
Abstract
Despite its effectiveness, radiochemotherapy treatment in the head and neck region is accompanied by acute oral complications such as oral mucositis, dysphagia, xerostomia, and dysgeusia. The aim of this study was to analyze and prospectively assess the frequency and evolution of acute oral complications during radiochemotherapy in patients diagnosed with squamous cell carcinoma in the head and neck region. We have analyzed oral complications of 20 patients during 6 weeks of radiochemotherapy treatment for squamous cell carcinoma. Oral mucositis was evaluated according to the World Health Organization criteria, dysphagia, and dysgeusia according to the National Cancer Institute Common Toxicity Criteria, and xerostomia according to parameters set by the Seminars in Radiation Oncology. Mucositis was first observed in the second week and all patients presented some degree of mucositis in the fourth week of radiotherapy. Xerostomia and dysphagia were initially reported already in the first week of radiotherapy. All patients presented xerostomia in the fourth week; however, dysphagia was observed in all patients, only in the sixth week. Dysgeusia was first observed in the second week, becoming more severe in the third week. Acute oral complications can be observed throughout the treatment, but the third week of radiotherapy seems to represent a critical week, regardless of the grade of the complication. The sixth week presents the worst grades of these complications. Knowledge about the natural course of oral complications during radiotherapy is important to develop better strategies for treatment and improve the patients’ quality of life.
Introduction
The radiotherapy (RT) is a well-known antineoplastic modality for malignant tumors in the head and neck region. This oncological treatment is capable of providing high rates of tumor control. However, despite its effective results, RT is accompanied by painful and debilitating acute oral complications such as mucositis, xerostomia, dysphagia, and dysgeusia, since RT also affects radiosensitive tissues located close to the tumor. 1 -4
Oral mucositis is an acute complication described as a toxic inflammatory reaction of the oral mucosa caused by cytoreductive treatment induced by RT and/or chemotherapy. 5,6 Patients may experience edema, erythema, ulcer, and pseudomembrane formation, resulting in burning symptoms which may progress to intense pain and consequent impairment in feeding and verbal communication. 4 -8 More than 95% of the patients undergoing radio/chemotherapy in the head and neck region develop some degree of oral mucositis. 2,5,7 In severe cases, it may cause dehydration, weight loss (15%), hospitalization (16%), and modification or discontinuation of the treatment due to debilitation of the patients. 5,8 -11 Oral mucositis usually occurs in patients in the second week of RT, and the severity increases along the weeks of RT reaches its peak around the fifth and sixth weeks of treatment. 4,5,9 -13
Xerostomia is also a major acute complication caused by possible destruction of the glandular parenchyma, leading to insufficient or no secretion of saliva. Xerostomia can also be characterized by saliva thickening and pH change due to the fact that serous acini are the first to undergo alterations in response to RT. 4,12,13 Xerostomia causes discomfort to patients, such as dry lips, oral mucosal burning, changes in the surface of the tongue and lip ridges, difficult adaptation to dental prosthesis, changes in the palate (dysgeusia), and in the most severe cases, interference with chewing, swallowing, and speech. 4,12 -15 Xerostomia is reported in 100% of patients undergoing RT in the head and neck region, being commonly reported after the first week and becoming more severe along the weeks, peaking in the sixth week. 4,12 -16
Dysphagia is a swallowing disorder in which, in addition to causing discomfort, can trigger malnutrition and dehydration. Almost 60% of patients who receive RT develop some degree of dysphagia, where 20% of patients develop severe dysphagia (grades 3 and 4). 4,7,10 These severe grades can be also related to the large extension of the tumor and to severe pain. In fact, patients in this condition can only ingest liquid food or cannot have oral intake at all, thus compromising their nutritional intake and causing weight loss consequently. When patients cannot eat orally, nasoenteral feeding tubes or gastrointestinal tubes are used. 4,10,12,13,17
Dysgeusia is the distortion or diminution of the sense of taste, which occurs due to injuries to the oral epithelium, taste buds, and nerves caused by RT or chemotherapy. It is estimated that 50% to 75% of patients may develop dysgeusia, which is usually reported at the beginning of the RT. 4,12,13 The severity of dysgeusia can affect appetite by reducing the caloric intake, thus inducing weight loss and affecting the patient’s nutritional status. 4,12,13,17
The objective of this study was to analyze and prospectively assess the frequency and evolution of acute oral complications during radiochemotherapy in patients diagnosed with squamous cell carcinoma in the head and neck region.
Patients and Methods
All procedures performed in this study involving participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved according to protocol number 910.924 (CAAE 37922114.9.0000.0065) by the Research Ethics Committee of the School of Medicine, University of São Paulo. Informed written consent forms were signed by all the participants of this study.
In the present study, we have analyzed the oral complications of 20 patients who were treated at the Dental Oncology Service of the São Paulo State Cancer Institute (ICESP-FMUSP). The patients were evaluated weekly during radiochemotherapy treatment for squamous cell carcinoma in the head and neck region. Oral mucositis was evaluated according to World Health Organization criteria, 18 whereas dysphagia and dysgeusia were evaluated according to the National Cancer Institute Common Toxicity Criteria, 19 and xerostomia was evaluated according to parameters set by the Seminars in Radiation Oncology, 20 as listed in Table 1.
Classification of Acute Oral Complications.
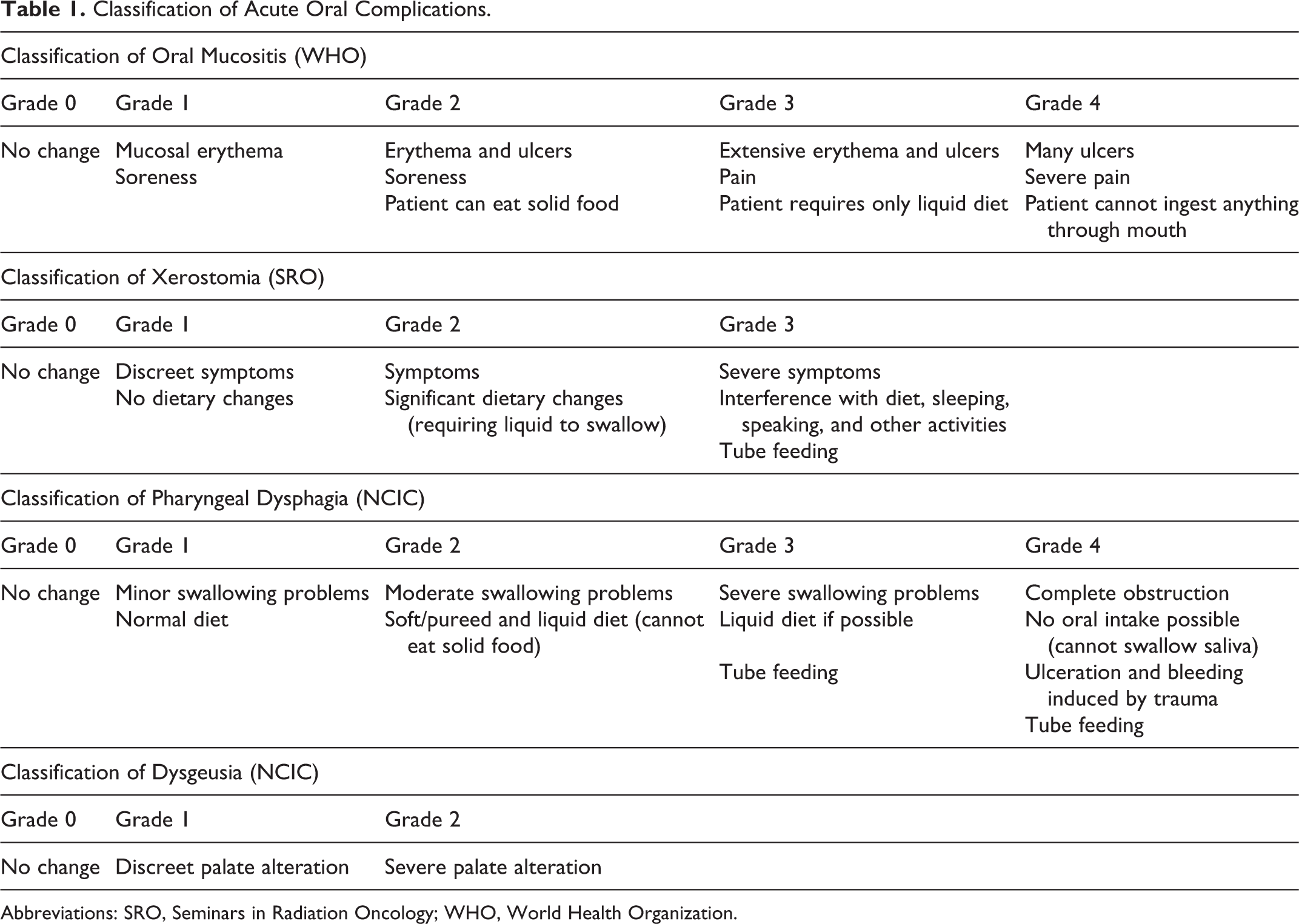
Abbreviations: SRO, Seminars in Radiation Oncology; WHO, World Health Organization.
All patients met the following eligibility criteria of the present study: diagnosis of head and neck squamous cell carcinoma, with visible tumors in the oral cavity. Treatment protocol using 3-dimensional RT. The total radiation dose was 60 Gy (fractionated into 30 fractions of 2 Gy/daily). Sessions occurred daily, for 5 consecutive days (Monday to Friday, with pauses on the weekends, for approximately 6 weeks). Association treatment with chemotherapy with cisplatin 100 mg/m2 (3 cycles every 21 days on days 1, 22, and 43) starting on the first day of RT. Dental treatment prior to RT, to control oral infections (tooth extractions, root scaling, and dental restoration); orientation on oral hygiene (ie, use of tooth brushing and dental floss, when possible, and oral rinsing with chlorhexidine 2%). Use of low-laser therapy protocol, to prevent and treat oral mucositis, according to the protocol established by the Dental Oncology Service of ICESP, for all patients undergoing RT against head and neck squamous cell carcinoma, with visible tumors in the oral cavity.
The low-laser therapy protocol establishes that all patients have received daily prophylactic doses, beginning on the first day of RT and after each session of RT. This consists in sessions of low-level laser applications at 10 W and 10 J (Laser DMC Twin, São Carlos, Brazil) to different sites (per point) of the oral cavity for 10 seconds: right and left sides of the tongue, upper and lower lips, soft palate (right and left), mouth floor (right and left), and ventral tongue. From the moment the first ulcer was observed, the patients were given curative laser therapy at low level (ie, 40 W, 60 J) for 1 minute per ulcer. Oral hygiene guidance was provided in combination with laser therapy, including use of artificial saliva and analgesic medication when required. 13,16
Medical history of patients was obtained from the medical records, namely age, gender, tumor location, and tumor-node-metastasis stage. The clinical evaluation of oral mucositis, pharyngeal dysphagia, xerostomia, and dysgeusia was performed by the same dentist on a weekly basis after RT session (during the 6 weeks of treatment).
The data were presented in absolute and relative frequencies. To compare the degree frequencies of mucositis, xerostomia, dysphagia, and dysgeusia, we used the Friedman’s test considering the weeks of RT. Statistical analyses were performed by using SPSS version 17.0 software (SPSS, Inc, Chicago, Illinois) at a significance level set at 5% (P < .05).
Results
Initially, we evaluated 50 patients undergoing the proposed treatment of radio/chemotherapy for squamous cell carcinoma in the head and neck region, with no previous surgery. Thirty patients were excluded from this cohort study either of personal reasons (9 decline participation and 3 moved to another city) or medical reasons (5 had changes in RT protocol before starting the treatment sessions, 4 had changes in RT protocol during treatment due to toxicity, 4 had RT suspended due to hospitalization in intensive care unit [ICU], and 5 died).
Twenty patients fully completed the RT treatment, with a total dose of 60 Gy. They met the eligible criteria of our study and had complications evaluated weekly during their RT treatment (ie, 6 weeks).
The general characteristics and medical history of these patients were presented in Table 2. All these characteristics were also described in a previously published work of our group. 13,16
Patients Characteristics.
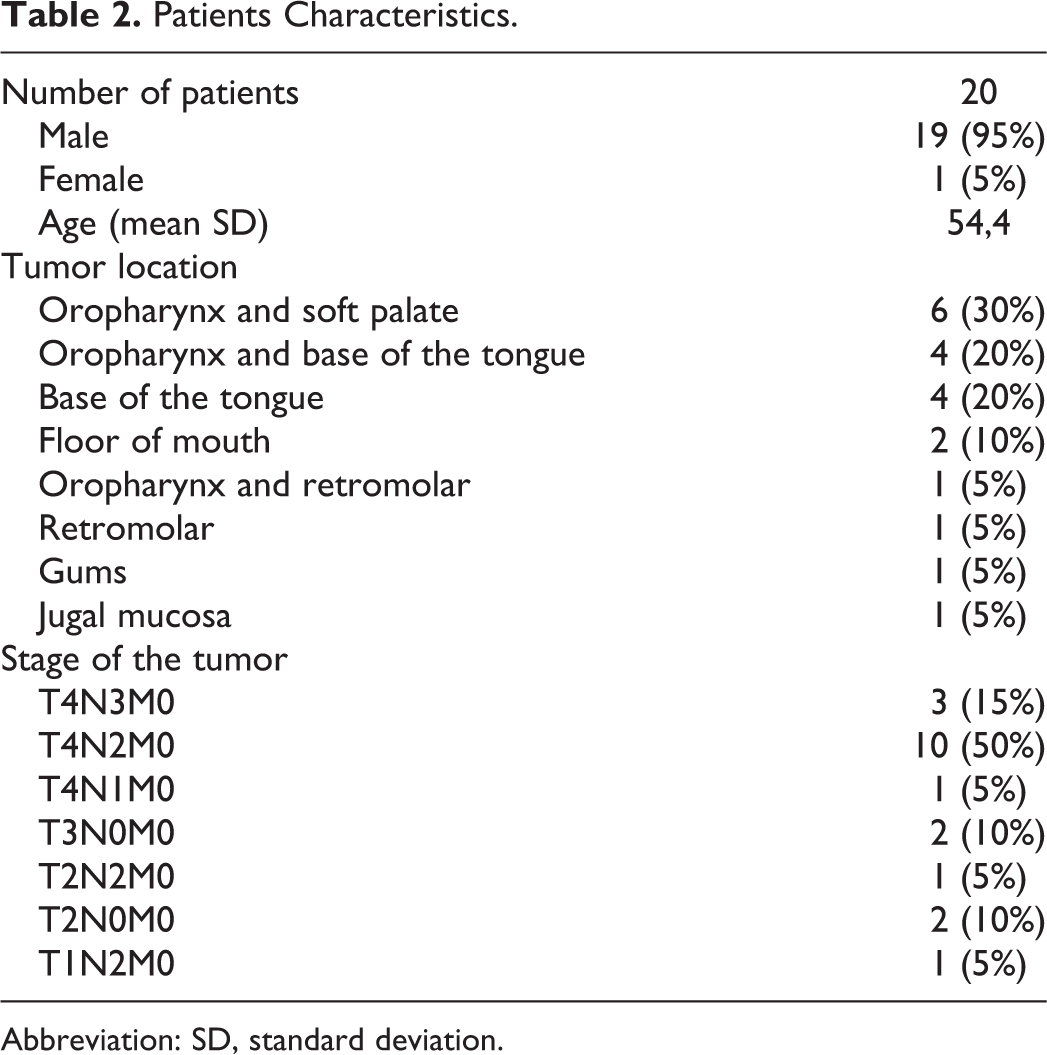
Abbreviation: SD, standard deviation.
Oral Mucositis
The clinical presentation of mucositis was first observed in the second week of RT, where 30% of the patients presented some alterations, being 2 of 20 with grade 1 and 4 of 20 with grade 2 (Figure 1). The number of patients with mucositis increased along the RT treatment and in the fourth week, all patients (20/20) presented some degree of mucositis. In this week, the first cases of more severe mucositis (grade 3) were also observed in 10% (2/20) of the patients. The sixth week was highlighted by the high number of more serious cases of mucositis, with 35% (7/20) being classified as grade 3 or 4. The lesions of oral mucositis worsened along the weeks of RT, that is, there was a transition from the second to the third week in which the highest number of changes was observed, but the sixth week had the most severe cases (Table 3).
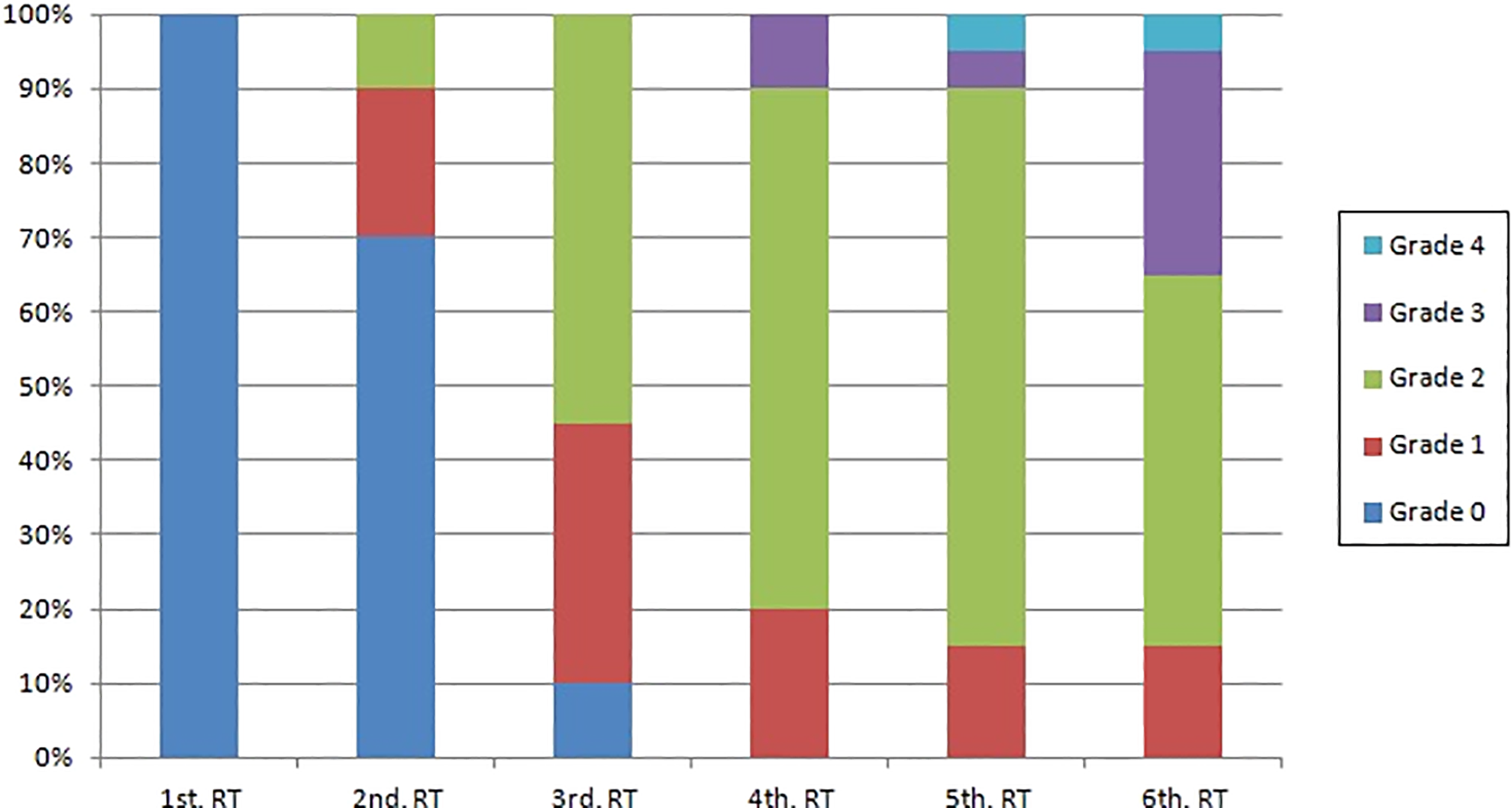
Degrees of mucositis (WHO) and weeks of RT (Friedman test, P < .001). RT indicates radiotherapy; WHO, World Health Organization.
Evaluation of the Degrees of Oral Mucositis During the 6 Weeks of RT.
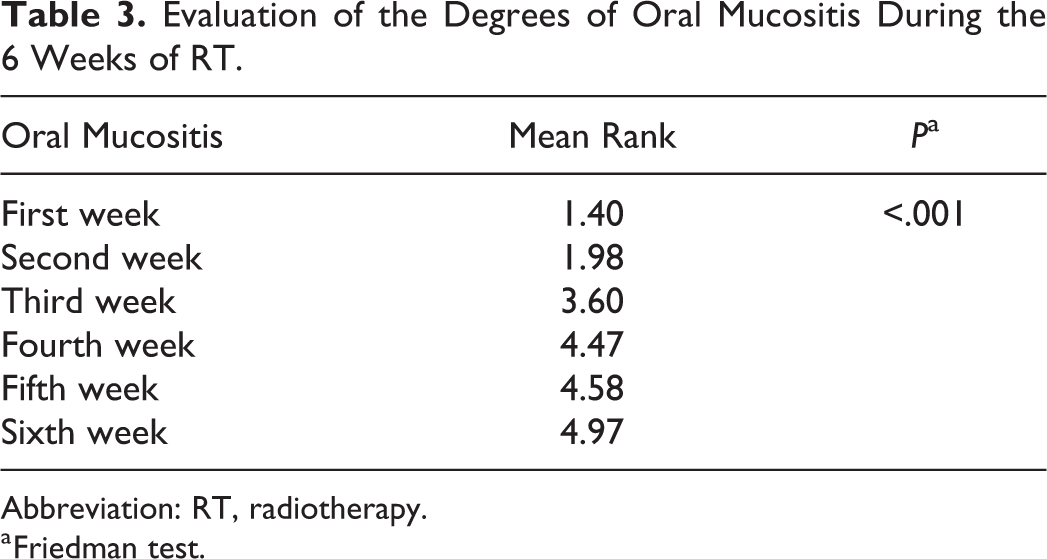
Abbreviation: RT, radiotherapy.
a Friedman test.
Xerostomia
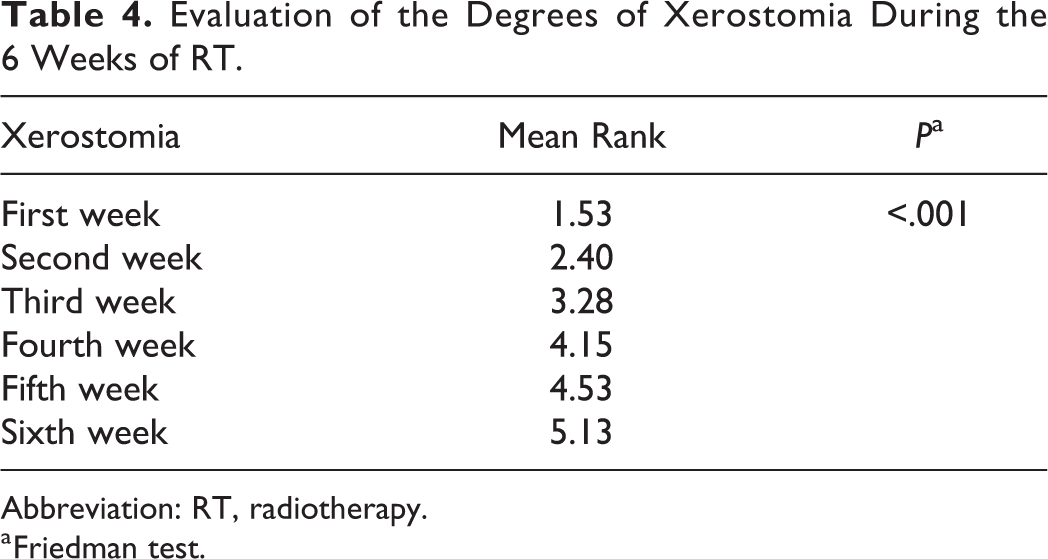
Fifteen percent (3/20) of the patients presented with xerostomia in the first week of RT. In the fourth week of RT, all patients (20/20) had some degree of xerostomia (Figure 2). The first patient with grade 3 xerostomia was observed in the fifth week. The sixth week was similar to that of patients with oral mucositis, being highlighted by the high number of xerostomia grade 3 in 20% (4/20) of patients. The patients progressed negatively along the weeks of RT, with the transition from the second to the third week presenting the highest number of changes and the sixth week having the most severe cases (Table 4).
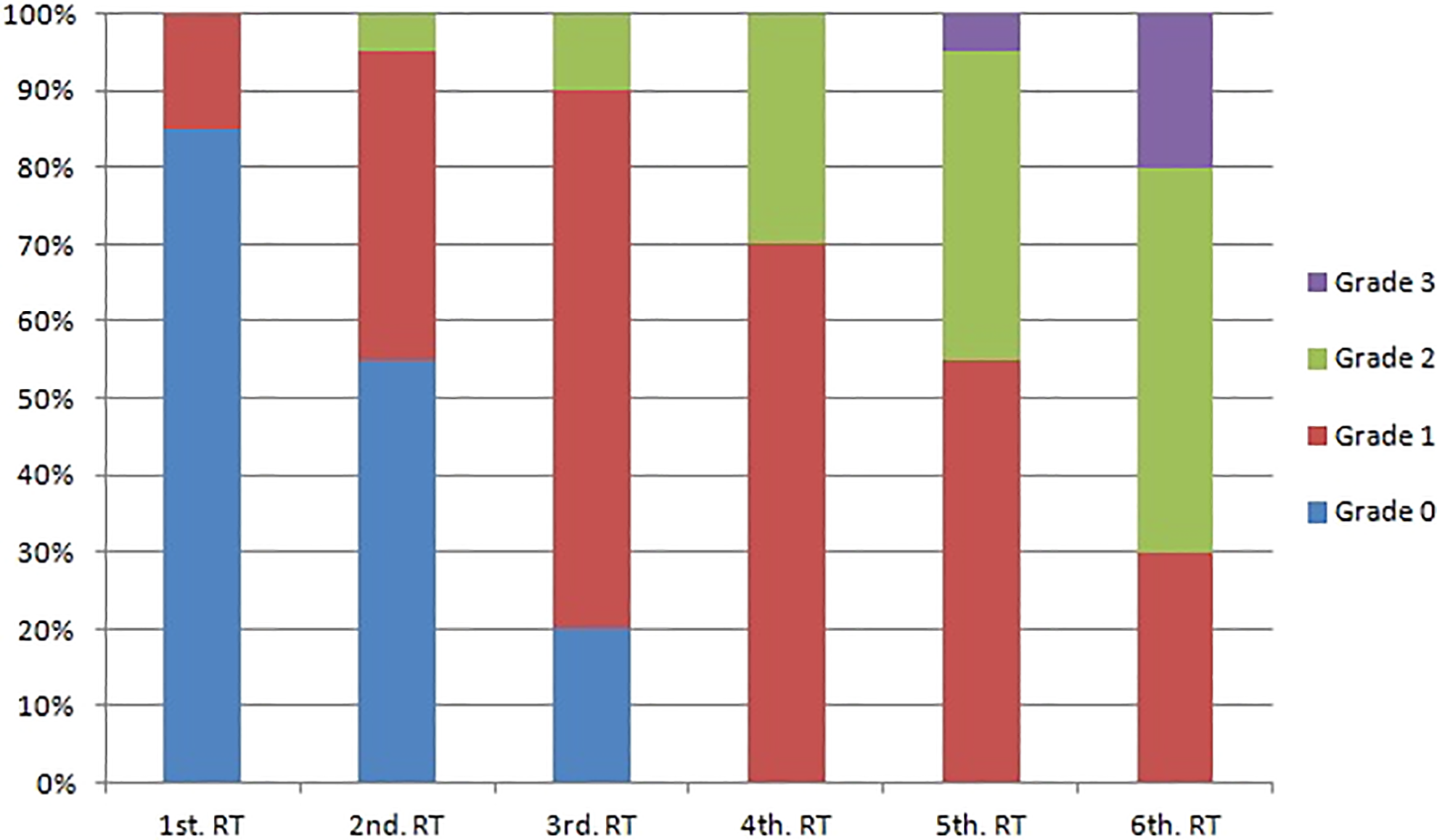
Degrees of xerostomia (SRO) and weeks of RT (Friedman test, P < .001). RT indicates radiotherapy; SRO, seminars in radiation Oncology.
Evaluation of the Degrees of Xerostomia During the 6 Weeks of RT.
Abbreviation: RT, radiotherapy.
a Friedman test.
Dysphagia
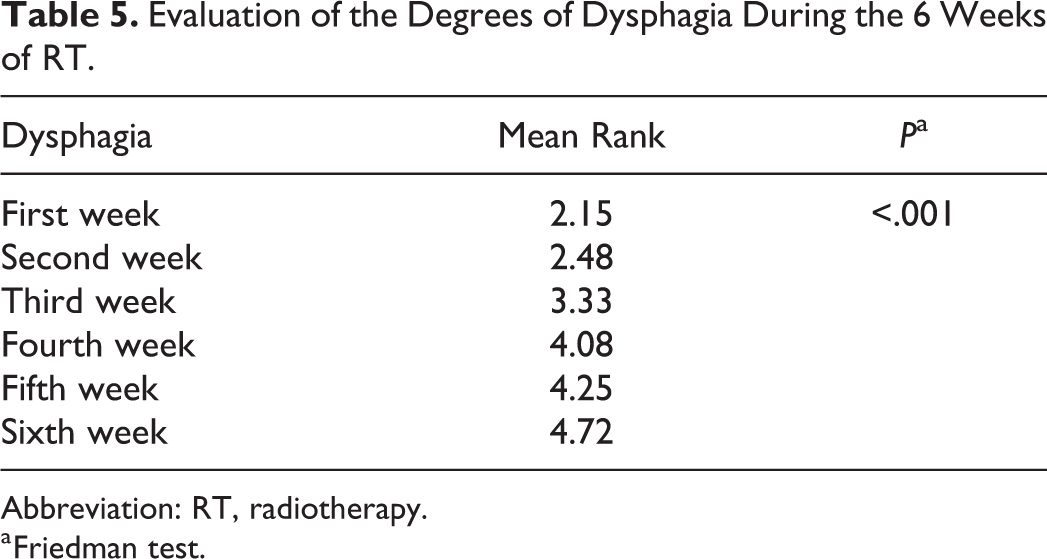
Fifty percent (10/20) of the patients reported dysphagia in the first week of RT, with 25% being grade 1 and 25% grade 3 (Figure 3). It was only in the sixth week that all patients (20/20) presented some degree of dysphagia, including the only case of more severe dysphagia (grade 4). Dysphagia was more common and increased in severity, with the transition from the second to the third week presenting the highest number of alterations and the sixth week having the most severe cases (Table 5).
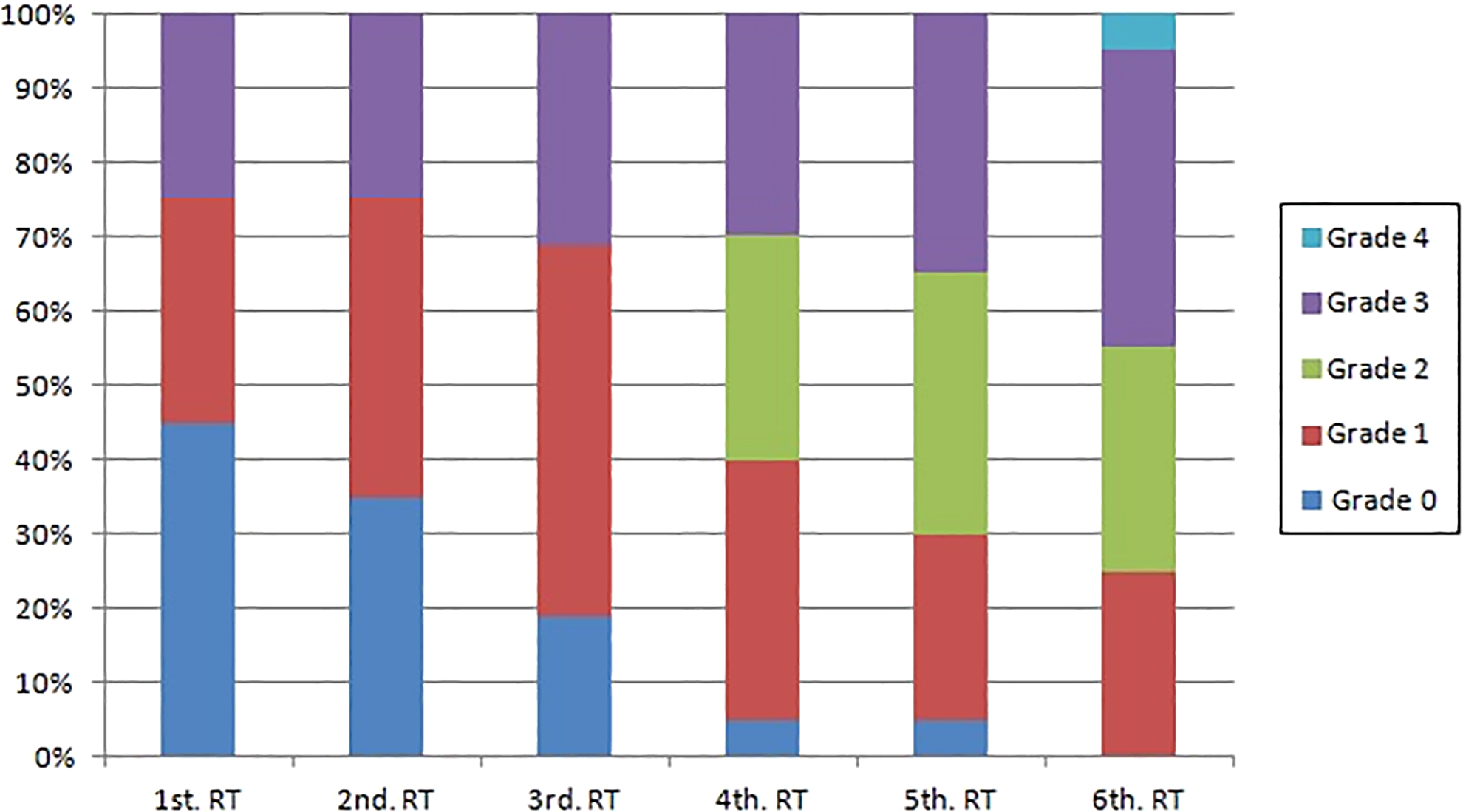
Degrees of dysphagia (NCIC) and weeks of RT (Friedman test, P < .001). RT indicates radiotherapy.
Evaluation of the Degrees of Dysphagia During the 6 Weeks of RT.
Abbreviation: RT, radiotherapy.
a Friedman test.
Dysgeusia
Dysgeusia was first observed in the second week of RT, where 40% of the cases being grade 1 (Figure 4). From the third week on, severe degree (grade 2) of dysgeusia was observed. In the fifth week, all patients who could be evaluated (13/13) reported some degree of dysgeusia and the highest number of severe cases was also observed in this period. The cases of dysgeusia worsened along the weeks as the transition from the first to the second week showed the highest number of alterations and the transition from the third to the fourth week showed a considerable worsening (Table 6). It is important to note that this variable involved loss of data during the weeks due to the fact that many patients had to receive tube feeding and did not receive oral diet during the RT treatment.
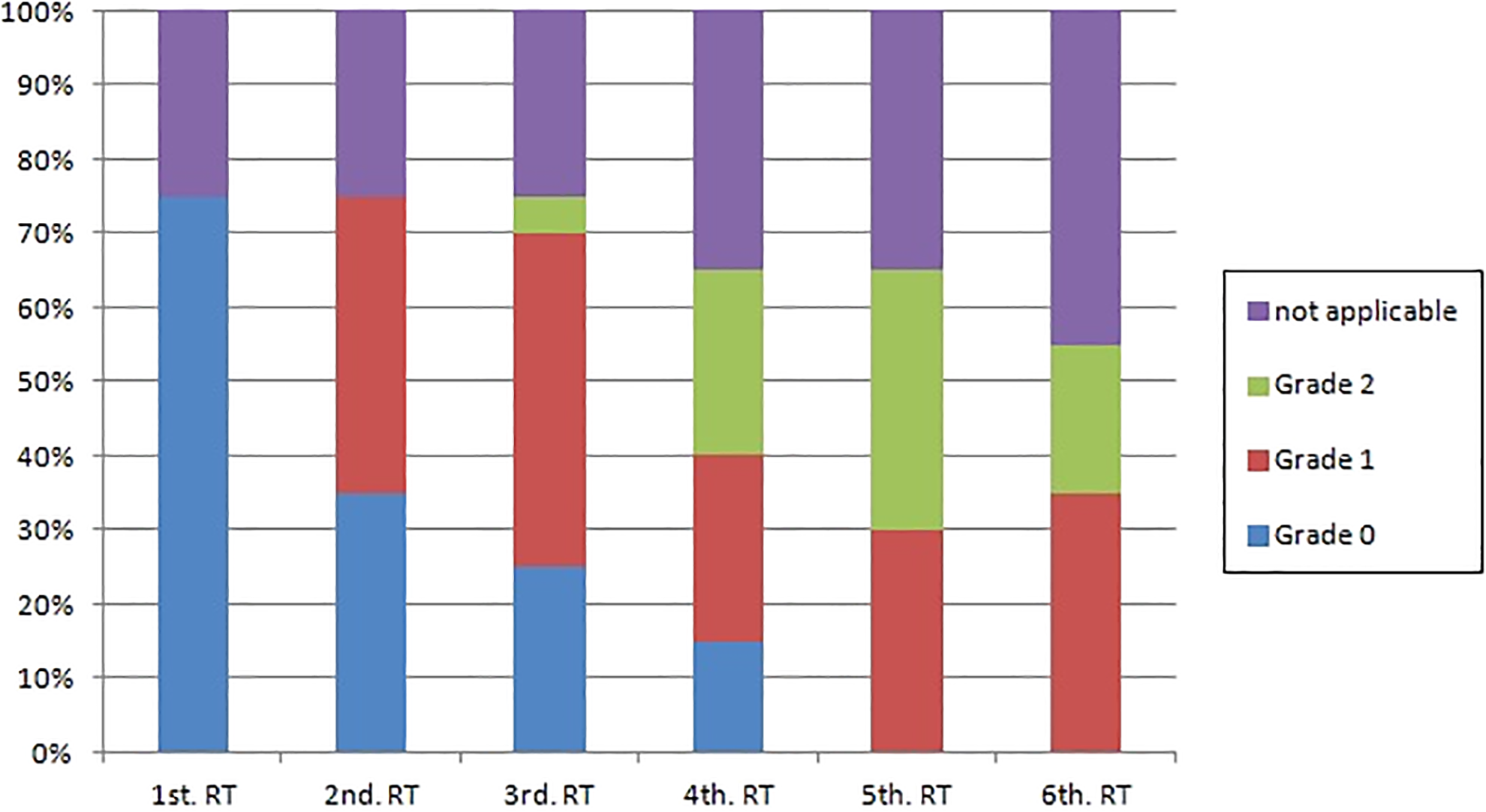
Degrees of dysgeusia (NCIC) and weeks of RT (Friedman test, P < .001). RT indicates radiotherapy.
Evaluation of the Degrees of Dysgeusia During the 6 Weeks of RT.
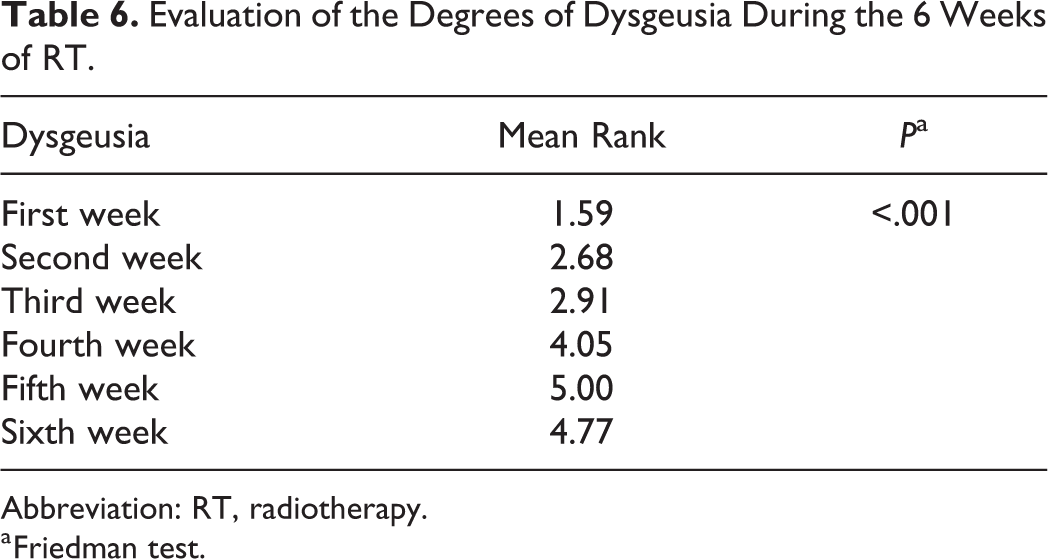
Abbreviation: RT, radiotherapy.
a Friedman test.
In general, it was observed that the third week of RT seemed to represent a critical week for the patients, since a higher number of alterations were observed in the transition from the second to the third week, regardless of the grade of the lesion. The sixth week, however, presented the worst grades of cases.
Discussion
Radiotherapy is one of the mostly used treatments worldwide for squamous cell carcinoma of the head and neck region because of its efficiency but is associated with oral complications which are well described in the literature, such as mucositis, xerostomia, dysphagia, and dysgeusia. 1 -4,13,17
In a systematic review by Trotti et al (2003), it was found that the highest prevalence of mucositis (43%) occurred in patients treated with RT associated with chemotherapy compared to patients treated with either RT (34%) or chemotherapy (22%). 10 Different authors report that mucositis is usually first seen in the second week of RT. 4,10,13 -15 Similar results were observed in our study, as 30% of the patients presented radiochemotherapy mucositis, in the second week of RT, 2 of 20 with grade 1 and 4 of 20 with grade 2 mucositis. An increase in its severity along the weeks of RT has also been described in the literature. In fact, the most severe degrees of mucositis (grades 3 and 4) are observed in the last weeks of treatment, which may lead to discontinuation of treatment or even hospitalization. 4,9,10,13,15,21 These data were also observed in our study as the first cases of grade 3 mucositis (10%; 2/20) were observed in the fourth week and one-third of patients (35%; 7/20) developed grades 3 and 4 mucositis in the sixth week.
Oral mucositis severity may be reduced with dental treatment and information prior to RT, which includes orientations on oral hygiene (to reduce oral infections by opportunistic pathogens that can exacerbate mucositis) and also monitoring throughout the treatment with low-level laser applications on a daily basis. 4,8,9,12 -14,22 -26 Despite the severe degrees of mucositis observed in our study, there was no discontinuation of radio/chemotherapy in our group of patients as a result of its severity. The control of mucositis within acceptable degrees was possible due to the pre-RT dental treatment and daily applications of low-intensity laser during the weeks of RT, for all patients undergoing RT against head and neck squamous cell carcinoma, with visible tumors in the oral cavity, thus showing the effectiveness of the protocol proposed by the ICESP. 13,20
Xerostomia is an oral complication with a different evolution, depending on the irradiated field. This complication can be described as transient, when the symptoms decrease or disappear after a few weeks from the end of RT, or permanent, when a possible permanent damage to the parenchyma of the salivary glands occurs. 4,12,13,15 There is a consensus that changes in the salivary flow rate will happen when salivary glands receive more than 50 Gy of radiation, and below that, changes can be transitory and limited.15,16 The first stages of xerostomia are usually observed in the first weeks of RT. 4,10,13,16,21,23,24 In our group, 3 of 20 patients presented xerostomia in the first week and 9 of 20 in the second week of RT. A worsening of xerostomia occurred throughout the weeks of RT, with all patients (20/20) presenting some degree of xerostomia in the fourth week of RT as they had a reduction in their salivary flow rate. In the sixth week, however, there were a high number of more severe cases of xerostomia in which 4 of 20 were classified as grade 3. In addition, the number of changes was the highest in the transition from the second to the third week.
The majority of patients undergoing RT in the head and neck region present some degree of dysphagia. In the fourth week of RT, most of patients developed severe grades of dysphagia (grade ≥ 2) and they may only eat liquid food and may require tube feeding. 4,10,13,16,17,25 Similar findings were also observed in our study, where 50% of patients reported dysphagia in the first week of RT (25% with grade 1 and 25% with grade 3). Studies report that the severity of dysphagia may be associated with the cumulative dose of radiation, 12,17,26 -28 a finding corroborated by our study as this acute complication was more common and more severe along the weeks of RT. Nevertheless, it was only in the sixth week that all the patients (20/20) presented some degree of dysphagia, including 1 case of grade 4 dysphagia. It was also observed that the transition from the second to the third week had the highest number of alterations, with an increase in dysphagia severity.
Dysgeusia is another oral complication well reported in the literature, occurring due to damage to oral epithelium or taste buds as a result of RT or chemotherapy. Dysgeusia is normally first reported by patients in the second week of RT, in parallel with the onset of mucositis. 4,12,13,17 This study has shown results similar to those reported in the literature, with dysgeusia being first observed in the second week of RT where 40% of the patients developed grade 1 dysgeusia. Similar to dysphagia, the severity of dysgeusia can be associated with the cumulative dose of radiation (2 Gy/daily, with total dose of 30 Gy or higher). 12,26 In our study, severe degrees of dysgeusia (grade 2) were observed from the third week on, and in the fifth week, all the patients who could be evaluated (13/13) reported some degree of dysgeusia. It was also observed that there was a high number of severe cases in the fifth week. It is important to remember that in our study, some patients could not be evaluated for dysgeusia (thus causing a loss of data along the weeks) as they were on tube feeding and received no oral diet. Nevertheless, worsening of dysgeusia along the weeks of RT was observed in the transition from the first to the second week as there were a higher number of taste alterations, but the transition from the third to the fourth week showed a considerable worsening as well.
The severity of the oral complications may be influenced by the dose, field, and mode of radiation delivery. Symptoms consistently and significantly improved after the final week of RT. The majority of complications return to baseline levels after 12 weeks posttreatment, excepting xerostomia. Mucositis and dysphagia had significant decrease in symptoms by 4 to 6 weeks posttreatment, while dysgeusia had its significant decrease in symptoms after 4 weeks. This information can be helpful to inform the timing of clinical service planning. 29
One of the limitations of this study is the number of patients excludes due to medical reasons. Five patients had changes in RT protocol before starting the RT sessions, because they were first submitted to surgery, and the possibility of RT would be evaluated after that. Four patients had changes in RT protocol during treatment due to clinical general conditions. Those patients were very debilitated, losing weight, and developing infections. Four patients had RT suspended due to hospitalization in ICU, for the same previous reasons, but in a much severe stage. Five patients died for different reasons such as stroke, advanced age, and large tumors that cause other severe complications. It is important to emphasize that all the exclusions that occurred during this study were not associated with acute oral complications.
Patients undergoing radiochemotherapy treatment are affected by acute oral complications that may lead to changes in the oral cavity affecting the patient’s quality of life. Understanding the natural course of acute oral complications is important by informing patients on the importance of maintaining an adequate oral health to help minimizing the symptoms of acute oral complications. Develop better strategies to treat these symptoms may help to improve quality of life in patients undergoing radiochemotherapy against head and neck cancer in the future.
Footnotes
Authors’ Note
This article was presented at the 14th Biennial Congress of the European Association of Oral Medicine (EAOM), in conjunction with the World Workshop on Oral Medicine VII, in Gothenburg, Sweden, in September 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Conselho Nacional de Desenvolvimento Tecnológico (CNPq grant no. 44004/2014-5) and Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP grant no. 2012/04303-5 and 2015/07727-9).