
Abstract
Frontal sinus stenting is widely used with the goal of maintaining nasofrontal duct patency after sinus surgery. The general recommendation is to leave stents in place for 6 months; however, prolonged stenting up to 6 years has been reported with no complication. We present the first reported case of frontal sinus posterior table and skull base erosion following prolonged frontal sinus stenting. A 57-year-old female presented with chronic sinusitis and nasal obstruction. Imaging revealed pansinusitis with retained stents in each frontal sinus that were placed 8 years prior. On the right, there was an area of skull base erosion at the tip of the stent. The patient underwent functional endoscopic sinus surgery with polypectomy. The stents were removed, revealing posterior table erosion on the right side but intact mucosa. Two months after surgery, there were no signs or symptoms of cerebrospinal fluid leak or other complications. Recent literature has suggested that prolonged stenting is safe; however, this case highlights a complication with potentially serious outcomes that can result from prolonged stenting. We recommend stent removal once stable nasofrontal duct patency has been achieved. If prolonged stenting is utilized, patients should be closely monitored and consideration should be given to periodic imaging to evaluate stent position.
Introduction
The frontoethmoidal region’s increased susceptibility to granulation, osteoneogenesis, and stenosis provides unique challenges to maintaining patency after frontal sinus surgery. After functional endoscopic sinus surgery (FESS), there is a reported rate of recurrent frontal sinus disease and restenosis of the nasofrontal duct (NFD) up to 30%. 1 Frontal sinus stenting has been used to maintain the patency of the sinus and has been shown to prevent postoperative scarring in 80% to 94% of cases. 2 -4
Stenting may be indicated for an intraoperative NFD diameter of less than 5 mm, 5 as NFDs of that size demonstrate a stenosis rate of 33%. 6 Other indications include severe polyposis and aspirin intolerance, as these factors have shown an increased risk of constriction and stenosis. Osteitic bone in the frontal recess and excessive denuded bone at the neo-ostium are also indications.
The length of time for frontal sinus stenting is surgeon and patient dependent. Stenting for up to 6 years has been reported without complications, 7 although manufacturers generally recommend removal after 6 months. Current reported complications of frontal sinus stenting include formation of granulation tissue, stent dislocation, and complications of infection, including superinfection, biofilm formation, and toxic shock syndrome. 8 -11 There have, however, been no reported cases of skull base erosion due to frontal sinus stenting. We present a case of posterior table and skull base erosion caused by a frontal sinus stent left in situ for 8 years.
Case Report
A 57-year-old female presented with symptoms of chronic sinusitis and nasal obstruction. Eight years prior, the patient had FESS for chronic sinusitis by an outside physician, but she was lost to follow-up. Computed tomography (CT) of the sinuses revealed extensive pansinusitis with a retained stent in each frontal sinus. On the right, there was a 5 mm × 4 mm (height × width) erosion of the skull base at the distal tip of the frontal sinus stent (Figure 1). A preoperative CT scan from 8 years prior showed an intact skull base. Magnetic resonance imaging was obtained after CT in order to further assess for intracranial abnormalities, of which there were none (Figure 2). Neurosurgery consultation recommended removal of the stent with further observation for a cerebrospinal fluid (CSF) leak, although an intact dura mater on imaging made this less likely.

Preoperative CT scan in axial (A) and sagittal (B) views demonstrating stent placement with bony erosion of the posterior table and skull base. CT indicates computed tomography.
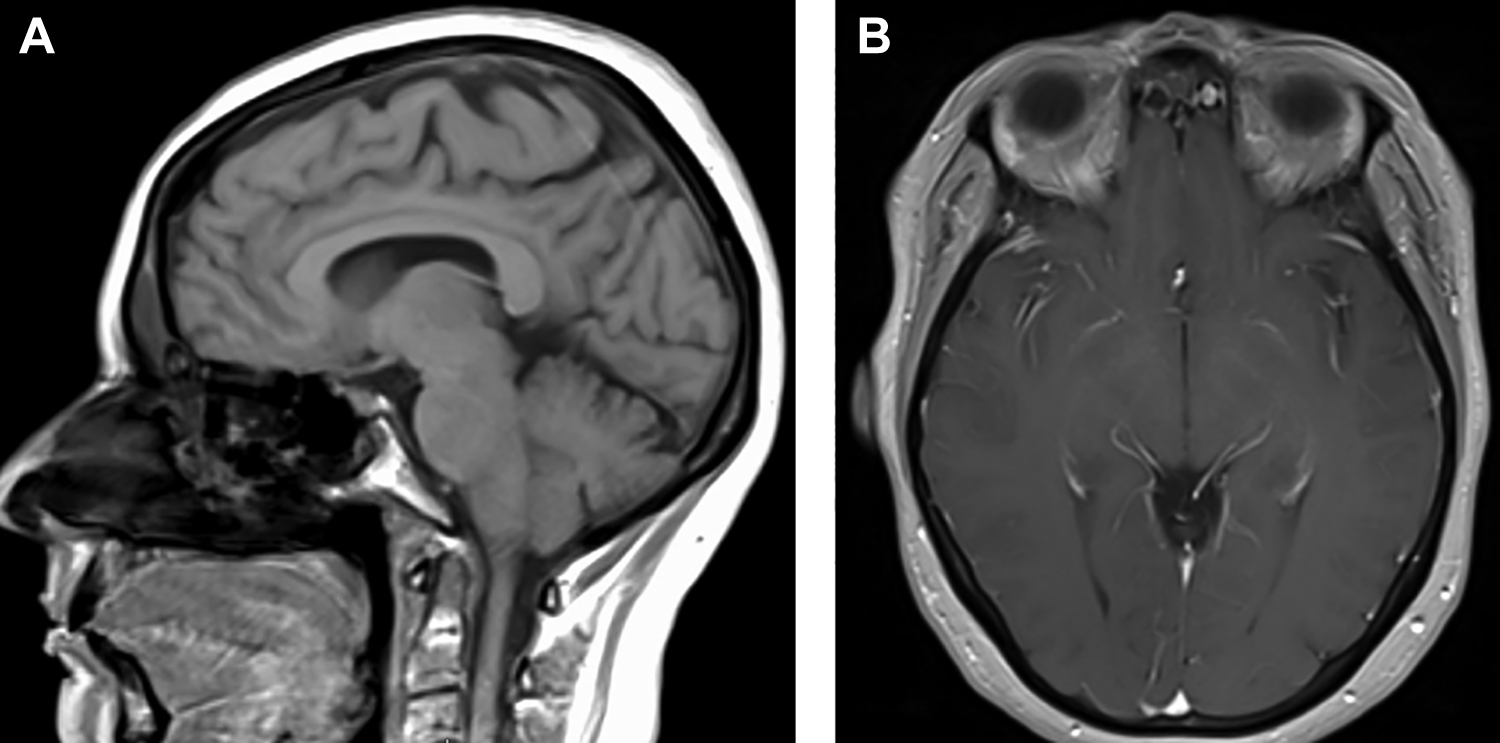
Preoperative T1 postgadolinium MRI in sagittal (A) and axial (B) views demonstrating right frontal sinus stent adjacent to dura. MRI indicates magnetic resonance imaging.
The patient was taken to the operating theater for removal. Polyps encasing the frontal sinus stent were cleared and the stent, a Rains Frontal Sinus Stent (Gyrus ACMI, Southborough, Massachusetts), was carefully extracted. Removal of the stent revealed clear posterior table erosion based on visible pulsations from the dura. The sinus mucosa appeared intact, and the duct was observed for several minutes with no sign of CSF leak (Figure 3). Due to the location of the skull base erosion and risk of intracranial extension of sinusitis, the patient was followed closely in the immediate postoperative period. Two months after surgery, there were no signs or symptoms of CSF leak or other complications.
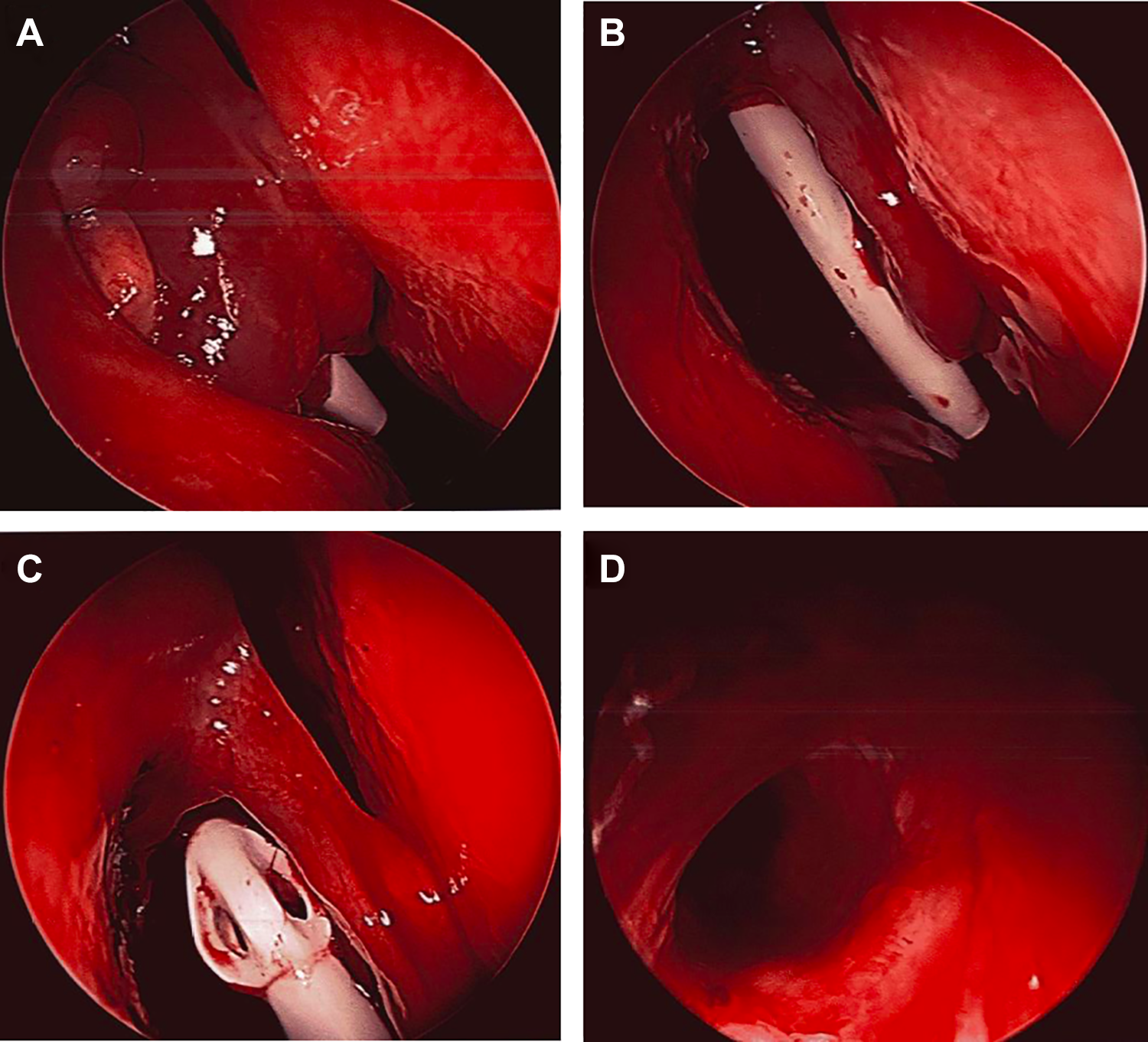
A, Intraoperative view demonstrating frontal sinus stent surrounded by polyps. B, Stent placement lateral to the middle turbinate after polyp removal. C and D, Stent removal (C) and view of the NFD and posterior table with mucosa intact (D). NFD indicates nasofrontal duct.
Discussion
Functional endoscopic sinus surgery is performed for chronic sinusitis to maintain patency throughout the paranasal sinuses via improved ventilation from widened sinus ostia. However, studies report a high rate of postoperative stenosis of the frontal sinus. Failure rates of 2% to 11% due to persistent frontal sinusitis with a revision rate of 1% to 5% have been reported by various studies. 3,6,12 -15 The frontal sinuses and associated NFD are predisposed to granulation tissue and scarring.
To combat the high rate of postoperative stenosis, frontal sinus stenting has been utilized since the early 1900s 5 as a method of maintaining patency without more extensive surgery, such as extended frontal sinusotomy procedures. Authors have proposed various indications for frontal sinus stenting. Stenting may be indicated for an intraoperative NFD diameter less than 5 mm, 5 as NFDs of that size demonstrate a stenosis rate of 33%. 6 Other indications include extensive polyposis, excessive denuded bone at the neo-ostium, and a floppy middle turbinate. 5 In a retrospective study by Orlandi and Knight, 7 2.2% of 462 patients who underwent frontal sinus exploration had stents placed in cases when mucosal preservation was sacrificed.
Timing for frontal sinus stent removal is surgeon and patient dependent, and authors have reported times varying from 1 week 5 up to 6 years without complications. 7 Multiple studies report success with long-term frontal sinus stenting over 3 months. A study by Weber et al 8 indicated improved outcomes and decreased rates of stenosis with stenting for at least 6 months. Orlandi and Knight 7 and Hunter et al 1 published series in which frontal stents were left in place as long as the NFD remained patent and patients remained asymptomatic. Rather than a strict time criterion, Rains recommended removal based on the clinical criteria of epithelialization of ethmoid sinuses, absence of drainage, and resolution of polypoid mucosa. 5
Orlandi and Knight 7 reported that 7 of 9 patients maintained successful frontal sinus stents for up to 6 years without stenosis and recurrence of symptoms. One patient required removal of their stent at 61 months due to infection that could not be controlled with culture-directed antimicrobials for 6 weeks. Endoscopy 8 weeks following stent removal revealed a patent frontal sinus outflow tract with mild edema. Another patient required removal at 11 months due to discomfort. The patient was followed for 10 months after stent removal and had a widely patent frontal sinus at last follow-up.
Hunter et al 1 reported 3 cases of successful long-term stenting that ranged from 48 to 60 months. Of these 3 cases, 1 patient experienced stent displacement after 29 months, and the stent was replaced and retained for another 19 months. Another patient experienced epistaxis immediately after surgery, and the stent was changed to a smaller size and left in place for over 60 months. Patients followed in the studies conducted by Orlandi and Knight, 7 Hunter et al, 1 and Weber et al 8 were followed regularly and received imaging as needed.
Frontal sinus stenting is widely utilized by otolaryngologists and is generally safe. Bony erosion of the posterior table of the frontal sinus and anterior skull base has not previously been reported as a complication of stenting. This complication carries with it the risk of subsequent CSF leak and other even more serious outcomes. It is unclear how long it takes for bony erosion to begin occurring and whether there are risk factors that make certain patients more susceptible. In this case, CT imaging revealed skull base erosion 8 years after insertion of a silicone Rains Frontal Sinus Stent (Gyrus ACMI). The literature has reported a range of other complications from frontal sinus stents, including granulation tissue, stent dislocation, and infectious complications such as superinfection, biofilm formation, and toxic shock syndrome. 8 -11 While recent literature has reported the perceived safety of prolonged stenting, 1,7 we recommend stent removal once stable NFD patency has been achieved in order to ensure serious complications do not occur. Patients who do have stents in place for prolonged periods should be closely monitored for complications and consideration should be given to periodic imaging to fully evaluate stent placement.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient to allow information and images to be published. Poster presented at the 2018 American Rhinologic Society Annual Meeting at COSM, National Harbor, MD, on April 20, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.