX Group’s HearScreen (HearX Group, Pretoria, South Africa) and the SHOEBOX’s play audiometry (Clearwater Clinical, Ottawa, Ontario, Canada), were used for hearing screening. Results were categorized as “pass” (500-4000 Hz pure-tone thresholds ≤35 dB) or “refer” (pure-tone thresholds ≥40 dB). This threshold was determined, as it has been previously defined by the Global Burden of Disease Expert Group on Hearing Loss as the threshold in which intervention would be warranted (≤35 dB). 19 Chi-square and number needed to treat was performed with Stata/SE version 15.0 (College Station, Texas).
Results
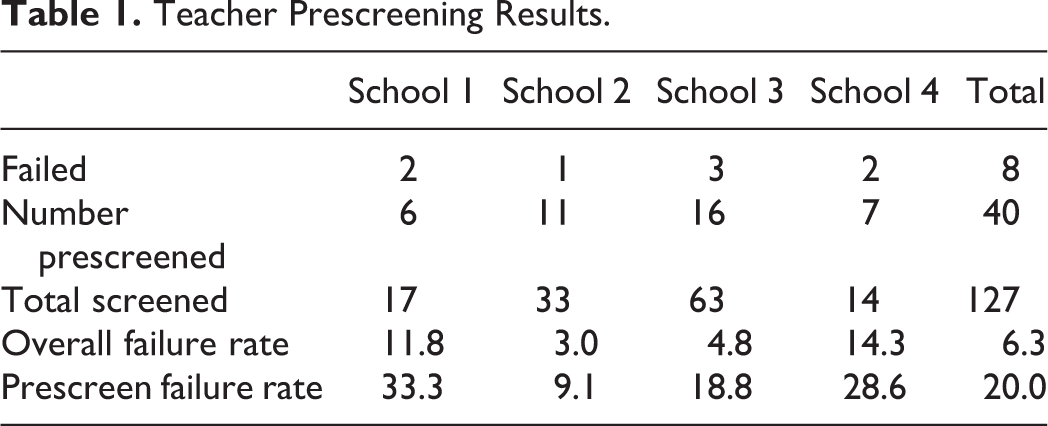
One hundred and twenty-seven children, aged 2 to 16 years (median 7 years [interquartile range, IQR: 4-9]) underwent hearing screening at 4 schools located 15 to 20 km from Malindi, Kenya. Children were screened at the point of care, and therefore there were no dropouts in the study. There were 68 (53.4%) males and 59 (46.5%) females. Complete hearing screening results are shown in Table 1 and Figure 1. Teachers identified 40 children with concern for HL (31.5%). A total of 8 children failed hearing screening (3 males and 5 females; median age = 8.5 [IQR: 6.24-10.5] years) who required further intervention, including treatment of otitis media, ENT referral, and formal audiometry retest for hearing aid candidacy (Table 2). All 8 children with HL were within the cohort identified by teachers as having a high risk of HL (P < .01). Thus, for every 5 children prescreened by schoolteachers, 1 child on average would be identified as having HL. Overall, teacher prescreening had a 100% identification rate and a 20% referral rate.
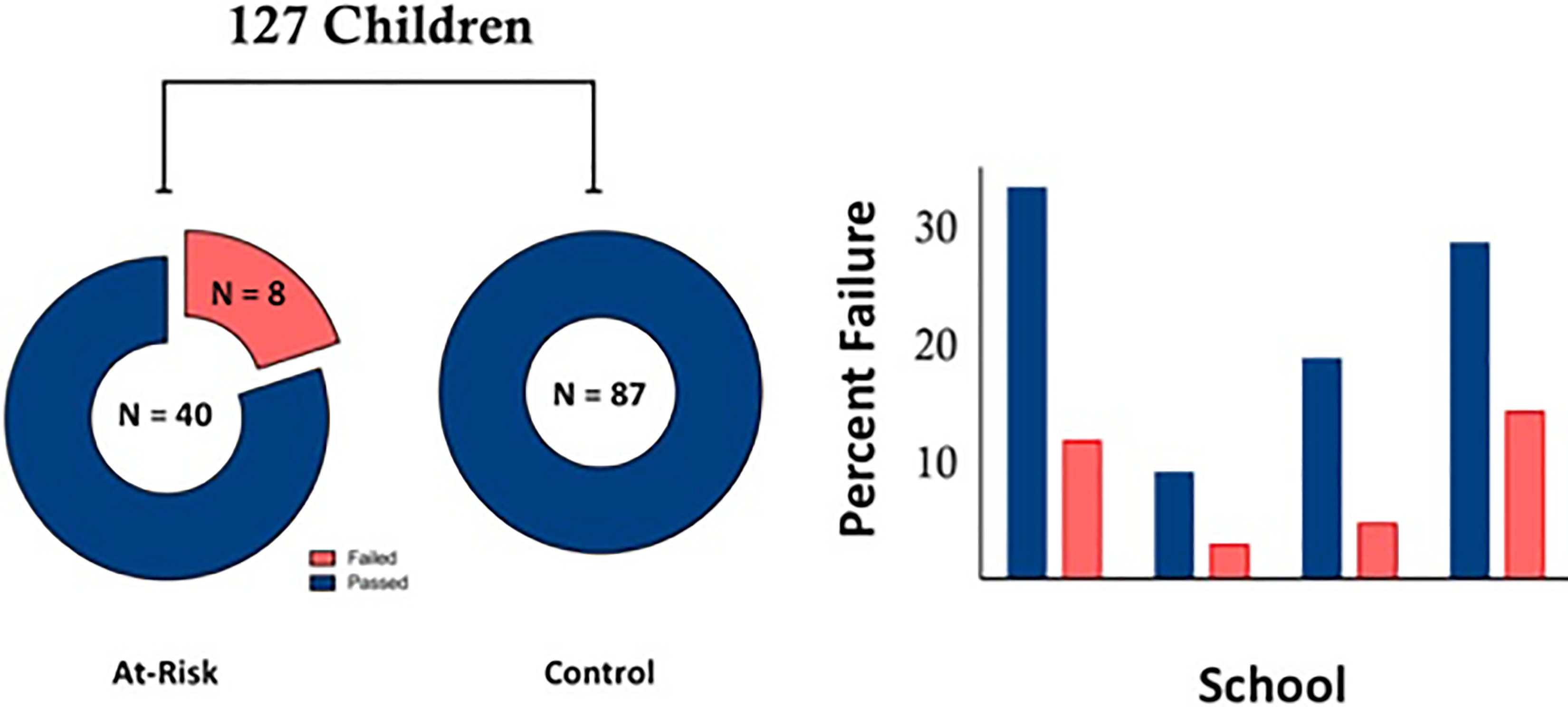
Teacher prescreening results. Left, Children who passed (80%) and failed (20%) hearing screening when prescreened by schoolteachers compared to children who were not identified as being at risk of hearing loss (100% pass rate). Right, Hearing screening failure rate for each school (blue = prescreened children; red = all children including prescreened children).
Teacher Prescreening Results.
Children With Failed Hearing Screening.
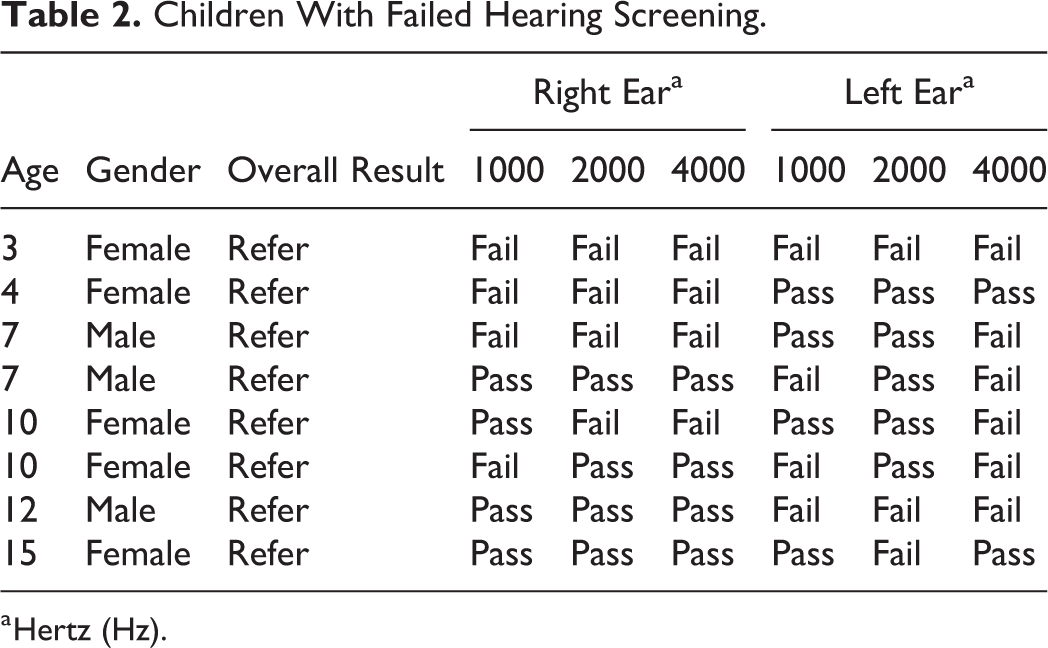
a Hertz (Hz).
Discussion
Children spend a significant amount of their formative years in school, and in the developed world, teachers provide valuable referrals for hearing evaluation. Our results show that teachers in LMICs are able to accurately identify children at the highest risk of HL at an important developmental period and have the potential to be an integral component in a sustainable hearing-screening program. 20 This finding can ultimately facilitate higher yield hearing screening, a concept especially important in regions without resources for universal hearing screening. Teachers, with their close interaction with their students, possess unique insight into children who are struggling and can immediately intervene through implementation of appropriate classroom positioning and development of alternate educational models. Furthermore, teacher identification and awareness of HL in the classroom is likely to produce a favorable response to include and educate these children at risk of intellectual delay and poor performance. 21 By extrapolating our pilot data, teacher prescreening could potentially reduce the need for hearing screening by 70% and could allow for more efficient hearing screening in low-resource settings.
Our data are limited by our small sample size, and additional studies are necessary to understand the utility of teachers as active participants in the hearing-screening algorithm. This study additionally does not compare a new test to a gold standard method, and none of the children underwent formal audiometric testing. We are unfortunately not able to truly determine whether those who were referred on hearing screening had HL.
Footnotes
Authors’ Note
J.R.S. and A.D.L.J. contributed to concept design, data analysis and interpretation, manuscript drafting and revision, and final approval. J.R.S. and M.G.Z. contributed to data acquisition. M.G.Z. contributed to concept design, data analysis and interpretation, manuscript revision, and final approval. J.L.N. contributed to concept design, data acquisition, data interpretation, manuscript revision, and final approval. Justin R. Shinn, Asitha D. L. Jayawardena, M. Geraldine Zuniga, and James L. Netterville. “Teacher pre-screening as a means to reduce hearing screening burden in low- and middle-income countries.” Poster presentation: American Academy of Otolaryngology Annual Meeting, Atlanta, Georgia. 2018.
Acknowledgments
The authors thank Tawfiq Hospital; the Caris Foundation; Ian Macharia, MBChB (Department of Otolaryngology, University of Nairobi, Nairobi, Kenya), Chrispus Munga, CO (Caris Foundation, Malindi, Kenya), and Jim Reppart, MA (Caris Foundation, Malindi, Kenya).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.