
Abstract
Purpose:
To assess the correlation between the comorbidities, such as hypertension, diabetes, thyroid disorders, hearing loss, hyperlipidemia, and vitamin D deficiency and benign paroxysmal positional vertigo (BPPV) and to determine the high-risk groups for recurrence of symptoms.
Design:
Descriptive analytical study.
Materials and Methods:
Patients who met the inclusion criteria underwent complete ear, nose, and throat examination, including Dix-Hallpike test and roll-over test and blood pressure recording. Investigations included pure tone audiometry, random blood sugar/fasting blood sugar, serum thyroid-stimulating hormone, fasting serum total cholesterol, and serum vitamin D levels. Patients were followed up for a period of 6 months to 1 year.
Results:
Older age-group has an increased risk of BPPV and recurrence of symptoms. About 45.1% of the patients with BPPV who were detected to have symptoms of hypertension were also more common with hypertensive. Diabetes mellitus was found to have an increased risk of BPPV and its recurrence. The presence of other comorbidities, such as abnormal thyroid function test (9%), sensorineural hearing loss (14%), hypercholesterolemia (46%), and vitamin D deficiency (79%) didn’t show any significant risk for recurrence.
Conclusion:
The presence of comorbidities worsens the status of BPPV, causing more frequent otolith detachment. Hence, it increases the risk of recurrence even after successful repositioning maneuver. Patients presenting with BPPV should therefore be evaluated and treated for these comorbidities along with the repositioning maneuvers.
Introduction
Benign paroxysmal positional vertigo (BPPV) is one of the most common peripheral vestibular conditions which presents in the neurotology clinic. The lifetime prevalence of BPPV is 2.4% 1 and it accounts for about 20% to 30% of vestibular vertigo, 1,2 with the age of onset ranging from 11 to 84 years. 3
Benign paroxysmal positional vertigo occurs due to inappropriate stimulation of semicircular canal hair cells in response to changes in head position, with respect to gravity, by sequestrated otoconia, 3 which have been explained by 2 theories, namely, Schuknecht “cupulolithiasis” theory and Hall “canalolithiasis” theory. 4,5 Many recent studies have found that BPPV can be associated with other illnesses including hypertension, diabetes, thyroid diseases, hyperlipidemia, and vitamin D deficiency and may be responsible for increased frequency of recurrence of BPPV following treatment, thereby worsening quality of life. 6 -10 If such a correlation between common comorbidities and BPPV exists, appropriate treatment of these conditions may be useful in limiting chronicity and reducing the frequency of recurrence.
Materials and Methods
Aims and Objectives
Our study aimed to find the statistical link between BPPV and comorbidities, such as hypertension, diabetes, thyroid disorders, hearing loss, hyperlipidemia, and vitamin D deficiency. We also intended to study the prevalence of comorbidities in patients with BPPV and the relationship between these comorbidities and BPPV. We also tried to define “at-risk groups” for recurrent or chronic BPPV.
Our study was a descriptive analytical study that was carried out in the Department of ENT outpatient clinic of a tertiary care center in India over a period of 18 months. Our study included all patients between 18 and 85 years of age clinically diagnosed as BPPV by history and clinical examination, including Dix-Hallpike test or roll-over test. We excluded patients with other forms of peripheral vertigo and central vertigo; patients with cerebellopontine angle or other intracranial tumors; those who had traumatic head injury, otitis media, and cervical spondylosis; patients who underwent middle ear surgery; those who received chemotherapy or other ototoxic drugs; and pregnant and lactating women.
Detailed history was obtained regarding the onset, duration, and nature of vertigo and other associated symptoms. Detailed history regarding the presence of other comorbid condition was also obtained. Clinical examination included otoscopic examination, tuning fork tests, Dix-Hallpike test, and roll-over test along with the other vestibular examination. Patients who met the inclusion criteria were included in the study. Blood pressure (BP) was recorded. Pure tone audiometry, random blood sugar (RBS)/fasting blood sugar (FBS), serum thyroid-stimulating hormone (TSH), fasting serum total cholesterol, and serum vitamin D levels were estimated. Patients were followed up for a period of 6 months to 1 year.
Hypertension was diagnosed if systolic BP is above 140 mm Hg and diastolic BP >90 mm Hg. Diabetes mellitus was diagnosed when FBS >126, RBS >200, hemoglobin A1c >6.5. Normal TSH value was taken as 0.34 to 5.5 IU. Total cholesterol less than 200 mg/dL is considered normal. For vitamin D, normal value was taken as 10 to 25 IU.
Statistical Analysis
The proportion of various comorbidities arising in the population with BPPV was given as percentages. Recurrence rates were given as percentages. χ2 test was performed to find the correlation between recurrence and comorbidities. A P value <.05 is considered statistically significant.
Observation and Results
A total of 71 patients were included in our study, of which 66 patients had at least 1 comorbidity.
Overall, 56% of the patients were females and 44% were males. The mean age was 49 ± 14 years, with maximum (23.9%) patients ranging between the ages of 41 and 50 years. Age distribution of the patients with BPPV is shown in Figure 1.
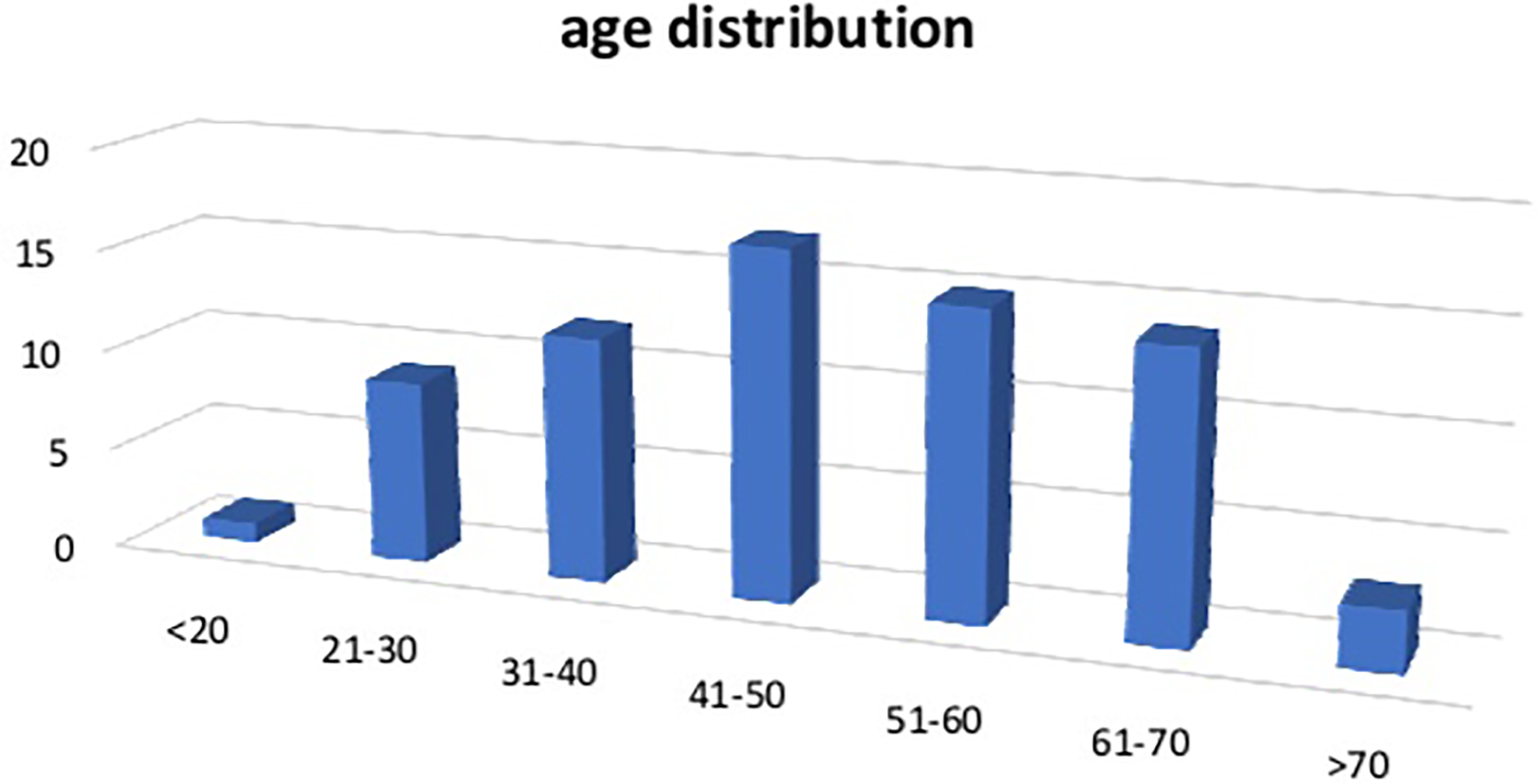
Age distribution of patients with benign paroxysmal positional vertigo.
Dix-Hallpike test showed right-sided canalolithiasis in 40 patients, left-sided canalolithiasis in 29 patients, and bilateral in 2 patients.
In our study, 45.1% of patients were found to have hypertension, of which 15.5% were newly detected. Diabetes mellitus was found in 8 (11%) patients with BPPV. Six patients have hypothyroidism and 1 patient hypothyroid. Only 5 of 71 patients had normal vitamin D levels and 79% with low serum vitamin D levels.
Association Between Recurrence of the Disease and Comorbidity
Recurrence was more commonly seen between the ages of 61 and 70 years. Age distribution of recurrence in patients with BPPV is shown in Table 1.
Age Distribution in Patients With Recurrence of BPPV.
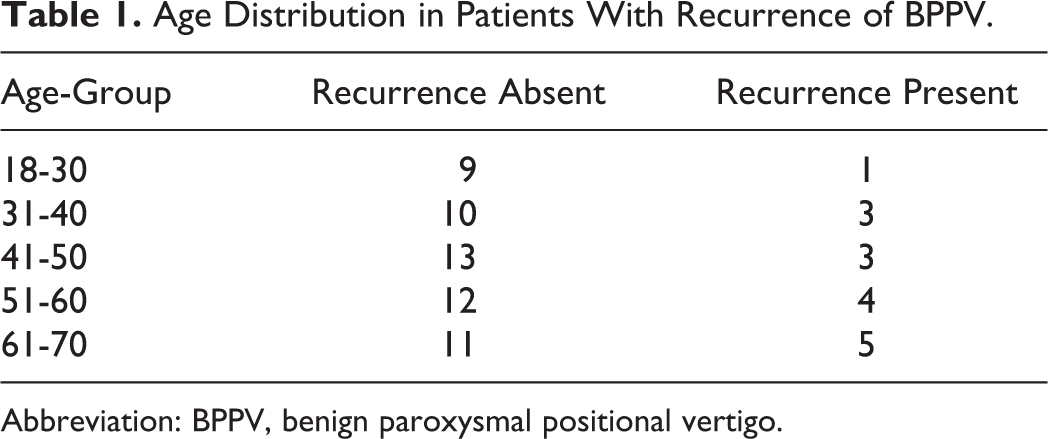
Abbreviation: BPPV, benign paroxysmal positional vertigo.
The recurrence was seen in 38.1% of patients with hypertension as compared to 16% of those without hypertension. The P value is .085 and therefore not statistically significant (Table 2).
Comparison of Presence of Hypertension in Patients With Recurrence of BPPV.
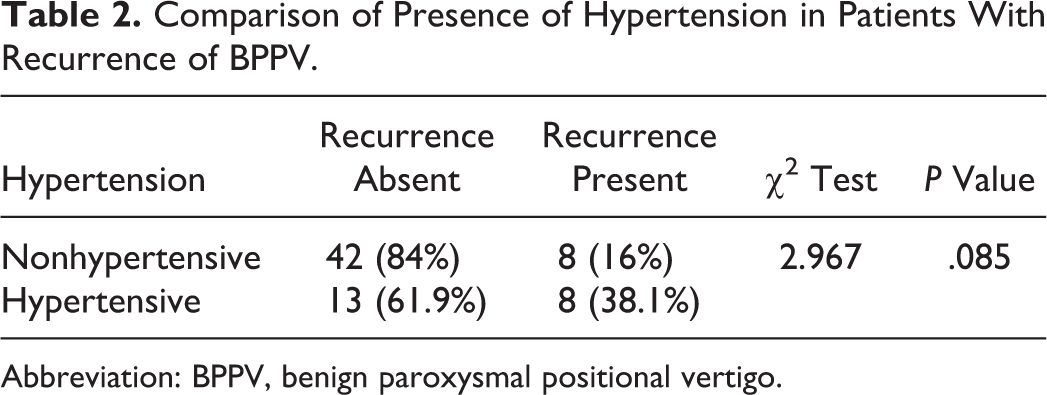
Abbreviation: BPPV, benign paroxysmal positional vertigo.
Of all, 62% of patients who had diabetes mellitus showed recurrence of symptoms with a P value of .015, which is statistically significant (Table 3).
Comparison of Presence of Diabetes Mellitus in Patients With Recurrence of BPPV.
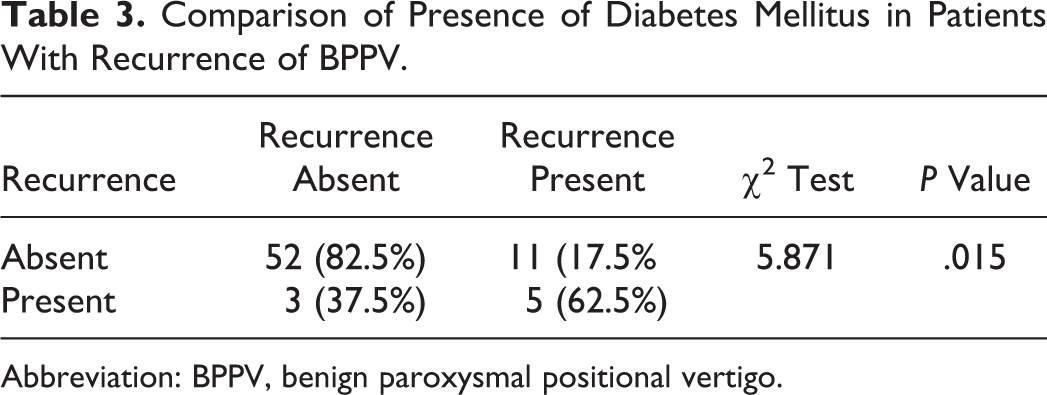
Abbreviation: BPPV, benign paroxysmal positional vertigo.
No statistical significance was found between recurrence of symptoms and ipsilateral hearing loss (Table 4), hypercholesterolemia (Table 5), and serum vitamin D levels (Table 6).
Comparison of Presence of Ipsilateral Sensorineural Hearing Loss in Patients With Recurrence of BPPV.
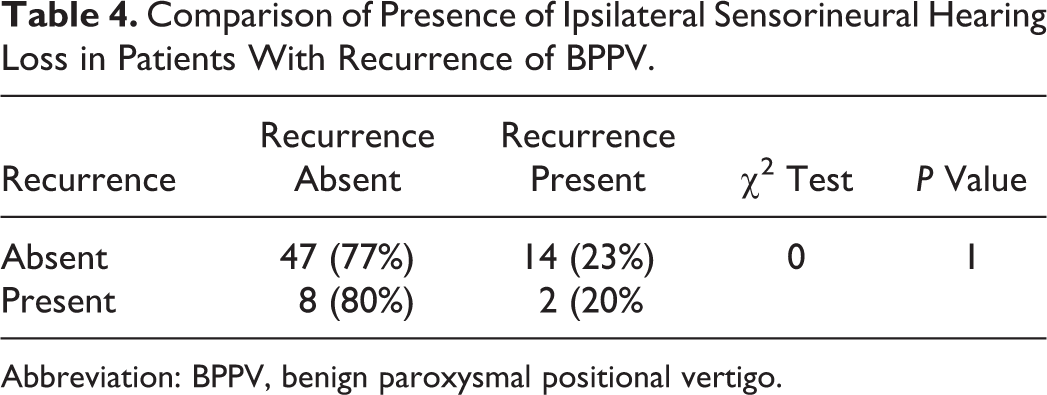
Abbreviation: BPPV, benign paroxysmal positional vertigo.
Comparison of Presence of Hypercholesterolemia in Patients With Recurrence of BPPV.
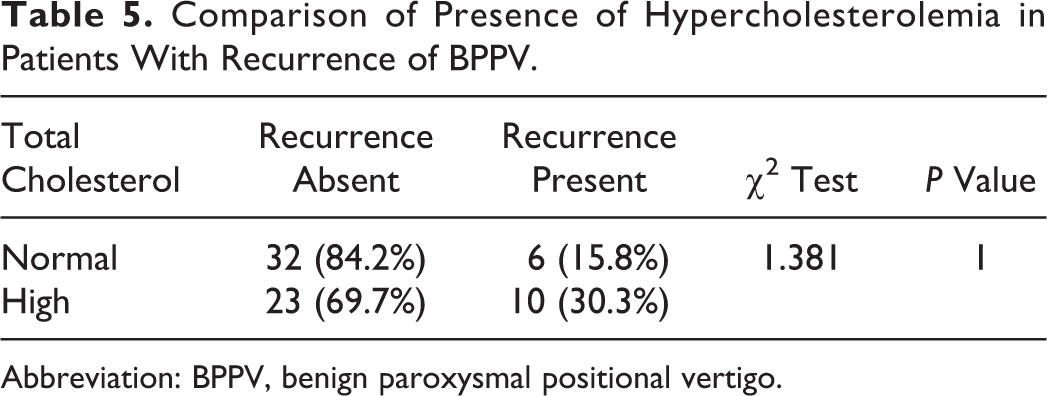
Abbreviation: BPPV, benign paroxysmal positional vertigo.
Comparison of Serum Vitamin D Levels in Patients With Recurrence of BPPV.
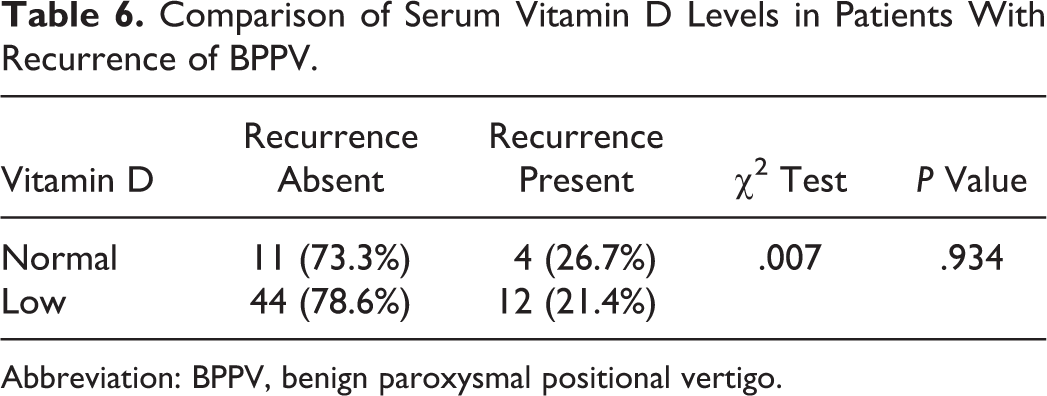
Abbreviation: BPPV, benign paroxysmal positional vertigo.
Discussion
Most studies showed that there is risk for recurrences of symptoms after a successful canalith reposition maneuver in the presence of certain comorbidities such as hypertension and diabetes.
In our study, we evaluated all patients diagnosed with BPPV by obtaining clinical history and performing Dix-Hallpike test. Patients were also evaluated for coexisting comorbidities, such as hypertension, diabetes mellitus, thyroid disorder, ipsilateral SNHL, vitamin D deficiency, and hypercholesterolemia.
In our study, we included 71 patients who were clinically diagnosed with BPPV. Of the 71 patients, 70.9% of patients had at least 1 comorbidity. The patients were followed up for a period of 6 months to 1 year. On follow-up, we found that 22.5% of patients had recurrence even after successful treatment with Epley canalith repositioning maneuver.
The maximum number of patients (23.9%) in our study were in the age-group of 41 to 50 years, with the mean age of 49 ± 13 years. Oghalai et al 11 carried out a study of unrecognized BPPV in elderly patients and found similar results with the maximum age of onset 45 to 60 years. Faralli et al 12 found that the incidence of BPPV increases with age and the prognosis also worsens as age advances. This is because of higher incidence of vascular risk factors in advanced age and also due to age-related degeneration and detachment of otoconia. In addition, it is due to the comorbidities associated with elderly people. 12 -14 We also found that, in addition to incidence, there was an increase in recurrence of BPPV with advanced age. Picciotti et al 14 also found similar results. If the number of comorbidities are equal, patients with recurrence are older on average compared to those without recurrence. The risk for recurrence is 1.6 times more in patients with age more than 65 years. A total of 45% of patients with BPPV were in the age-group >50 years. Recurrence was seen more commonly in older age group, with 56% in >50 years of age. According to our study, there was an increase in incidence and also increase in recurrence as age increases.
In our study, we found that both males and females were affected almost equally—that is, males being 44% and females being 56%. Some studies, however, showed that BPPV is more commonly seen in females 14 and is hypothesized to be due to the hormonal influence. 15,16
Dix-Hallpike test was positive for right-sided canalolithiasis for 40 patients, left side for 29 patients, and bilateral for 2 patients. Epley repositioning maneuver was done for all patients. There is no study, however, which found any increased predilection to a particular side.
In our study, 45.1% of the patients had hypertension. Although only 29.6% of the patients gave a positive history of hypertension, 15.5% were newly detected hypertension. On follow-up, recurrence was seen in 38.1% of patients with hypertension as compared to 16% of those who didn’t have hypertension. Statistical evaluation showed a P value of .085, which is close to significant. Tan et al 17 in their study to evaluate the clinical characteristics and outcome in patients with BPPV and its association with hypertension, compared idiopathic BPPV patients with hypertensive BPPV patients and reported that patients with hypertension had longer median duration of episode. They also reported increased recurrence in hypertensive group compared to idiopathic group. Messina et al 18 found that 55.8% of patients with BPPV had hypertension. They also analyzed the recurrence of disease among patients with BPPV and found that 64.5% of patient with hypertension had recurrence that was found to be significant. 19 De Stefano et al 6 in their multicentric study found the prevalence of hypertension to be higher as compared to other comorbidities (15%). They also found that the risk of recurrence in the presence of hypertension is 2.66. Al-Asadi and Al-Lami, 20 in a cross-sectional study, concurred that the prevalence of BPPV was significantly higher in hypertensive (26.7%) than that in nonhypertensive (18.5%). Korkmaz and Korkmaz 19 also found that the number of reposition maneuver required for successful in patients with hypertension was significantly high compared to others. It is believed that the increased risk for BPPV and its recurrence with hypertension is due to the vascular damage caused by hypertension, which will cause labyrinthine ischemia and thus otoconial detachment. 6,14,18 -20 There are few studies that couldn’t find any correlation between hypertension and BPPV and this could be due to variation in follow-up in these studies. 15,21
D’Silva et al 22 analyzed the otolith function using vestibular evoked myogenic potential and found that diabetes mellitus affects the otolith function. Webster et al 8 in their prospective study found that patient with hyperglycemia has a relative risk of 2.47 times higher for BPPV recurrence, which was statistically significant, whereas patients with a normal glucose–insulin curve test have a relative risk of only 0.22, which was also statistically significant, thus implying normal value may be a protective factor for recurrence of BPPV. In our study, 11% of the patients were diagnosed with diabetes mellitus. Among these patients, 62% showed recurrence and this was found to be statistically significant. This is consistent with other studies, which found diabetes to be a significant risk factor. De Stefano et al 6 found that prevalence of diabetes among their patients were 1.5%. They also concurred that there was significant risk for recurrence in the presence of diabetes mellitus which was 3.33. Picciotti et al 14 found an increased risk of recurrence among patients with diabetes mellitus, with an odds ratio 2.48 with P value <.02. Messina et al 18 studied 2682 patients and found that 17% was affected by diabetes mellitus. They also found that a risk of 1.73 (odds ratio), which was statistically significant, among the diabetic patients. These studies suggest that there is instability of otoconia. This is mainly because of microangiopathy due to diabetes and thus labyrinthine ischemia. 14,18 Diabetes-associated neuropathy and vasculopathy also contribute to otoconial degeneration and thus precipitate BPPV. Diabetic patients have poorer capacity for recovery from mild insults, such as viral infections or mild trauma, in effect making these insults more severe. This also predispose to BPPV. A combination of age-related and diabetic-related pathophysiologic mechanisms for otoconial degeneration and thus instability could affect this subgroup. 23 However, there were few studies that found no significant rate of recurrence among diabetic patients. 18,24,15
In our study, we evaluated patients with serum TSH. Of 71 patients, 9% of patients have hypothyroidism and 1% had hyperthyroidism. No recurrence was seen among these patients. Picciottti et al 14 found that there is risk for recurrence in patients with thyroid disorders, with odds ratio of 2.79 and P value of <.0005. They haven’t specified the type of thyroid disorders where recurrence was found. There are some recent studies which suggest that it’s not the hypothyroidism that predisposes to BPPV, but the autoimmune thyroiditis that causes BPPV. 20,25 Papi et al 26 found that the association of BPPV with elevated antithyroid antibodies (odds ratio 25.6) was higher than that of BPPV with hypothyroidism (odds ratio 12.9). Modugno et al 25 found that some autoimmune alterations were found in 70 (48.5%) patients. The serum antithyroid antibodies were found to be high in 27.1%. Thus, they found that the incidence of thyroiditis in patients with BPPV was found to be significantly higher than that in control group.
The prevalence of vitamin D deficiency in patients diagnosed with BPPV was high as 79%. The recurrence among patients with vitamin D deficiency (21.4%) was not statistically significant. Jeong et al 9 studied 100 patients with idiopathic BPPV and 192 controls and found that serum vitamin D levels are significantly lower in the idiopathic patients compared to the controls. Although there are many studies reporting that vitamin D deficiency is a risk of recurrence in BBPV, in our study we couldn’t find any correlation in the risk of recurrence. The prevalence of vitamin D deficiency in patients with BPPV was high though. To understand the significance, we should further research an analytical study with a longer follow-up. The recurrence rate would have been less if vitamin D supplementations were started. Büki et al 10 evaluated the relation between vitamin D deficiency and BPPV and found that the vertigo improves after vitamin D supplementation. Taalat et al 27 evaluated reduction in recurrence rate of BPPV following treatment for severe vitamin D deficiency and found that there is significant decrease in the recurrence rate following improvement in serum 25-hydroxyvitamin D3. Vitamin D plays a crucial role in homeostasis of calcium and phosphorus. Otoconia, similar to bone, are a result of ordered deposition of inorganic calcium carbonate (calcium phosphate in bone) crystallites onto a preformed framework of organic matrix. However, the calcium for otoconia formation is from the endolymph, which is extruded from the hair cells. Hence, it is cleared that there are significant differences between bone and otoconia formation. Therefore, serum markers of turnover are not expected to be directly involved in pathogenesis of BPPV. 10,27,25
The prevalence of vitamin D deficiency is high in the general population. Unlike the tendencies in the literature, our study suggests that vitamin D deficiency is not risk factor for BPPV. The coexistence of BPPV with vitamin D deficiency is coincidental. However, an analytical study with a more sample size may help to give a more accurate result.
Ipsilateral sensorineural hearing loss was seen in 14% of patients with BPPV. Recurrence was seen in 20% of patients with unilateral SNHL as compared to 23% of those without SNHL. This was not statistically significant. Kim et al 28 evaluated 4 patients with concurrent BPPV and SNHL and found that concurrent BPPV with ipsilateral SNHL may be caused by blood debris due to inner ear hemorrhage. Kim et al 29 found that 125 patients had ipsilateral SNHL. Benign paroxysmal positional vertigo associated with SNHL required more canal reposition maneuver as compared to others. There are studies reporting that BPPV and SNHL could be coexisting as the inner ear as a whole get affected by the insult. However, our study didn’t show any such correlation.
46% of patients had hypercholesterolemia. The recurrence was seen in 30.3% of patients with hypercholesterolemia, whereas 15.8% among patients with normal serum cholesterol level. There are studies showing a significant risk in patients with hypercholesterolemia. This is due to risk for cardiovascular comorbidities like artheriosclerosis. 30,31 In our study, we evaluated only by fasting serum total cholesterol. If we have studied more number of patients with the complete lipid profile, then the analysis would have been better.
Limitations of the Study
If the study was conducted in a larger group, the comorbidities like hypertension would have shown a significant risk for recurrence. It was not an analytical study; hence, there was no comparable group. So, the significance in prevalence of comorbidity in patients with BPPV couldn’t be evaluated. The follow-up period ranged from 6 months to 1 year. It was not uniform. If patients are followed up for longer time, the recurrence rate would have increased.
Conclusion
In our study, we conclude that the presence of comorbidities will worsen the status of BPPV, causing more frequent otolith detachment. Hence, it will increase the risk for recurrence even after successful repositioning maneuver. Hence, patients presenting with BPPV should be evaluated and treated for the comorbidities along with the repositioning maneuvers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.