
Abstract

A 47-year-old man visited for the evaluation of a left nasal obstruction of 6 months duration. No trauma history or other underlying systemic disease was noted. Endoscopic examination revealed a nasal polyp arising from the ostiomeatal complex and extending into the nasopharynx. Paranasal sinus computed tomography (CT) showed total opacity of the left maxillary sinus and soft tissue density mass in the nasal cavity that passed through a widened maxillary sinus ostium and extended into the choana. The roof and floor of the maxillary sinus were intact, but a thin-rimmed, expansile calcification area within the maxillary antrum was demonstrated on CT images (Figure 1). Under suspicion of an antrochoanal polyp (ACP) of the left nasal cavity, endoscopic sinus surgery was performed. Intraoperatively, a solitary nasal polyp that originated in the maxillary antrum was identified, and a dark brown-colored, soft, friable materials were observed in the affected maxillary sinus after the cystic portion of the ACP had been ruptured. The lesion was extirpated completely using the transnasal endoscopic approach. Histopathological examination of surgical specimens of maxillary sinus revealed cholesterol clefts and a foreign body granuloma in edematous stroma, which were consistent with a finding of cholesterol granuloma (Figure 2). The pathological diagnosis was nasal polyp associated with cholesterol granuloma of the maxillary sinus. There was no evidence of recurrence at the 2-year follow-up.
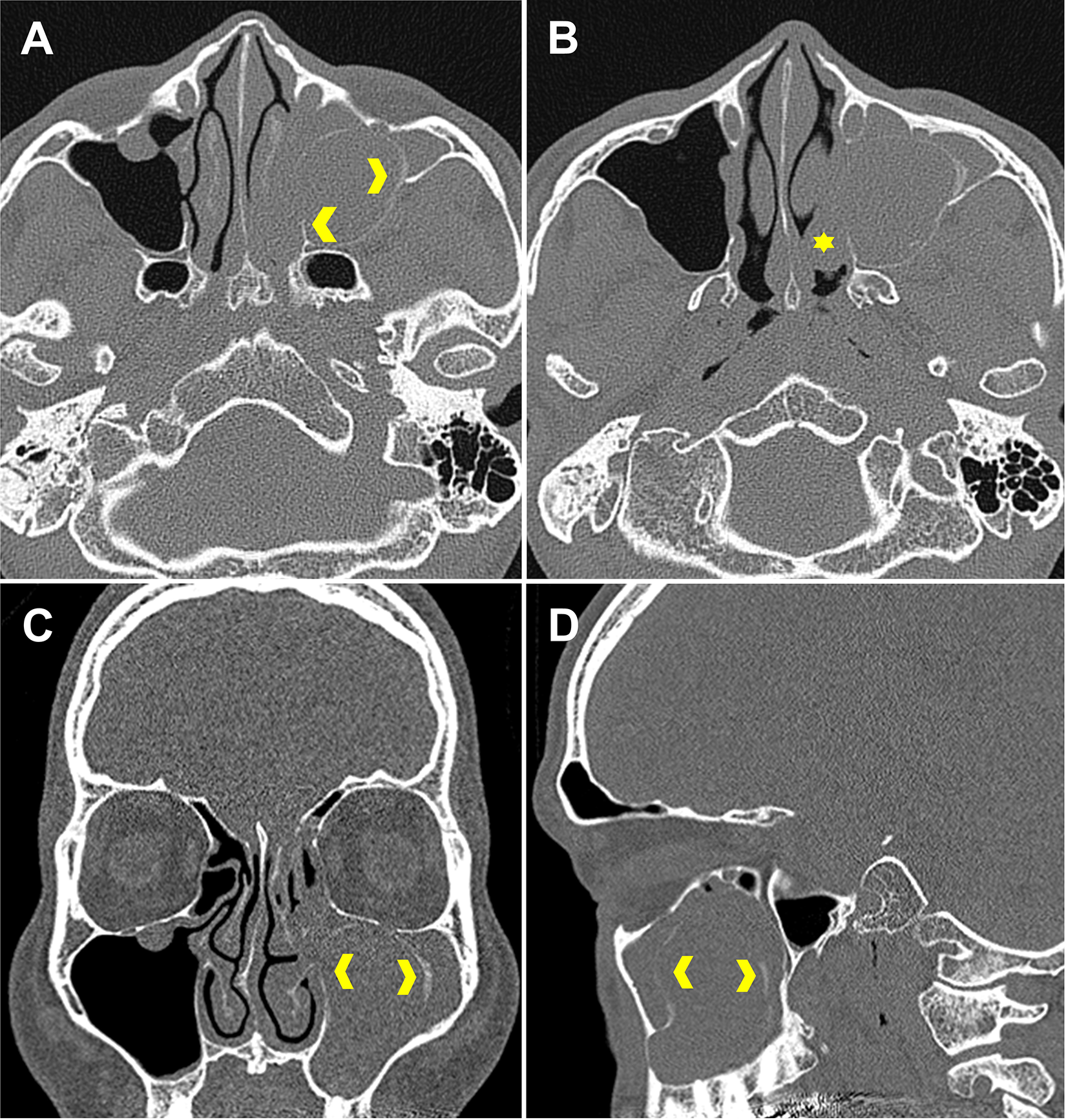
Computed tomography (CT) images. Axial view (A and B), coronal view (C), and sagittal view (D). Axial CT scans (A and B) show well-marginated, expansile, soft tissue density with rim calcification (yellow arrowhead) in the left maxillary sinus passing through a widened maxillary sinus ostium and extending into the choana (yellow asterisk). Coronal (C) and sagittal (D) CT scans showing total opacification of the left maxillary sinus and the rim calcification area (yellow arrowhead).
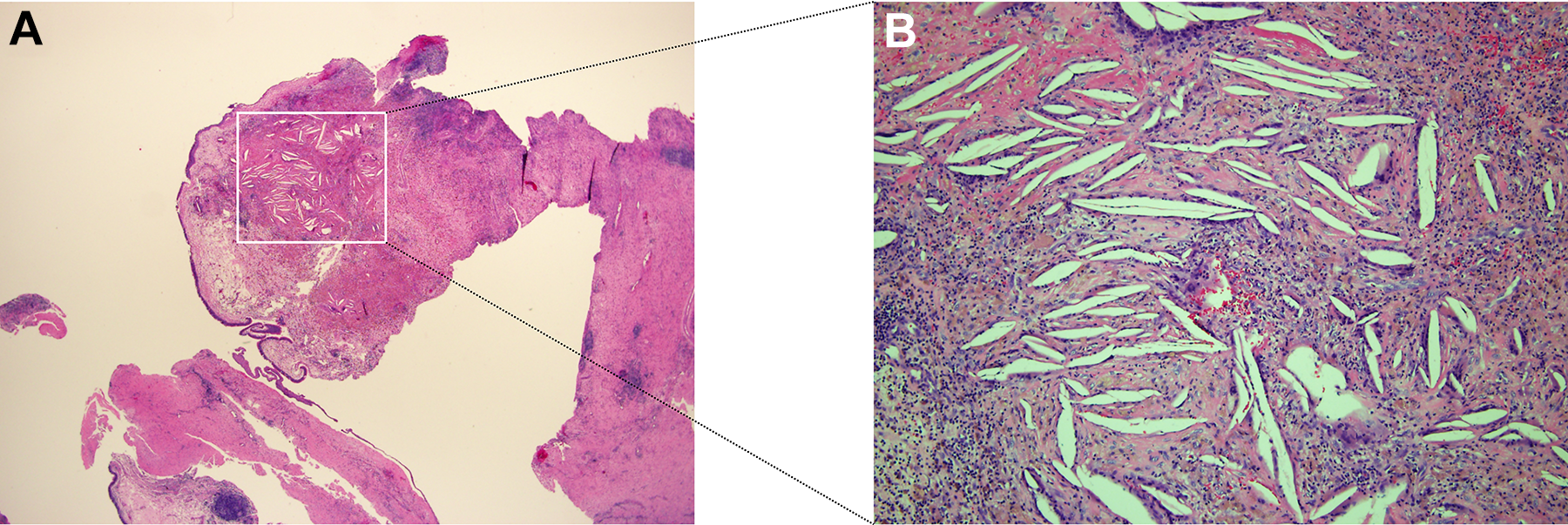
A, Photomicrograph of surgical specimen epithelium, showing invaginations and cystic cavitation formation. The stroma showed prominent edema with diffuse inflammatory infiltrate and lymphocyte aggregates (hematoxylin and eosin [H&E] stained, original magnification ×20). B, Cholesterol crystals, which appeared as clefts, were surrounded by multinucleated foreign body giant cells, small areas of hemorrhage, and chronic inflammatory infiltrate (H&E stained, ×100).
Cholesterol granuloma is a granulomatous reaction to cholesterol crystals precipitated in tissues and is commonly found in the airspace of temporal bone. 1 Since cholesterol granuloma is rarely found in the sinonasal region, little is known of its etiology or clinical manifestations. 2 To the best of our knowledge, only 6 cases of cholesterol granuloma associated with ACP have been described in the English literature. 3,4
Antrochoanal polyp is known to occur in inflamed, edematous mucosa of the maxillary sinus or an accessory ostium. 5 Several possible mechanisms, that is, drainage impairment, disturbed ventilation, and hemorrhage, have been proposed to explain the pathogenesis of cholesterol granuloma and the accumulation of cholesterol crystals in the sinonasal region. 6,7 In our patient, the ACP may have interfered with air exchange within the maxillary sinus and promoted cholesterol granuloma formation. More specifically, the negative pressure and hypoxic condition caused by the ACP may have induced a vicious cycle of transudate and blood extravasation, accumulations of hemosiderin and especially cholesterol crystals, and foreign body granuloma formation. Opening the closed space, evacuating contents, and aerating the cavity probably arrest this process, 2,8 and thus, the treatment and outcomes of an ACP associated with cholesterol granuloma are the same as for usual ACPs. Magnetic resonance imaging has led to substantial advances in the preoperative differential diagnosis of cholesterol granuloma. 1 On CT images, the typical radiologic feature of cholesterol granuloma is a well-circumscribed expansile lesion with soft tissue density, which makes it difficult to differentiate from nasal polyp or mucocele. 9 Interestingly, in our case, CT also depicted a calcified area in the opacified maxillary sinus region, which was previously described by Ko et al, who suggested that repeated foreign body reaction causes calcification that might be visualized on CT images as an opacified lesion with calcification. 8 Although a final diagnosis of cholesterol granuloma in a sinonasal lesion is difficult to make before examination of a surgical specimen, we suggest cholesterol granuloma be included in the differential diagnosis in patients showing characteristic unilateral opacification with intralesional calcification on CT images.
We describe a unique case of ACP associated with cholesterol granuloma of the maxillary sinus. It seems possible that the shared clinical manifestations of ACP and cholesterol granuloma reflect a causative relationship. We hope this report improves clinical knowledge of cholesterol granuloma in a sinonasal lesion and increases the likelihood of early diagnosis and treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.