
Abstract
Objectives:
Mastoid reconstruction principle had been described to overcome problems of chronic discharging cavity. Different materials were used; nonbiologic materials seem to be less preferred. Platelet-rich plasma (PRP) could promote the regeneration of mineralized tissues. In this work, the authors present a simple and easy technique for mastoid reconstruction with PRP and cortical bone pate.
Methods:
The study design is a case series. Patients had mastoid reconstruction after canal wall down mastoidectomy using PRP and cortical bone pate.
Results:
This study included 21 patients: 9 males, and 12 females. Sixteen patients had left side disease. All surgical procedures were conducted smoothly within 90 to 135 minutes with no stressful events had been reported. At 12 to 16 months of follow-up, external canal stenosis and mastoid fistulas were not reported. Good healing of the tympanic membrane was seen in 18 patients. No radiological signs suggestive of recurrence were detected and the reconstructed mastoid cavity was smooth and well aerated. Residual tympanic membrane perforations were detected in 3 patients.
Conclusion:
Autologous materials (PRP and bone pate pate) after canal wall down mastoidectomy appear to be a reliable and effective choice for mastoid reconstruction.
Introduction
Canal wall down (CWD) mastoidectomy aims to provide a safe, dry, and “self-cleaning” ear. However, chronic discharging cavity with frequent cleaning of offensive debris and unsightly meatoplasty are the main concerns after CWD mastoidectomy. 1 -5 Mastoid reconstruction principle had been described to overcome these problems and different materials were used; these materials can be classified into: (1) free grafts (biologic and nonbiologic) and (2) local flaps. 4 -10 All of these techniques have their advantages and disadvantages but nonbiologic materials seem to be less preferred. 1,2,6 Platelet-rich plasma (PRP) is a simple laboratory method to obtain a high concentrates of autologous growth factors. Platelet-rich plasma could accelerate tissue regeneration and promote soft tissue healing; thus PRP was used in soft tissues otological procedures with good results. Platelet-rich plasma could promote the regeneration of mineralized tissues; however, it was not widely studied for reconstruction of mastoid cavities in the available English literature. 4,9 -12
In this work, authors present a simple and easy technique for Mastoid reconstruction (MR) (in selected group of patients) via autologous tissues: PRP and cortical bone pate.
Patients and Methods
Patients
This case series was conducted from April 2015 to May 2019 at the Otorhinolaryngology–Head and Neck Surgery Surgery Department, Zagazig University, Egypt. The study was conducted according to the Declaration of Helsinki on Biomedical Research Involving Human Subjects. Participants were not exposed to any physical, psychological, or social harm. It included adult patients with chronic suppurative otitis media who needed CWD mastoidectomy. Patients with complicated otitis media and labyrinthine fistula were excluded from the study. Also, we excluded patients who had previous otological surgeries or had trials for mastoid reconstruction. The follow-up period ranged from 34 to 47 months (mean = 38 ± 2.9 months).
Methods
After written informative consent, detailed history and general/head and neck examination were offered. Full otological evaluation (including otomicroscopic examination) followed. Pure-tone audiometry thresholds were determined and the air–bone gaps were calculated. Computed tomography (CT) scanning of the temporal bone was requested for all patients, aiming at detection of the disease, definition of surgical landmarks, and to record external canal size. All patients had mastoid reconstruction after CWD mastoidectomy performed by (or under direct supervision) the senior author.
Surgical Procedure
The procedure began via a postauricular incision. Cortical bone pate was collected and CWD mastoidectomy was performed. Temporalis fascia graft was then harvested and PRP was prepared; 5 mL of peripheral venous blood was drawn from the patient with a 16- to 18-gauge syringe. The collected blood was put in 5-mL tubes (without an anticoagulant or calcium). Tubes were immediately centrifuged in a tabletop centrifuge (Low Speed Centrifuge [800]; Jiangsu Zhengji Instruments, Jiangsu, China) machine for 12 minutes at 3200 rpm. Blood would separate into the 3 layers: the bottom layer (red blood cells), the middle layer (PRP; platelets and white blood cells), and the top layer (platelet-poor plasma) The PRP layer was extracted just before application (Figure 1). 9 -11 If needed, a piece of cartilage was employed for ossiculoplasty. The bone pate was applied over the walls of mastoid cavity as a carpet and then PRP plug was put comfortably in the mastoid cavity (Figure 2). Temporalis fascia graft was used to reconstruct the tympanic membrane (TM) perforation. An external meatal pack was placed. The postauricular incision was closed in layers.

Right: PRP tube. Left: Extraction of PRP plug. PRP indicates platelets rich plasma.
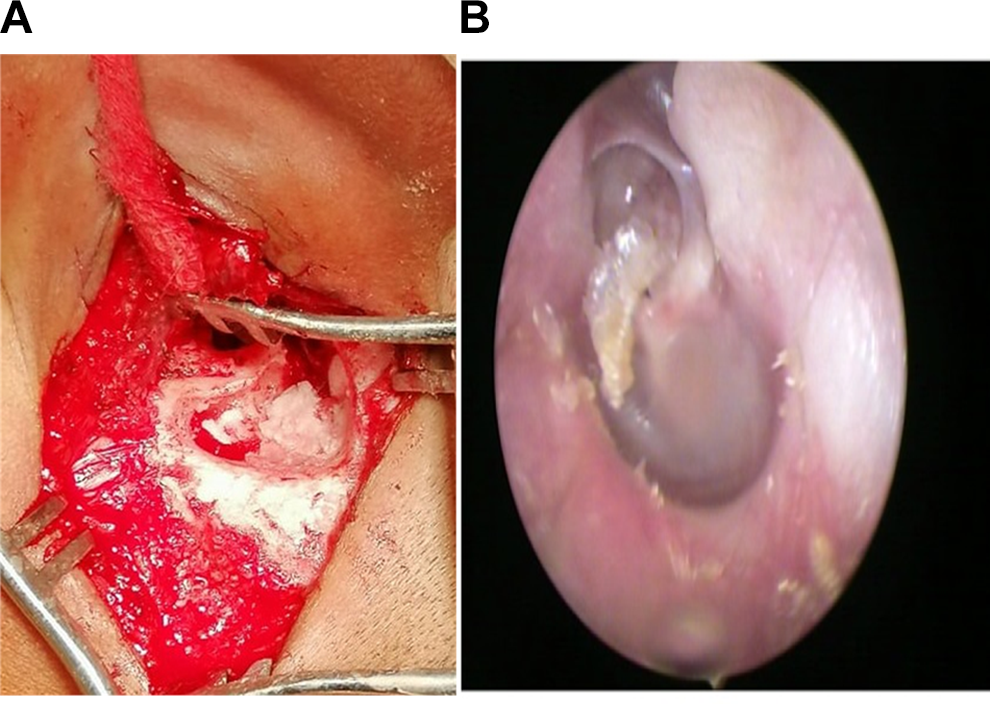
A, Reconstruction of mastoid with PRP and bone pate. B, Tympanic membrane and external auditory canal at 1 year follow-up. PRP indicates platelets rich plasma.
Postoperative Follow-Up
All patients were sent home in the following morning. Packs, dressings, and stitches were removed 7 to 10 days postoperatively. Otoendoscopic examinations were performed weekly for the first month, then monthly for 3 months, then every 3 months till the end of follow-up. Pure-tone audiometry and CT were requested 10 to 12 months postoperatively.
Statistical Analysis
Preoperative and postoperative evaluation results were compared using SPSS program version 20.0 (Chicago, Illinois). Numerical data were represented by median and range. Wilcoxon signed-rank test was used as a nonparametric test to compare different variables. When P value is <.05, it was considered statistically significant.
Results
Patient Characteristics
This study included 21 patients: 9 (42.86%) males and 12 (57.14%) females. The mean age of the patients at the operation was 31 (±7.2 SD) years (range: 19-55 years). Most of the studied patients had a unilateral disease; the left side was dominant (16 [76.19%] patients). Three (14.29%) patients had bilateral disease. We only operated one ear at a time.
Preoperative Evaluation
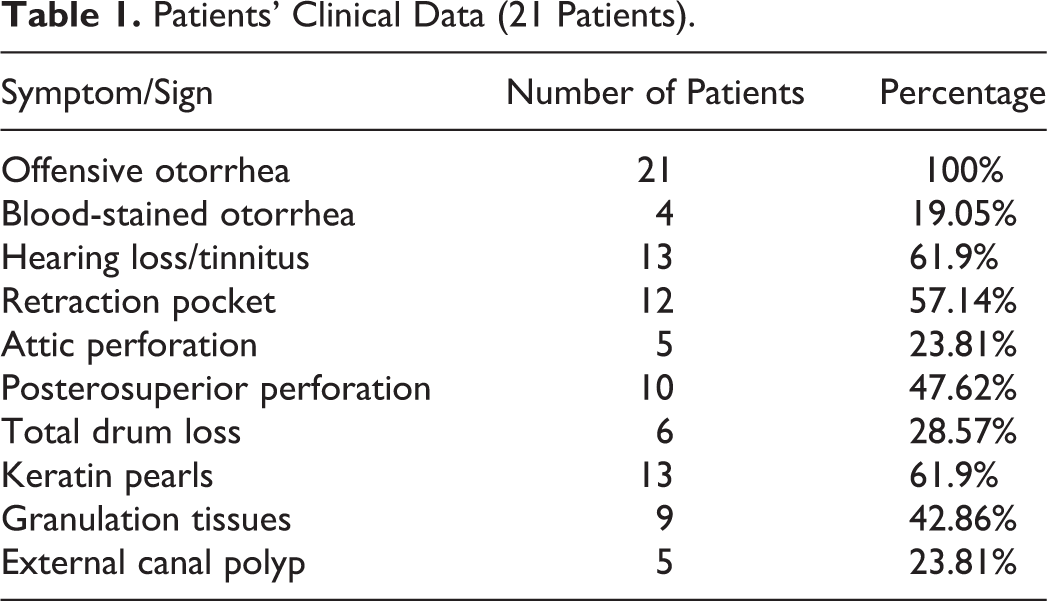
All included patients complained of persistent offensive discharge (4 of them had blood-stained discharge). Basic clinical and otomicroscopic examination data are presented in Table 1. Retraction pockets were the commonest finding (57.14%). Air–bone gaps ranged between 25 and 45 dB (with a mean of 32 ± 2.1 dB). Preoperative CT scans show soft-tissue mass with varying levels of bone erosion or destruction in 12 (57.14%) patients. Sclerotic mastoid was described in 8 (38.1%) patients. Outer attic wall destruction was seen in all studied patients. Ossicular necrosis was detected in 12 (57.14%) patients.
Patients’ Clinical Data (21 Patients).
Operative Data
Included patients had mastoid reconstruction via PRP and bone pate after CWD mastoidectomy. All surgical procedures were conducted smoothly within 90 to 135 minutes (mean = 102 ±3.7) with no stressful events had been reported. Cartilage ossiculoplasty was performed in 12 (57.14%) patients.
Postoperative Evaluation
The early postoperative period (4-6 weeks) had passed smoothly. There were no reports of wound infections, dehiscence, or hematomas. Nine (42.86%) patients complained of altered taste sensation; it was trivial and disappeared within 4 to 6 months.
At 12 to 16 months of follow-up, external canal stenosis and mastoid fistulas were not reported. Good healing of the TM was seen in 18 (85.71%) patients (Figure 2). In all patients, no CT signs suggestive of recurrence were detected and the reconstructed mastoid cavity was smooth and well aerated (Figure 3). One (4.76%) patient had recurrent discharge; it was not offensive and was managed successfully by topical antibiotic/steroid ear drops for 7 days. Residual TM perforations were detected in 3 (14.29%) patients. Two patients were prepared for revision surgery to close the TM perforations; during surgeries, no keratin pearls nor granulation tissues were detected and closure of the perforation was successfully accomplished via perichondrial grafts.
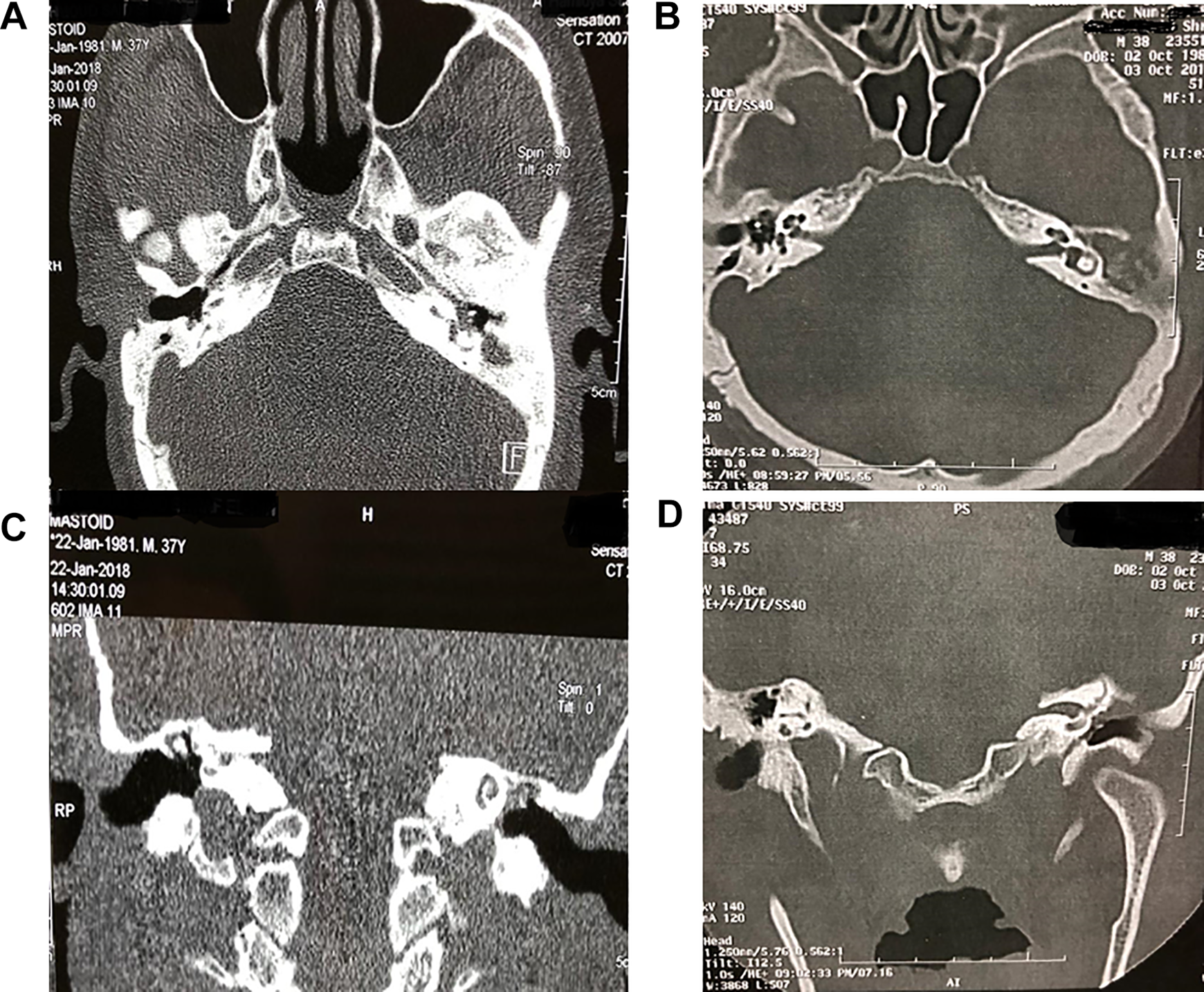
Preoperative CT: (A) axial and (C) coronal cuts, showing opacity in the attic and mastoid antrum with erosion of outer attic wall and ossicular necrosis (left ear). Postoperative CT: (B) axial and (D) coronal cuts, showing reconstruction of mastoid with autologous tissues: PRP and bone pate (left ear). CT indicates computed tomography; PRP, platelets rich plasma.
Discussion
Canal wall down mastoidectomy techniques are associated with low rates of recurrent disease, but the risks of discharging cavity problems are frequently reported (20% to 60%). 1,2,5 The basic idea of mastoid reconstruction is that it could prevent cavity problems and the collapse of reconstructed posterior canal wall. Mastoid reconstruction techniques also lessen the development of postauricular skin depression, improve the aesthetic appearance, and a future hearing aid could be fitted comfortably. 1 -5
Background
The ideal procedure for MR should be simple, easy, and quick to do with fast learning curves and unique results. The new cavity should heal quickly and promote complete epithelial lining of the mastoid cavity, leading to a safe, dry, and self-cleaning ear. There should be minimal complications. The created cavity should be easy to inspect for the detection of recurrent disease. Unfortunately, such a perfect solution is yet to show up. 1 -6 The chosen surgical procedure should be tailored to the patient’s condition, size of mastoid cavity, and surgeon’s experience. 1,2,4
Materials for Mastoid Reconstruction
Different materials were used; they can be classified into 2 main categories: (1) free grafts (biologic and nonbiologic) and (2) local flaps. All of these materials have their advantages and disadvantages, but nonbiologic materials seem to be less preferred. Autologous tissues (cartilage, cortical bone pate, and bone chips) were mentioned with good results. 1 -8
The PRP in Otology
Platelet-rich plasma has a high concentration of platelets and normal concentration of fibrinogen. The high concentration of platelets could promote wound healing and tissue sealing; thus, it had been used by otologists in TM perforation and good results were obtained. Platelet-rich plasma had been shown to stimulate the mitogenic activity of human trabecular bone cells. It could increase the proliferation rate of human osteoblast-like cells and stromal stem cells; therefore, it promotes the regeneration of mineralized tissues and induces bone growth. 9 -12 Accordingly, we thought it would be reasonable to use it for mastoid cavity reconstruction.
Our Technique: Idea and Pre- Versus Post-Operative Results
In our study, we present a simple, safe, easy, and effective technique of reconstruction of mastoid cavity after CWD mastoidectomy. Authors used autologous tissues: PRP and cortical bone pate. The current study reported a high efficacy rate with no reported complications; a total success rate was more than 85%. No postoperative wound infections were reported. These results are compatible with other works. 1 -5 Another important point to be mentioned (as regard the use of self-materials) is that it has no reaction, thus (in case of recurrence) no hazards of hidden disease.
The proposed technique is readily available, less costly, and economic. This point has the utmost importance in developing countries with limited health budgets. However, the evident limitation of MR techniques is the requirement for the surgeon to ensure complete removal of the cholesteatoma matrix from the entire mastoid cavity.
Points of Strengths
The strength of this study lies in its prospective nature, which allowed data to be assessed without depending on patient recollection or registration faults. Statistical analysis could provide data validation.
Limitations
The current study has limitations, for example, the number of participants was not quietly enough to judge the technique efficiently and the results were not analyzed in a blinded manner. Another limitation was the lack of a control group; however, our basic target was to assess the postoperative results as a preliminary report. Gained data reflects the experience of a single surgeon (at a single institution). Future multicenter comparative studies with longer follow-up periods are recommended.
Conclusion
Autologous materials (PRP and bone pate pate) after CWD mastoidectomy appear to be a reliable and effective choice for mastoid reconstruction. Those materials improve healing and give a smooth appearance to the mastoid cavity. No considerable complications were reported. The results provide a useful platform for future wider research works.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.