
Abstract
A previously healthy 11-month-old female was hospitalized for a barking cough and difficulty breathing. Her mother did not witness the triggering event at home but heard the child begin coughing while she was playing out of sight. She improved with corticosteroids and nebulized racemic epinephrine and was diagnosed with croup. She was discharged the following day without incident. The patient was readmitted to the hospital 10 days later with return of the barking cough and new dysphonia. Soft tissue neck X-ray demonstrated moderate subglottic narrowing with no foreign body seen. Her symptoms once again improved with clindamycin, ceftriaxone, and corticosteroids. Several days later, she was discharged home on antibiotics and a corticosteroid taper.
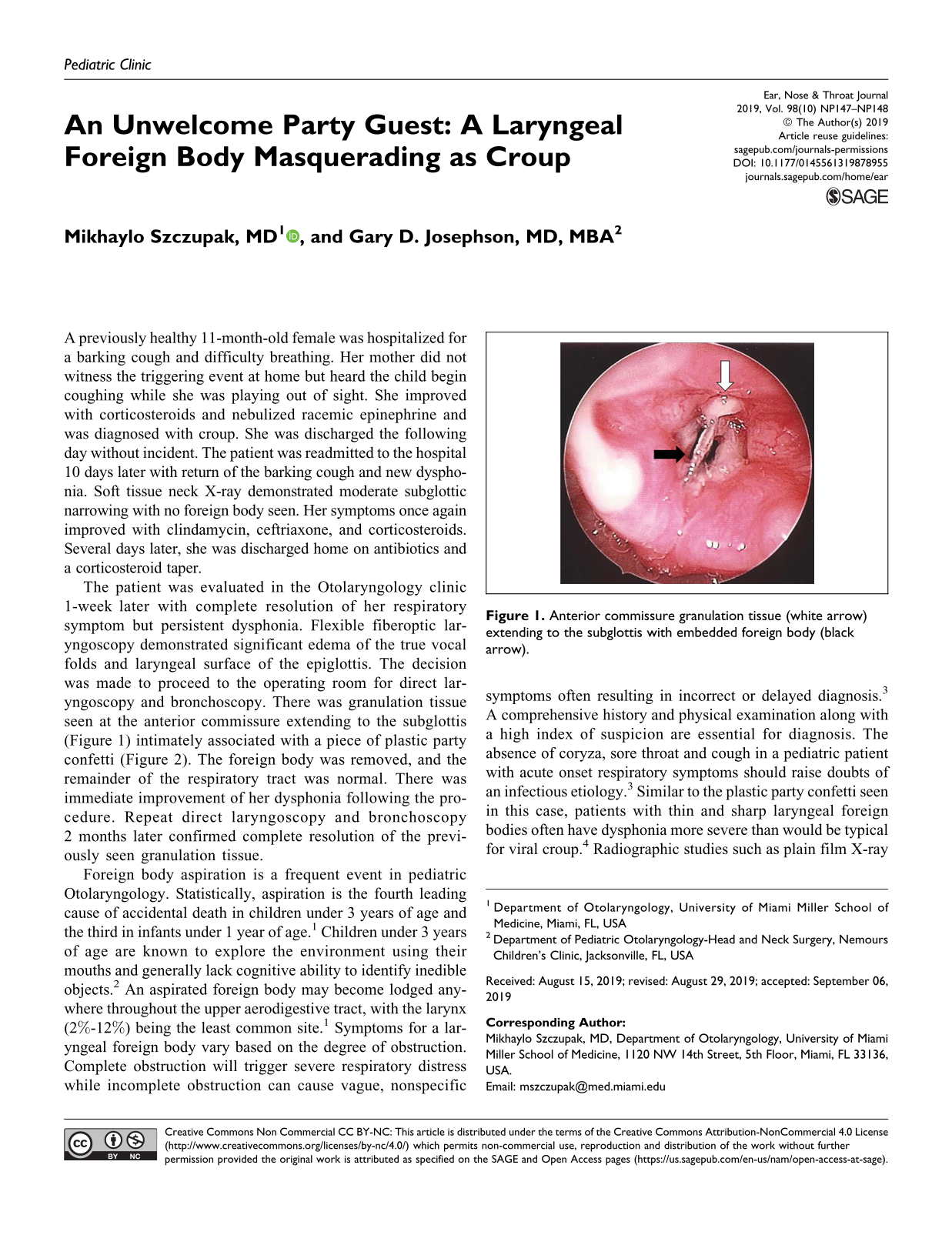
The patient was evaluated in the Otolaryngology clinic 1-week later with complete resolution of her respiratory symptom but persistent dysphonia. Flexible fiberoptic laryngoscopy demonstrated significant edema of the true vocal folds and laryngeal surface of the epiglottis. The decision was made to proceed to the operating room for direct laryngoscopy and bronchoscopy. There was granulation tissue seen at the anterior commissure extending to the subglottis (Figure 1) intimately associated with a piece of plastic party confetti (Figure 2). The foreign body was removed, and the remainder of the respiratory tract was normal. There was immediate improvement of her dysphonia following the procedure. Repeat direct laryngoscopy and bronchoscopy 2 months later confirmed complete resolution of the previously seen granulation tissue.

Anterior commissure granulation tissue (white arrow) extending to the subglottis with embedded foreign body (black arrow).

Plastic party confetti foreign body following removal.
Foreign body aspiration is a frequent event in pediatric Otolaryngology. Statistically, aspiration is the fourth leading cause of accidental death in children under 3 years of age and the third in infants under 1 year of age. 1 Children under 3 years of age are known to explore the environment using their mouths and generally lack cognitive ability to identify inedible objects. 2 An aspirated foreign body may become lodged anywhere throughout the upper aerodigestive tract, with the larynx (2%-12%) being the least common site. 1 Symptoms for a laryngeal foreign body vary based on the degree of obstruction. Complete obstruction will trigger severe respiratory distress while incomplete obstruction can cause vague, nonspecific symptoms often resulting in incorrect or delayed diagnosis. 3 A comprehensive history and physical examination along with a high index of suspicion are essential for diagnosis. The absence of coryza, sore throat and cough in a pediatric patient with acute onset respiratory symptoms should raise doubts of an infectious etiology. 3 Similar to the plastic party confetti seen in this case, patients with thin and sharp laryngeal foreign bodies often have dysphonia more severe than would be typical for viral croup. 4 Radiographic studies such as plain film X-ray are typically performed but a negative result should not delay intervention. Approximately 80% of airway foreign bodies in children less than 3 years of age are food items or other radiolucent substances. 5 Flexible endoscopy of the airway should be performed if the history and physical examination are suggestive of an aspirated foreign body 6 and should not preclude a decision for direct laryngoscopy and rigid bronchoscopy under general anesthesia for definitive airway survey in selected cases where diagnosis remains in doubt. This case provides an excellent example for a laryngeal foreign body that was not visualized on flexible endoscopy but instead required direct laryngoscopy and bronchoscopy for both diagnosis and treatment.
Footnotes
Authors’ Note
This work has not been previously been presented at any scientific meetings.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.