
Abstract
Laryngeal carcinomas are the most common upper respiratory tract cancers and most commonly involve the glottic region. The aim of this study is to evaluate the voice quality after radiotherapy (RT) and microsurgical cordectomy (MC) treatments using Voice Handicap Index (VHI) and Grade, Roughness, Breathiness, Astenicity, and Strain (GRBAS) perceptual evaluation scale in patients with early-stage glottic carcinoma. A total of 37 patients with early-stage glottic carcinomas, 19 patients had RT and 18 patients with MC, were included in our study. The patients were evaluated in terms of their sound quality by using VHI-10 and GRBAS perceptual assessment scale 3 months after the treatment was completed. Although the findings were better in favor of RT according to GRBAS perceptual assessment scale of patients who received RT (n = 19) and MC (n = 18), no statistically significant difference was found between the 2 groups (P = .613). Patients in both groups were evaluated with VHI-10, emotional (P = .036) and physiological (P = .038) scores were significantly higher in MC group and no significant difference was found in functional scores (P = .192). However, there was no statistically significant difference between the 2 groups in terms of voice quality (P = .185). In early-stage (Tis, T1a, T1b) glottic carcinoma, there was no significant difference between RT and MC in terms of voice quality. Therefore, the choice of treatment modality in patients with early-stage glottic carcinoma should be taken into account in terms of the patient’s occupation, comorbid diseases, cost of treatment, hospital stay, and, most importantly, patient preference.
Introduction
Laryngeal cancers constitute 2% of all cancers and 25% of head and neck cancer. It is the most common upper respiratory tract cancer. 1 Laryngeal carcinomas most commonly involve the glottic region (60%-65%). 2,3 There is hoarseness associated with vocal cord involvement in glottic carcinomas, which leads to early diagnosis and more successful treatment. 4 The most common histological type of laryngeal cancer is the squamous cell carcinoma (SCC). Because of the poor lymphatic drainage of the glottic region, the possibility of lymph node or distant metastasis of early-stage glottic carcinomas is quite low. 5 Common lesions including the in situ tumors of the vocal cords, which hold the vocal cords but do not impair their movement, have been described as early-stage glottic cancers. 6 The choice of treatment method in early-stage (T1-2 N0M0) tumors depends on the patient’s age, sex, profession, tumor histology, tumor extension, the presence of metastasis, patient performance, surgical team experience, and patient preference. 7,8 Transoral laser excision, open partial laryngectomy, or local radiotherapy (RT) is commonly used treatment option in early-stage glottic larynx cancers. 9 Local control rates in T1 tumors without anterior commissure involvement were 71% to 100% in laser surgery and 73% to 95% in RT. 10 In patients with T1a glottic carcinoma, the choice of treatment depends on quality of life and especially voice quality. 11,12 The aim of this study is to evaluate the voice functions of patients with early-stage laryngeal carcinoma (Tis, T1a, T1b) using the Voice Handicap Index (VHI) and Grade, Roughness, Breathiness, Astenicity, and Strain (GRBAS) perceptual assessment scale after RT and transoral cold cordectomy treatments.
Materials and Methods
Study Protocol
The study was started after obtaining approval from the local ethics committee (No. TUEK1-2019BADK/1-6). Patients who were admitted to the Otorhinolaryngology Department of Health Science University Samsun Training and Research Hospital with complaints of hoarseness and diagnosed as early-stage glottic carcinoma were included in the study between January 2016 and December 2018. The patients who were admitted to our clinic with complaints of hoarseness were examined by indirect laryngeal endoscopy. The patients who had laryngeal pathology underwent biopsy by suspension direct laryngoscopy under general anesthesia.
Patients
As a result of the pathology, the cases reported as carcinoma in situ and SCC in the glottic region were staged according to the American Joint Committee on Cancer. According to this staging, patients with Tis, T1a, and T1b tumor stage and who did not have clinically detected neck metastases were included in the study. All patients were evaluated as multidisciplinary in the tumor council of our hospital, and RT and microsurgical cordectomy (MC) treatment options were presented to the patients. Two treatment options were explained to the patients. Patients were divided into 2 groups as RT group and MC group according to the treatment they chose.
Irradiation was performed in a supine position, using a thermoplastic mask to fix the head and neck area and shoulders throughout the treatment, a total of 63 Gy (2.25 Gy/fraction) or 66 Gy (2 Gy/fraction; dose adjusted according to the condition of the patients) 5 days a week 1 fraction per day. The irradiation area was limited in the posterior prevertebral fascia, superior hyoid subcutaneous bone, inferior cricoid cartilage inferior border, and anterior region at a distance of 1 to 2 cm. Microsurgical cordectomy group underwent microsurgical cordectomy using a microscope with suspension laryngoscopy method under general anesthesia.
In order to evaluate the vocal competence of the patients who completed the third month after the treatment, the VHI-10 and the GRBAS perceptual assessment scale were used to evaluate the voice quality. VHI-10 consists of 3 physical, 3 functional, and 4 emotional questions. Each question is given by the patient between 0 and 4 points (0 = never, 1 = rarely, 2 = sometimes, 3 = often, 4 = always). The total score ranges from 0 to 40. A high score indicates that the patient’s voice is not good. The GRBAS scores were evaluated as voice quality parameters. The evaluation was made by 2 language and speech therapists and the forms were filled in and recorded. The evaluation was made by giving a score of 0 to 3 (0 = normal, 1 = mildly affected, 2 = moderately affected, 3 = highly affected). The total score ranges from 0 to 15. Perceptual evaluation scale was completed with the participation of 19 patients who underwent RT and 18 patients who underwent MC. In addition, age, gender, smoking, and comorbid diseases were evaluated in these 2 groups.
Statistical Analysis
SPSS version 15.0 for Windows (SPSS Inc, Chicago, Illinois) package program was used. The Kolmogorov-Smirnov test was used to determine whether the data were within normal distribution. In the comparison of the data of the 2 independent groups, the t test was used if the normal distribution was not compatible and the Mann-Whitney U test was used if compatible. The χ2 test was used to compare the data groups. P < .05 was considered significant.
Results
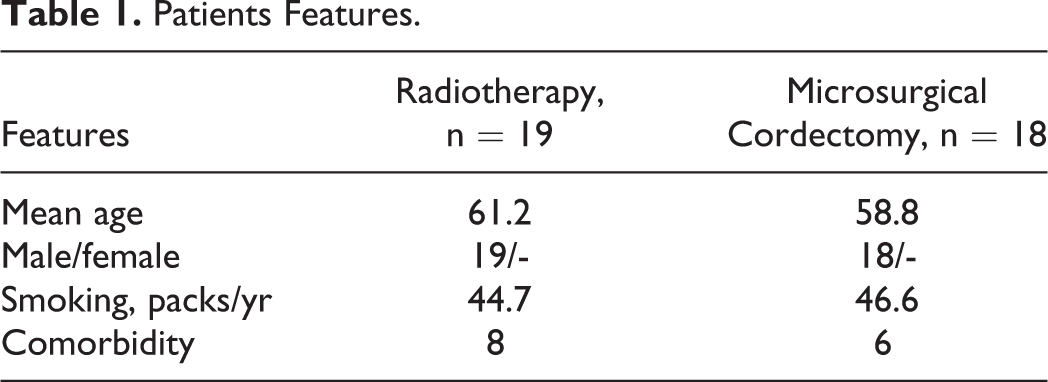
All 37 patients included in the study were male. The ages of the patients ranged from 36 to 79 years, with a mean age of 58.8 years. The mean age was 61.2 years in the RT (n = 19) group and 56.4 years in the MC (n = 18) group. The age difference between the 2 groups was not statistically significant (P = .284). Table 1 summarizes the demographic data and additional factors available for the patients. No significant difference was found between the patient groups in terms of age, gender, smoking, and comorbidity (P > .05).
Patients Features.
All the patients in the RT group were SCC. Fifteen cases were T1a and 4 cases were T1b. In the MC group, 12 cases were Tis and 6 cases were T1a. There was no case with anterior commissure involvement in the MC group. There were 3 cases in T1a cases and 4 cases of T1b cases in the RT group that anterior commissure involved.
The results of VHI by groups are summarized in Table 2. There was no significant difference between the groups in terms of total VHI score and functional voice scores. But physiological and emotional scores were significantly higher in the MC group.
Voice Handicap Index Scores.
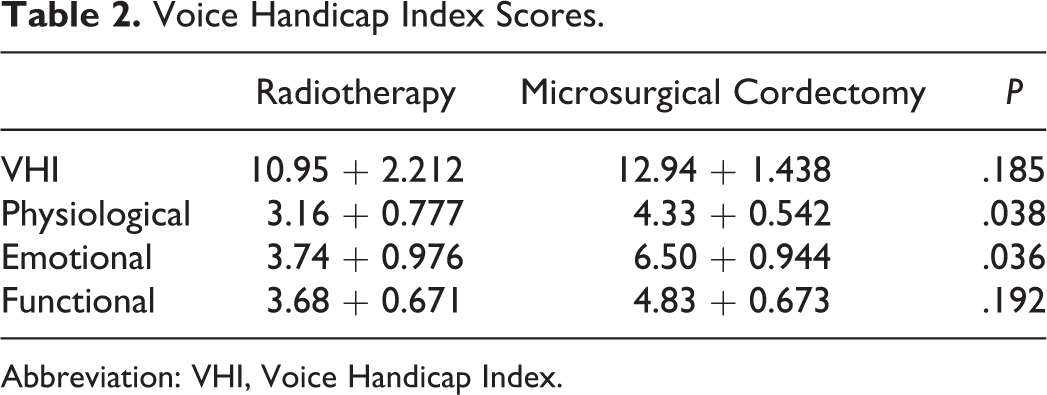
Abbreviation: VHI, Voice Handicap Index.
The total GRBAS score was found to be 5.05 + 0.495 in the RT group and 5.22 + 0.552 in the MC group. There was no significant difference between the groups in terms of total GRBAS score (P = .613). The GRBAS scores of the groups are summarized in Tables 3 and 4.
GRBAS Scores in RT Group (n = 19).
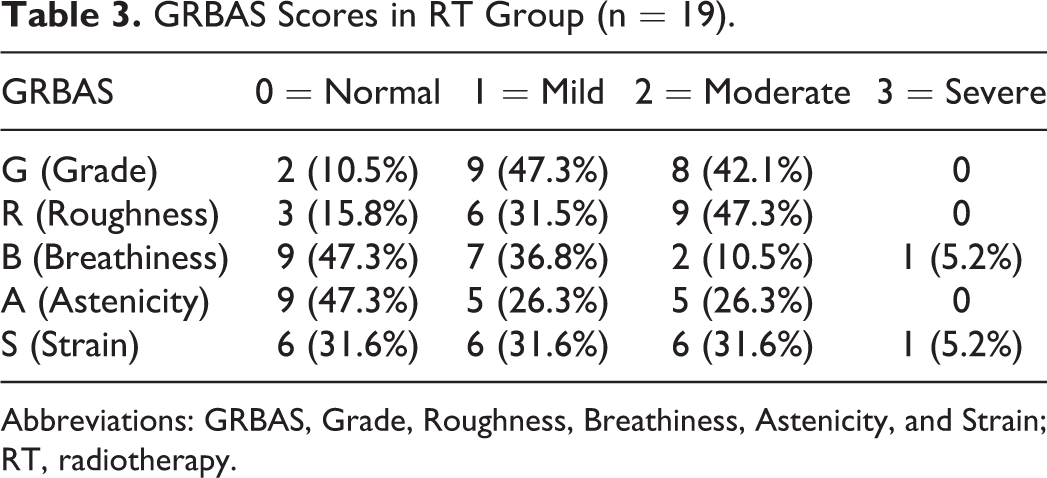
Abbreviations: GRBAS, Grade, Roughness, Breathiness, Astenicity, and Strain; RT, radiotherapy.
GRBAS Scores in MC Group (n = 18).
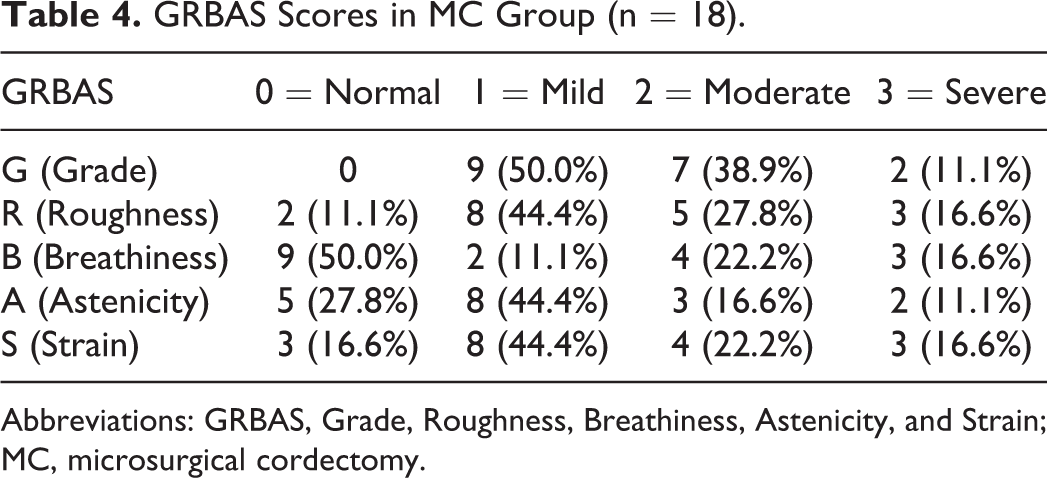
Abbreviations: GRBAS, Grade, Roughness, Breathiness, Astenicity, and Strain; MC, microsurgical cordectomy.
Discussion
Laryngeal cancers constitute 2% of all cancers and 25% of head and neck cancers. Laryngeal cancers are most commonly seen between 50 and 70 years of age. Men are 5 times more likely than women. 1 The age of the 37 patients included in our study ranged from 36 to 79 years, with an average of 58.2 years. The age difference between the RT group (61.2 years) and the MC group (56.4 years) was not statistically significant (P = .273). All of the patients in our study were male.
Smoking is the most important factor in the etiology of laryngeal cancers. It is extremely rare for nonsmokers to be seen. Cancer risk is directly proportional to smoking cigarettes. 13 In our study, there was no smoking history in 3 patients in the RT group, while the others had a smoking rate of 46.6 packs/yr. In the MC group, 1 patient had stopped smoking 30 years ago. The other 17 patients had a smoking history of 44.7 packs/yr. The difference between the 2 groups was not statistically significant (P = .590).
Mendenhall et al 7 studied the transoral laser excision, open partial surgery, and RT in patients with early-stage glottic (T1-T2) laryngeal cancer. One of the parameters evaluated in this meta-analysis is the voice quality. The voice quality is similar after transoral laser excision or RT for the limited T1a tumor. However, laser resection of larger tumors may likely lead to worse outcomes. In another meta-analysis, Greulich et al 14 included 8 retrospective cohort studies. A total of 155 patients (total 362 patients) who underwent laser surgery were included in the study. Then, VHI data of the patients were evaluated after treatment. They reported that it was difficult to determine the time to VHI evaluation after treatment, but the evaluations were performed in more than 6 months. As a result of the evaluation, there were positive results in favor of RT in 2 articles, whereas there was no difference between RT and transoral laser cordectomy in 6 articles. In the meta-analysis of VHI, good results were in favor of RT, but the difference between the 2 groups was not statistically significant.
Sjögren et al 15 published results of 34 patients who had T1a glottic carcinoma that 16 of them received RT and 18 had laser surgery. They underwent a cordectomy with types 1 and 2 cordectomy. All patients were reported as SCC. In the RT group and 8 patients from the laser cordectomy group, both the VHI and the GRABS perceptual assessment scale were compared between the 2 groups. It was found that VHI was 17.6 in the RT group and 19.2 in the laser cordectomy group. However, the difference was not statistically significant. Although the statistical difference was found in favor of RT in VHI functional and emotional scores, they found no significant difference in physical scores between RT and transoral laser cordectomy. On the GRBAS perceptual assessment scale, 56% of the RT group and 38% of the laser cordectomy group were evaluated as normal sound, but the difference between these numbers was not statistically significant. In our study, VHI was found to be 10.95 in the RT group and 12.94 in the MC group. Although the VHI evaluation was better in the RT group, the difference between the 2 groups was not statistically significant (P = .185).
Laoufi et al 16 evaluated 95 patients with T1a glottic carcinoma using VHI-30 and found that there were 51 patients 8 years after RT and 44 patients 4 years after surgery. As a result of the evaluation, the long-term RT (13.1) group reported that the result was better than the laser surgery group (29.2) in terms of physical, functional, and emotional factors. In our study, the difference between the 2 groups was statistically significant in favor of the RT group as a result of the VHI physiological (P = .038) and emotional (P = .036) evaluation questions of the patients in the RT and MC groups, but the difference between the functional evaluation was not significant (P = .192). Although there was no difference in total VHI scores between the 2 groups, we think that physiological and emotional scores were significantly lower in the RT group in terms of informing our patients. Because this difference between the groups can change the patient’s expectation from the outcome of the treatment.
Nunez Batalla et al 17 published results of 37 patients with glottic carcinoma of which 19 patients treated with CO2 laser surgery and 18 patients treated with RT. After the treatment, the patients were evaluated with GRBAS scale. They detected mild dysphonia in 31.5%, moderate dysphonia in 37%, and severe dysphonia in 31.5% according to the GRBAS score treated with laser therapy. The GRBAS results of patients treated with RT revealed normal voice in 11%, mild dysphonia in 44.4%, moderate dysphonia in 27.8%, and severe dysphonia in 16.7%. In comparison of the results of the GRBAS scale, no significant difference was found between each group. In our study, 30.5% of the patients’ voice was normal, 34.7% of them were mildly affected, 31.6% of the patients were moderately affected, and 2.1% of the patients were highly affected in the RT group. In the MC group, 21.1% of the patients had normal voice, 38.9% had mildly affected, 25.5% had moderately affected, and 11.5% had severely affected voice. In our study, there was no statistically significant difference between the 2 groups in the GRBAS perceptual assessment scale (P = .613). In conclusion, it was determined that the difference between the 2 groups was not statistically significant as a result of total VHI scores and GRBAS perceptual analysis after RT and MC application to patients with early-stage glottic carcinoma. There is no difference between functional voice results in early-stage glottic carcinoma between RT or surgery both in the literature and our study. In this situation, the choice of treatment method in patients with early-stage glottic carcinoma should be considered according to the patient’s age, occupation, comorbid diseases, cost of treatment, hospital stay, and, most importantly, patient preference.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.