
Abstract
Objective:
To evaluate speech understanding in noise and patient satisfaction using the new Cochlear Wireless Phone Clip device.
Material and Methods:
Twenty-nine experienced cochlear implant (CI) users (>6 months usage) were situated in a soundproof room where a 65 dB SPL Spanish cocktail noise was generated continuously from 4 loudspeakers. Lists of disyllabic words were presented through the clinic landline telephone to the patients. Patients were tested first holding the phone and then with the Cochlear Phone Clip© paired to the CP910 using various mixing ratios (2:1, 4:1, and Phone Clip© only).
Results:
Statistically significant (P < .001) improvement of speech recognition performance was found in cell phone usage by wireless transmission and also when using this new device. Kepler questionnaire results showed that before using Phone Clip in everyday life, 55.2% of patients described themselves highly or greatly affected by their deafness for telephone use and 80% moderately to greatly affected. Kim questionnaire results showed statistically significant differences (P < .001) in the subjective satisfaction of the Bluetooth-implemented CI compared to the conventional mode for sound quality, noise interference, and sound accuracy.
Conclusions:
The wireless Phone Clip© device helps implanted people to improve subjective and objective speech recognition performance through the phone in noisy environments.
Introduction
Use of telephone is one of the imperatives of contemporary life. Use of the telephone is not always easy for many cochlear implant (CI) recipients, because of the limited frequency range (300-3400 Hz) and the various types of interference that are often produced due to the numerous transformations involved in conveying speech by telephone. 1,2 The fact that one cannot see the speaker and is consequently deprived of the information contained in facial expression, lip-read, and body language creates even more difficulty.
Multiple studies suggest that CI recipients encounter substantial difficulty communicating over the telephone. 2 -7 Telephone has long been a source of communication difficulty for the hearing-impaired population. It has been reported that 69% 7 of this population indicate that their hearing impairment many times discourages them from using the telephone. Also, 81% of them indicate that their hearing impairment has had a moderate to great effect on their use of the phone and affirm that hearing over the telephone is “somewhat” to “extremely” difficult. 7 Moreover, 94% of these patients reported that external background noise causes great difficulty in carrying on telephone conversations and people who use the telephone for business stated that hearing impairment has affected their work performance. 7
Several studies 8 -11 have been conducted to examine wireless connections between the telephone and hearing aids to improve speech intelligibility, and it is clear that this technology enhances speech recognition. In addition, Bluetooth technology is widely used in real life. It allows wireless communication between electronic devices with short-range wireless radio technology to connect devices with each other. These wireless technologies are developing in the hearing aid industry, and many commercially enabled hearing aids have been developed. 8 Recently, this technology has been implemented to the CIs, and Cochlear Ltd (Spain) and the GN Resound hearing aid company (Spain) formed a technology that enables a wireless connectivity between Cochlear Nucleus 6 (Spain) and Cochlear Baha 4 and 5 sound processors (Spain) and a Bluetooth streaming accessory (called Phone Clip) that may be used with mobile smart telephones. The Phone Clip receives the audio signal from the mobile phone and streams it directly to the user’s sound processor via digital radio frequency transmission. After digitalizing the audio signal, this wireless accessory utilizes a proprietary protocol to deliver the signal of interest to the receptor, supposedly making the audio signal clearer to the listener.
In a recent study, Wolfe et al 2,12 surveyed 16 adult users of CIs and evaluated the differences in word recognition over the mobile telephone in quiet and in competing noise in the acoustic mobile telephone condition compared to performance obtained with use of the CI sound processor and the wireless technology. They observed that the use of this kind of wireless device improves the word recognition over the mobile phone in quiet and in noise relative to performance in the acoustic mobile telephone condition.
The objective of our study was to evaluate speech perception improvement in a noisy environment through a Bluetooth phone accessory, implemented for CI users. We also evaluated the subjective satisfaction by analyzing participants’ responses on a satisfaction questionnaire and the effect of different mobile phone to microphone mixing ratios in speech recognition.
Patients and Methods
Participants
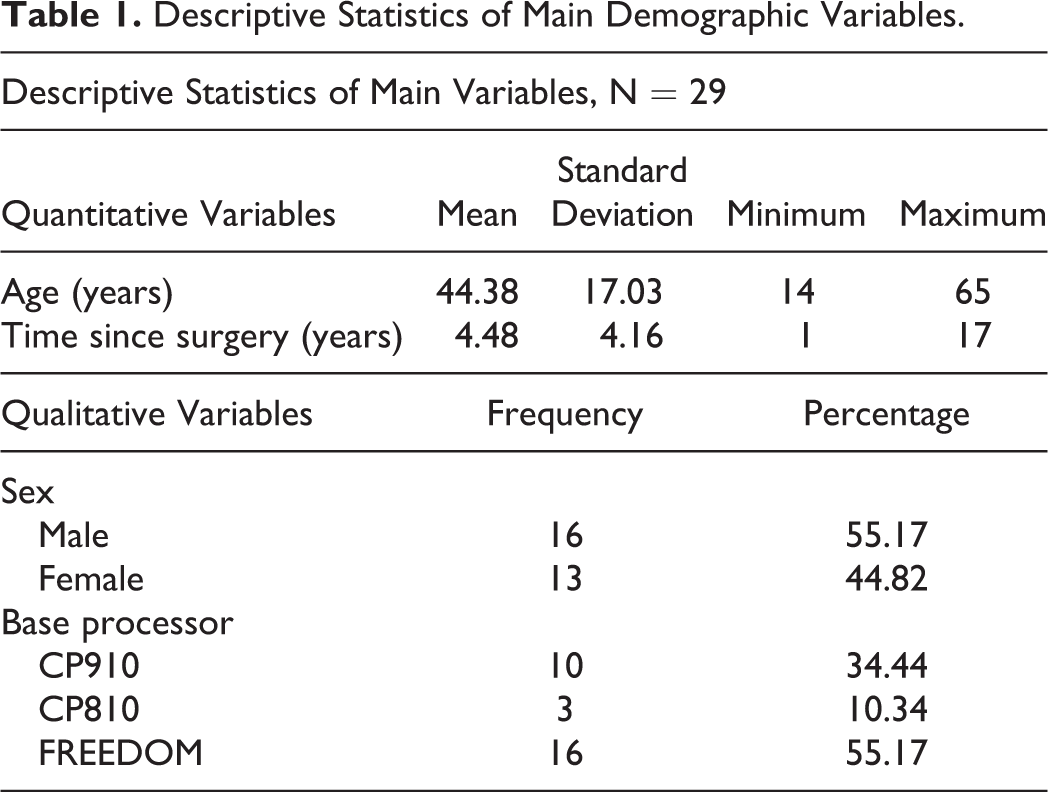
A total of 29 Spanish CI users were enrolled in a prospective comparison study. The Hospital Universitario Donostia’s institutional review board approved this study’s protocol, and a signed informed consent was obtained from all participants. All patients were aged between 14 and 65 years. Sixteen males and thirteen females were included and all of them had a stable map and more than 6 months of experience with their implant. All participants were implanted with a Cochlear Ltd implant and all of them were unilateral CI users without significant residual hearing on the contralateral implanted ear. Patients information is detailed in Table 1 and Figure 1.
Descriptive Statistics of Main Demographic Variables.
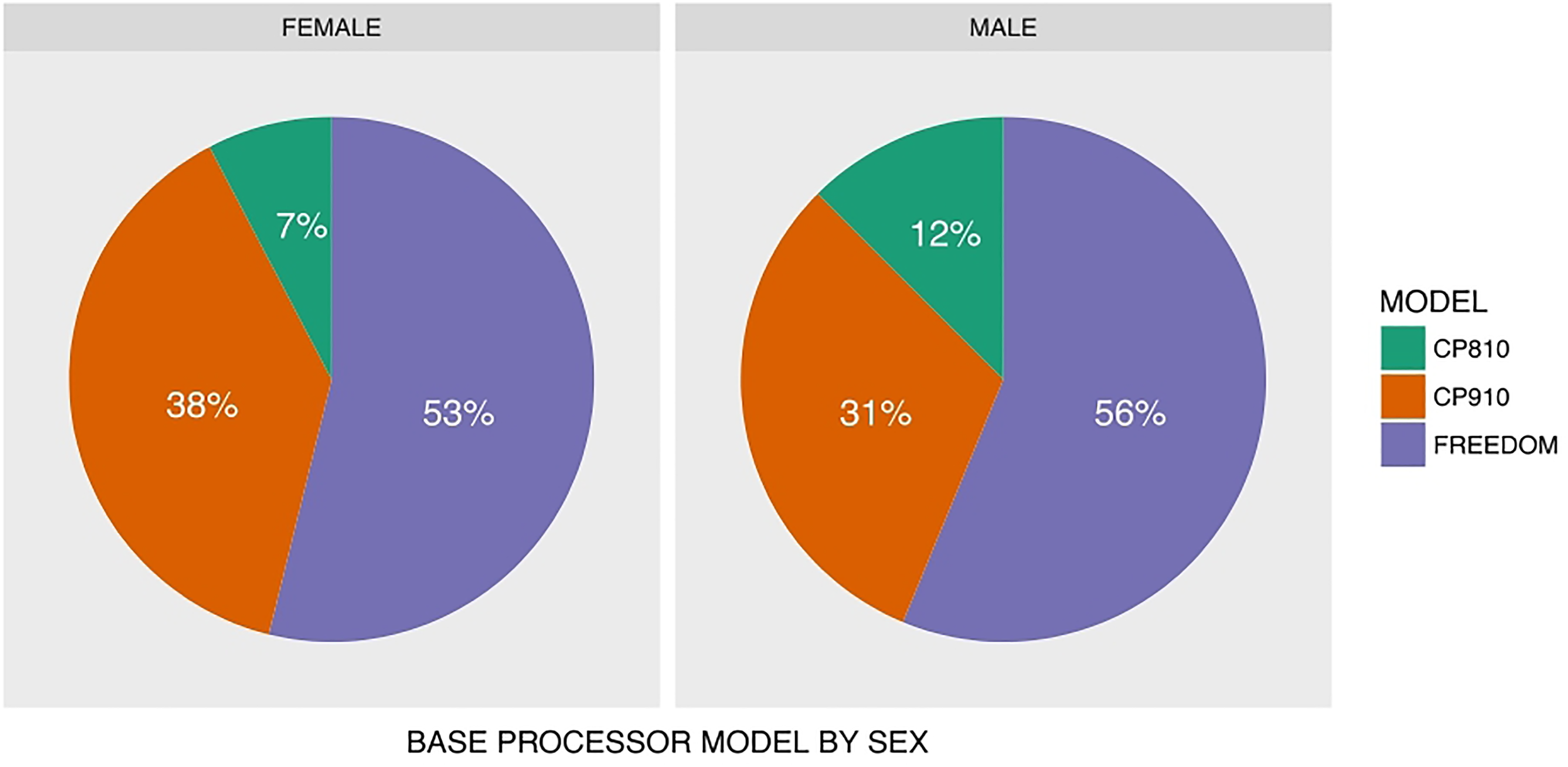
Descriptive sector plot with the base processor use by gender.
Equipment
All participants used the Nucleus 6 Sound Processor while participating in this study and all of them performed better than 60% in aided sentence recognition tests in quiet. Their speech recognition over the mobile was evaluated while they used the Nucleus 6 Sound Processor holding the mobile phone directly to the sound processor (acoustic way), with Phone Clip alone (with no other source of sound) and Phone Clip with different mixing sound ratios (2:1 and 4:1). These mixing ratios are defined in reference to the input proportion of mobile phone source versus the processor microphone source. In the 2:1 ratio, phone sound is mixed with microphone sound at 2 to 1 proportion. In the 4:1 ratio, phone sound is mixed with microphone sound at 4 to 1 proportion.
All tests were carried out in a soundproof room where a 65 dB SPL Spanish cocktail noise (defined as speech-in-speech, “cocktail party” situation with the spoken words in Spanish language) was generated continuously. Noise was produced from 4 loudspeakers located at the corners of the room, at 45-, 135-, 225-, and 315-degrees azimuth relative to the patient. The loudspeakers were placed at 1.57 m distance among them. As shown in the Figure 2, the participants were located in the center of the square and the distance from the participant to the loudspeaker was 1 m. The test room had an ambient noise level of 62 dB as determined with a Quest type 1 sound-level meter.
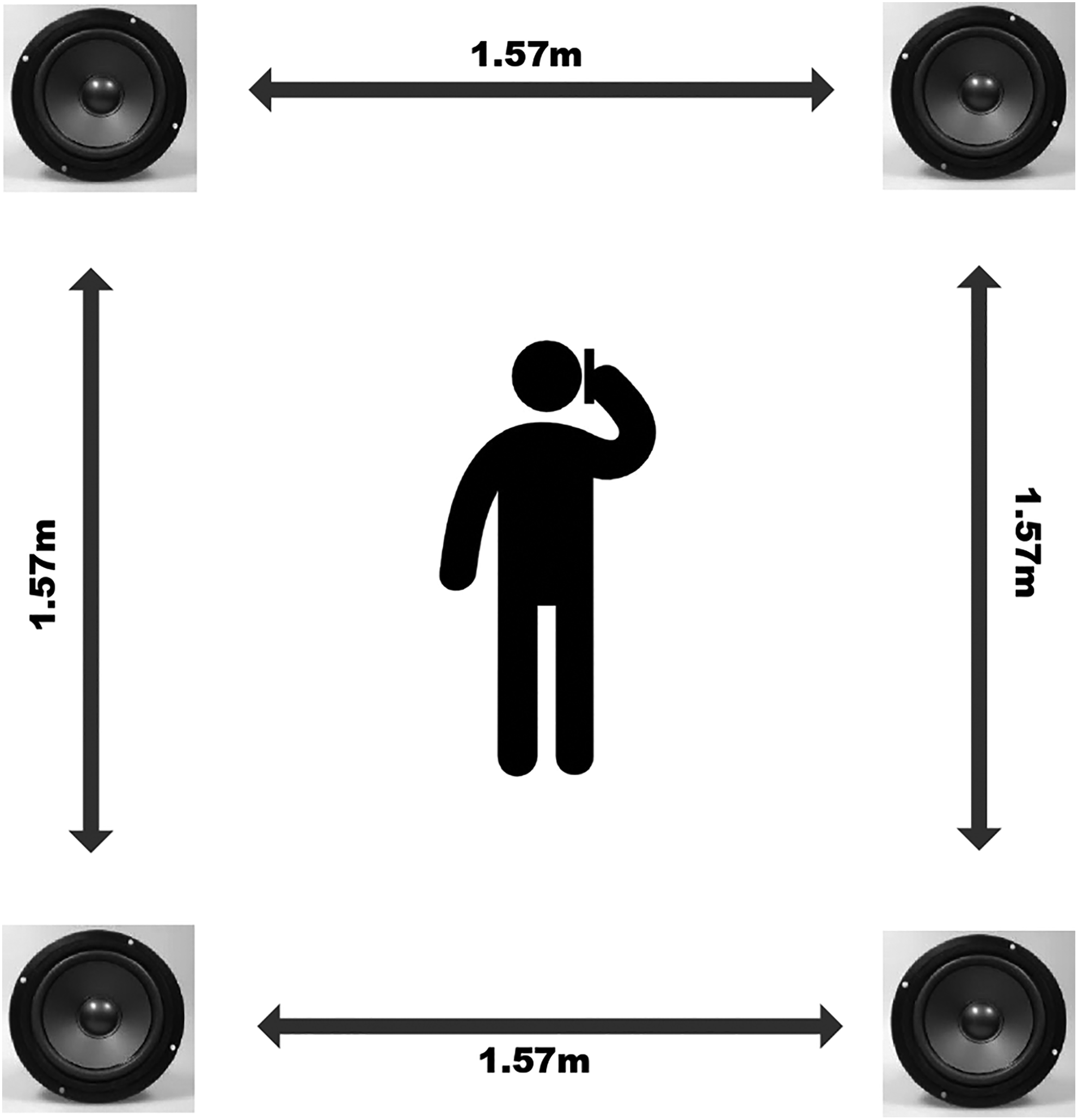
Disposition of the loudspeakers and the patient in the soundproof room.
Lists of 50 disyllabic words were presented through the clinic landline telephone to the patients’ mobile phone. The speech stimuli were presented through a compact disc (CD) player, which was coupled to a landline telephone by way of a handset interface (JK Audio Telephone Handset Audio Tap 2 or THAT-2 interface 4 ). Specifically, as shown in Figure 3, the THAT-2 interface was coupled at the same time to the CD player and to the landline telephone, in order to deliver the CD standardized disyllabic words from the clinic landline telephone to the participants’ mobile phone. Therefore, the THAT-2 interface was coupled to the audio output port of the CD player via 3.5 mm RCA audio plug auxiliary cable. Then, the phone output cable (RJ11) of the handset was coupled to the receiver handset input port of the landline telephone. This equipment setup allowed the delivery of recorded words from the landline telephone to wireless connected mobile phone on the testing room through a standard telephone to mobile phone call (Figure 3).
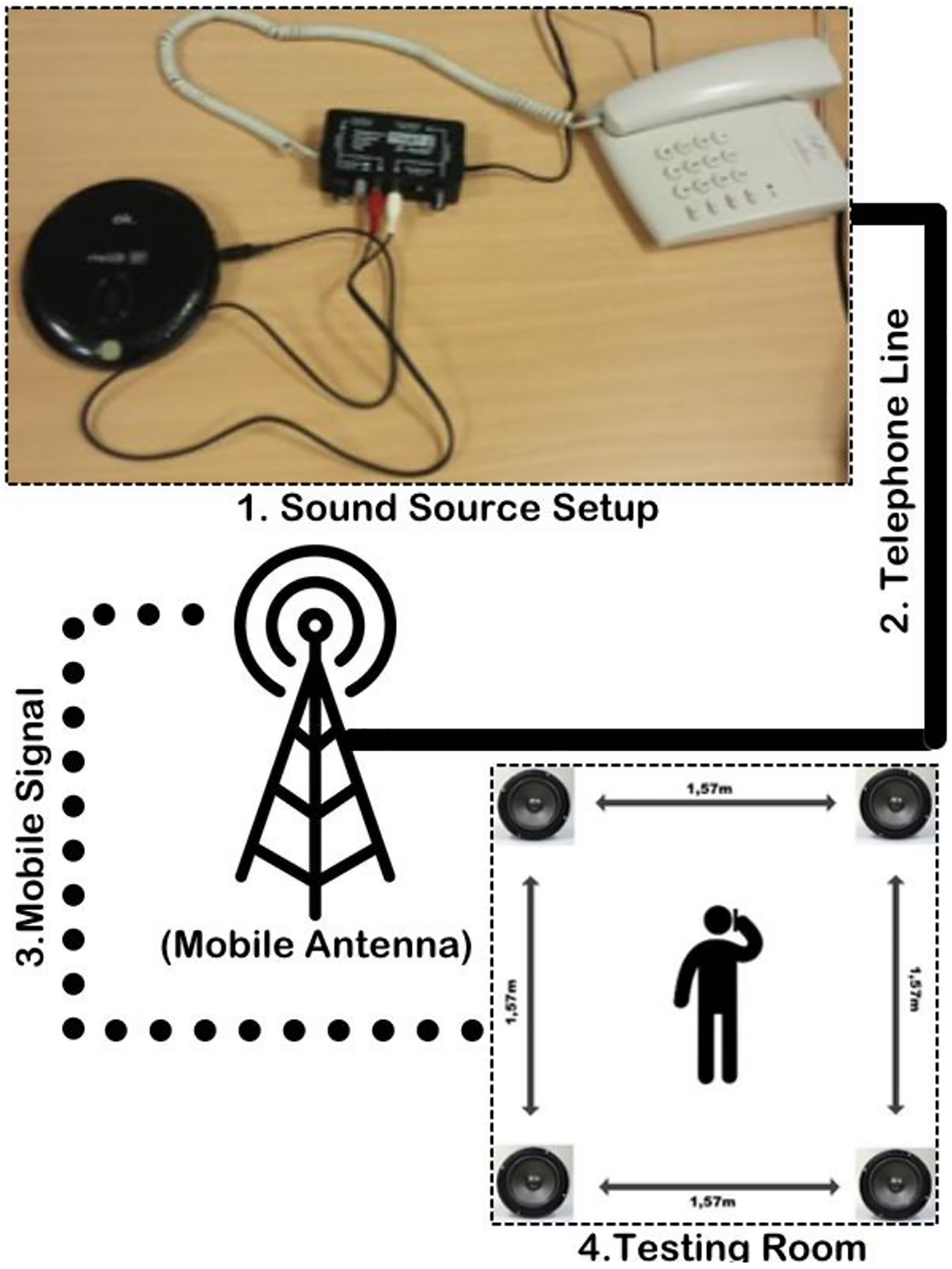
Landline telephone linked to the THAT-2 and mobile phone connection. THAT-2 indicates Telephone Handset Audio Tap 2.
A normal hearing individual could recognize in this situation (with the back Spanish cocktail noise in the soundproof room) all the disyllabic words, obtaining a 100% of disyllabic recognition with a tone threshold average (BIAP 1997) of 10 dB hearing loss (HL).
Testing Materials
Evaluation of speech recognition performance (objective measurement)
Word recognition scores were used for speech recognition performance. The standardized disyllabic words were derived from the Spanish version of standardized words for speech audiometry according to Huarte et al. 13 Spanish standardized disyllabic words are set in 20 blocks of 25 words each one. We used 8 blocks of 25 words, 2 blocks (50 words) for each situation was tested. Thus, when we tested using 2 blocks, the maximal sentence word recognition score is 50. We analyzed these results by percentage correct.
Questionnaires (subjective measurement)
Participants were asked to complete questionnaires before the test session. They completed the Kepler telephone usage questionnaire 7 (adaptation) and the Kim subjective satisfaction test. 8 After the test session, they completed again the Kim subjective satisfaction test using the Phone Clip. Most contents contained questions about their telephone using habits. The Kim questionnaires included subjective satisfaction about sound quality, noise interference, and accuracy naturalness, and all contents of this test used a visual analog scale. Maximal and minimal points of each parameter were +5 and −5, respectively.
The subjective measurement questionnaires described before were translated into Spanish by a bilingual audiologist, the translation method description and validation results were not published yet in actual literature.
Assessment Protocol
Following the fitting procedures described above, each participant was tested in 4 listening conditions, always with back cocktail noise and delivering through the participant mobile phone the standardized Spanish disyllabic words. After listening a word, the participant had to repeat it and the observer on the other side of the telephone line registered the participant’s answer.
First, we tested the disyllabic recognition while the participants were holding the phone next to the microphone of the sound processor, in the way the participant uses it in real life.
Second, we paired the new Cochlear Phone Clip with the participants Nucleus 6 Sound processor using different mixing ratios (proportion of signal coming from the accessory vs the sound processor microphone) and tested them in 3 different situations: 2:1, 4:1, and only with the Phone Clip. Finally, the participants completed the Kim questionnaire to investigate subjective satisfaction with the Phone Clip.
Statistical analysis
All the data were analyzed using STATA 13.0 (StataCorp 2013, Stata Statistical Software: Release 13, College Station, Texas) and R 3.4.2 (R Core Team. 2017, R: A language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/) statistical programs. Percentages of word recognition score in each test condition (without Phone Clip, with Phone Clip 2:1 mixing ratio, 4:1 mixing ratio, and only Phone Clip) were assessed using repeated-measurements analysis of variance (ANOVA) test with Tukey post hoc test to compare each measurement protocol results. In addition, the subjective satisfaction of each parameter, such as sound quality, noise interference, and accuracy naturalness, was analyzed using paired tests according to whether wireless or conventional mode. The statistical level of significance was defined as a P value of less than .05.
Results
Twenty-nine participants met the inclusion criteria. All participants had more than 6 months experience with their CIs and stable maps. All of them were unilateral CI users. Age range was 14 to 65 years, with a mean age of 44.4. Thirteen patients were women (44.8%) and 16 (55.2%) were men. The mean time since implantation was 4.48 years (standard deviation [SD]: 4.16). The mean sentence recognition in the speech audiometry in silence was 94.3% (SD: 0.85). Data are detailed in Table 1 and Figure 1.
Improvements in Speech Recognition Performance (Objective Measurement)
The average number of correct words without Phone Clip was 16.17 of 50 words (SD: 9.11). The average number of correct words with Phone Clip mixing ratio 2:1 was 21.89 (SD: 8.42), with Phone Clip mixing ratio 4:1 was 25.75 (SD: 7.80), and finally, the average number of correct words with only the Phone Clip (the whole acoustic signal entries from the Phone Clip, no signal comes from the microphones) was 27.86 of 50 words (SD: 9.72). Measured results are plotted on in Figure 4.
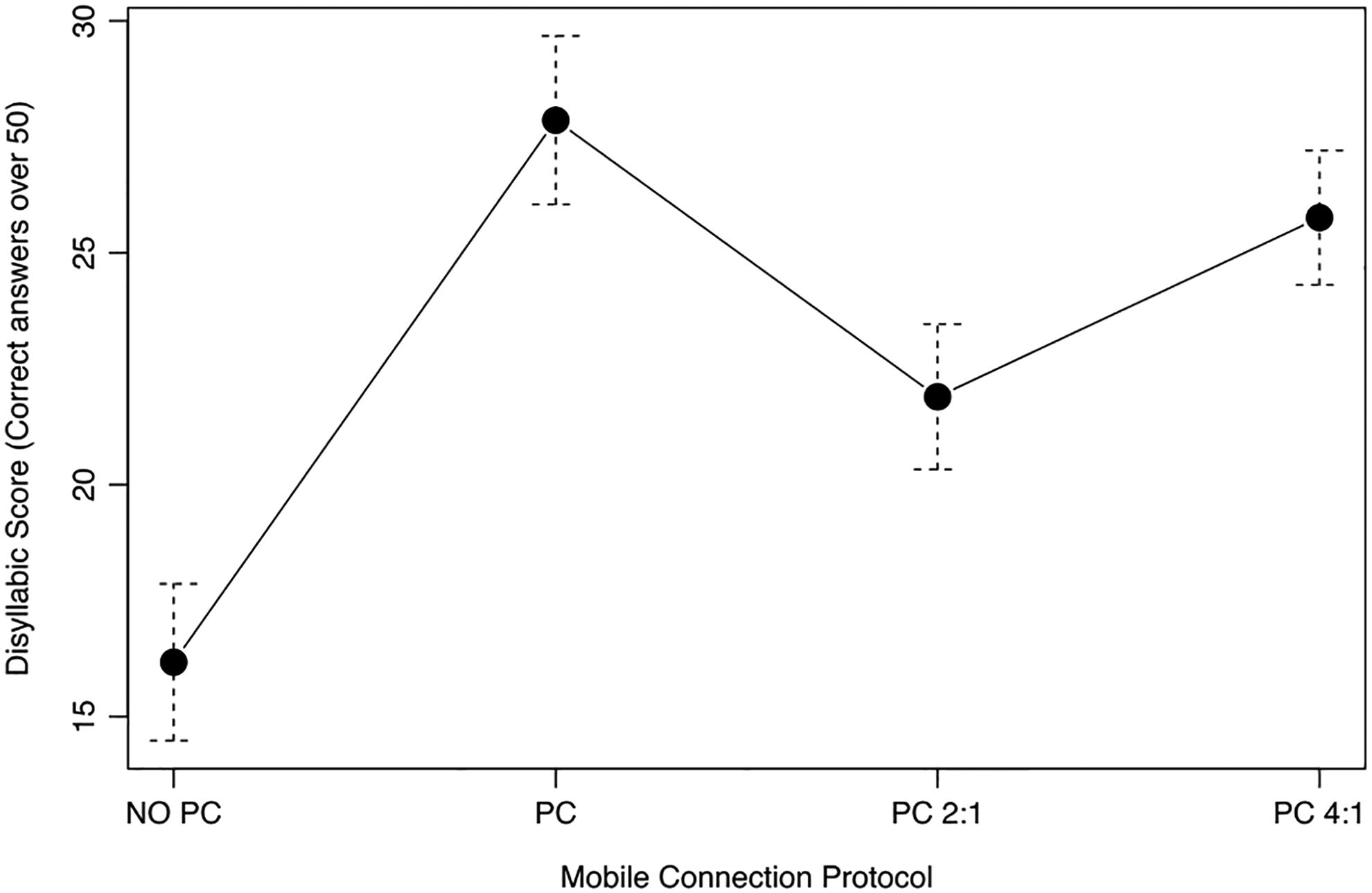
Mean with 95% confidence interval for dissyllabic words understanding in noise without Phone Clip, with Phone Clip and input microphone at various mixing ratio, and with Phone Clip only. No PC indicates no Phone Clip condition; PC, Phone Clip without Processor microphone sound mix; PC 2:1, Phone Clip with 2:1 sound mix ratio; PC 4:1, Phone Clip with 4:1 sound mix ratio.
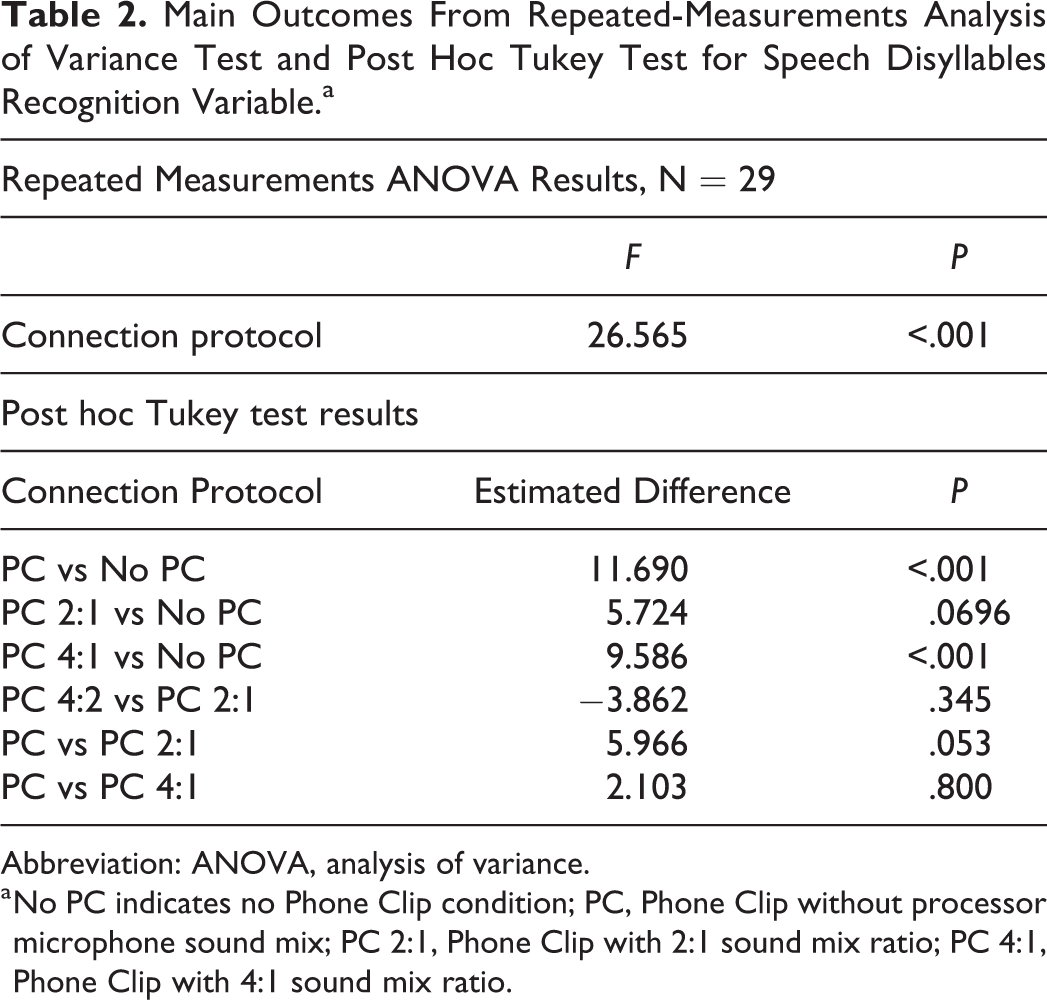
Repeated-measurements ANOVA show that statistically significant (P < .001) word recognition performance differences were found in the 4 different situations (no Phone Clip, Phone Clip 2:1, Phone Clip 4:1, and only with Phone Clip; Table 2). Post hoc Tukey test shows statistical differences of wireless transmission compared to the conventional mode (no Phone Clip), no Phone Clip shows significant decreased recognition score versus the Phone Clip without sound mixing (P < .001), significant decreased recognition versus Phone Clip with 4:1 sound mixing ratio (P < .001), and tendency to statistical significance decreased recognition versus Phone Clip with 2:1 sound mixing ratio (P = .069). Therefore, obvious improvement of speech recognition performance was found in cell phone usage by wireless transmission.
Main Outcomes From Repeated-Measurements Analysis of Variance Test and Post Hoc Tukey Test for Speech Disyllables Recognition Variable.a
Abbreviation: ANOVA, analysis of variance.
a No PC indicates no Phone Clip condition; PC, Phone Clip without processor microphone sound mix; PC 2:1, Phone Clip with 2:1 sound mix ratio; PC 4:1, Phone Clip with 4:1 sound mix ratio.
Subjective Measurement
With the Kepler telephone usage questionnaire, we observed that in 63% of our sample, the HL prevented them from using the telephone at all. We also verified that the hearing impairment discouraged from using the phone to the 70% of our patients.
As shown in Figure 5, in 80% of our participants, the deafness has a moderate to great impact on their usage of the telephone without Phone Clip. In fact, in 27% of our participants, deafness had a moderate impact on their usage of telephone, in 27% this impact was high and in 27% the impact was defined as “great impact.” We also confirmed that 70% of our sample felt that other people reported their hearing impairment over the telephone. In addition, we observed that 69% of the implanted patients found hearing over the telephone very difficult and 76% had to end a phone call before the conversation was completely finished because they had difficulty understanding.
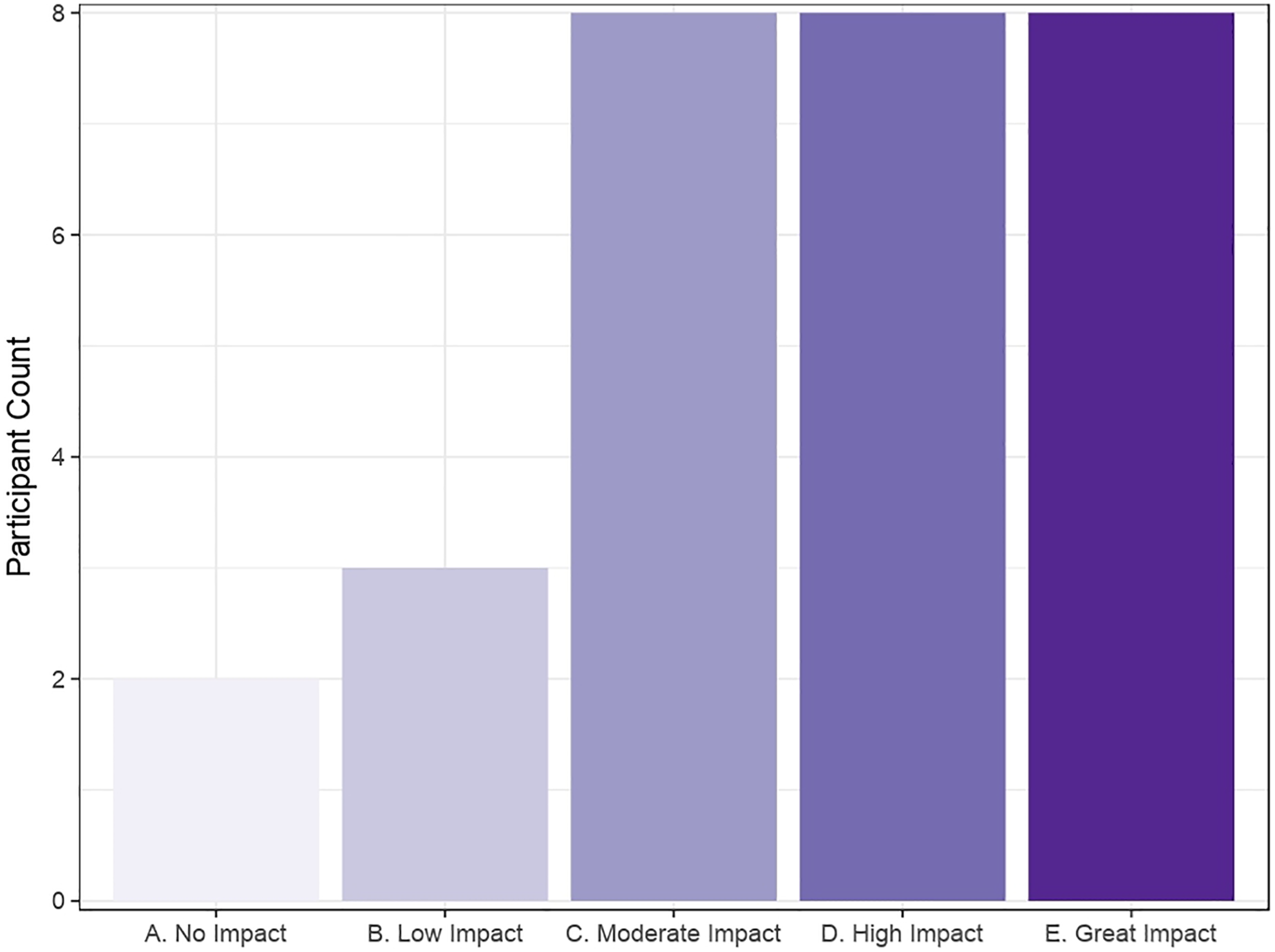
Number of patients categorizing themselves according to Kepler questionnaire.
Furthermore, we verified that when using the telephone in a noisy environment, 17% of our patients reported having high difficulty or great difficulty 76% of the times in hearing the person on the telephone. In our study, we observed that our implanted population avoided using the telephone and 51% of them usually placed on average less than 3 outgoing calls per day.
Subjective Preference of Wireless Sound Transmission
The participants were asked whether they preferred acoustic-free field transmission (conventional mode) or wireless transmission (with Phone Clip). We analyzed 3 items in subjective satisfaction: sound quality, noise interference, and accuracy naturalness. Figure 6 shows the subjective satisfaction scores expressed in a visual analog scale from −5 to +5 with and without Phone Clip. We found statistically significant differences (P < .001) in the subjective satisfaction of the Bluetooth-implemented CI device compared to the conventional mode in the following 3 items.
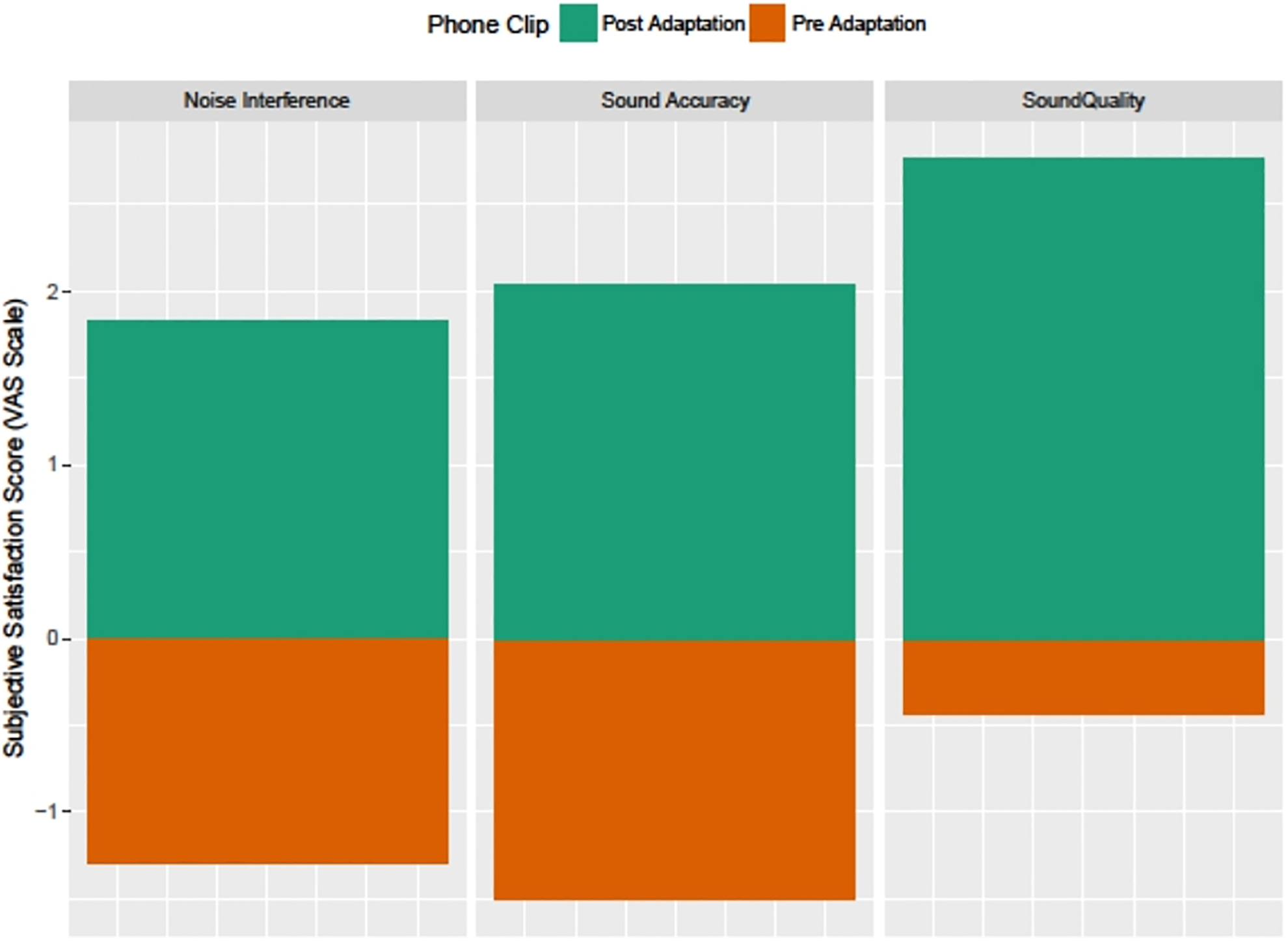
Patient subjective satisfaction score about acute Phone Clip usage: score given on visual analog scale ranging from −5 to 5 (right).
Sound quality
In our study, sound quality was defined as the physical pleasure or fatigue experienced by a listener. Therefore, sound quality was determined by pleasantness or unpleasantness of the sound. Statistically significant benefits of the wireless transmission to the CI were observed (P < .001). We analyzed using a paired Student t test and mean sound quality observed without wireless transmission was −0.43 (SD: 0.42) and the mean mark after the use of the wireless device was +1.83 (SD: 0.47) in a scale ranging from −5 to +5. The mean difference between both situations was 2.26 points better with the Phone Clip device.
Noise interference
In our study, noise interference meant mostly background noise. In the analysis of satisfaction about noise interference, we achieved statistically significant benefits with wireless transmission (P < .001). We also analyzed using a paired Student t test and mean noise interference observed without wireless transmission was −1.5 (SD: 0.49) and the mean rating using the wireless device was +2.76 (SD: 0.56) in a scale ranging from −5 to +5. The mean difference between both situations was 4.26 points better with the device.
Accuracy naturalness
We defined accuracy naturalness by naturalness of sound. Statistically significant satisfaction improvement in accuracy naturalness by using the Bluetooth-implemented device was observed (P < .001). We checked it with a paired Student t test and mean accuracy naturalness observed without wireless transmission was −1.3 (SD: 0.48) and the mean rating using the wireless device was +2.03 (SD: 0.45) in a scale ranging from −5 to +5. The mean difference between both situations was 3.33 points better with the device.
Discussion
Nowadays, use of the telephone is necessary in daily life many times. However, hearing-impaired people often have difficulty communicating over the telephone. 1,3 -6 These obstacles with the telephone communication may affect their social lives as well as their performance at work.
The intelligibility of telephone speech is considerably lower than the intelligibility of face-to-face speech. This is partly because of lack of visual cues, limited telephone bandwidth, and background noise. 1,2 In addition, cell phones may cause interference with the CI.
On the other hand, several studies 8 -11 have examined wireless connections between the telephone and hearing aids to improve speech intelligibility and it is clear that this technology enhances speech recognition. Moreover, Bluetooth technology is widely used in real life, allowing wireless communication between electronic devices.
To address the problems that hearing-impaired people experience with telephones, this article examines a wireless device (Cochlear Wireless Phone Clip) that can route the audio signal directly to the CI processor. The Cochlear Phone Clip may be paired with a Bluetooth-enabled electronic device as a smartphone. Once the coupling is complete, the Cochlear Phone Clip receives the audio signal and streams it direct to the Nucleus 6 Sound Processor.
We used the Kepler telephone usage questionnaire (adaptation) and the Kim subjective satisfaction test to assess the difficulties that our implanted participants experiences with the telephone usage during their daily lives. We found that without the Phone Clip, 80% of the CI users were moderately to greatly negatively impact on the telephone use because of their hearing impairment. We are aware that one limitation to our subjective test findings is that the translation method used in the present study is not validated and published; this should be considered in future studies. We consider that because of the concordance between the positive results obtained in these questionnaires and the positive results obtained with the disyllabic recognition objective test make that this limitation of validation in Spanish-translated tests probably has a low effect in the present study results for subjective assessments.
After the use of the Phone Clip, the participants were asked to fulfill again the Kim subjective satisfaction test, in order to determine whether they preferred acoustic-free field transmission (conventional mode) or wireless transmission (with Phone Clip). Statistically significant improvement (P < .001) was observed in subjective patient satisfaction when using the Phone Clip for the following 3 measurements: sound quality, noise interference, and sound accuracy.
In addition, statistically significant (P < .001) improvement of speech recognition performance was found using cell phone in noise. We also observed that changing mixing ratio does impact speech understanding, so that proper counseling is necessary to adapt to each participant’s needs.
In this study, we investigated how different mixing ratios affected the speech recognition. We observed that there are a significant and tenant to significance differences between 4:1 and 2:1 with the no Phone Clip condition (P < .001 and P = .06) and we also observed that there is no difference between 4:1 and 2:1 conditions (P = .345). These results suggest that the recipient could use the 4:1 and 2:1 ratios with a significant improvement of the speech recognition allowing to the recipients to not be isolated from the environment sounds, which should produce a more comfortable hearing experience that should be investigated on future studies.
Our data show that this Bluetooth-implemented device could be beneficial for speech recognition performance in the use of the telephone in CI recipients. To our knowledge, wireless transmission could have an advantage for the use of electronic devices in the cochlear-implanted patients. 2 As discussed before, our results suggest that better speech recognition compared with other manual connection methods (holding the mobile phone directly to the sound processor), this is probably related with the lower noise level of the wireless transmission. Also, acoustic coupling sound between the telephone speaker and the processor microphone is avoided in the Bluetooth connection method; these advantages (in noise and coupling sound reduction) will probably improve the mobile phone user experience in CI recipients.
In conclusion, it is clear that many implanted have difficulties over the telephone. Recently, Bluetooth technology has been developed and widely used in real life and it allows wireless communication between electronic devices. Furthermore, this technology has been successfully implemented to the hearing aids. These wireless technologies have been now developed in the CI industry. The wireless Phone Clip© device helps implanted people to improve subjective and objective speech recognition performance through the phone in noisy environments. This a step forward for CI users, which may impact their quality of life as well as their efficiency at work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.