
Abstract
Background:
Open rhinoplasty has been performed for over 50 years. Rhinoplasty procedures have a risk of complications and it is important to follow each step diligently in order to avoid complications. Periorbital edema is the most common complication of septorhinoplasty. As far as we are aware, there are no studies in the available literature examining the impact of the septorhinoplasty on intraocular pressure and the retina.
Objectives:
The aim of this study was to evaluate the effects of septorhinoplasty-related periorbital edema on intraocular pressure and the retina by means of objective tests.
Methods:
Ten patients with phase 4 periorbital edema (5 males and 5 females) who underwent open rhinoplasty with bilateral lateral osteotomies were enrolled in the study. All the patients were examined by an eye specialist for visual acuity, intraocular pressure, retinal nerve fiber layer, and ganglion cell complex pathologies with optical coherence tomography preoperatively and postoperatively on the seventh day.
Results:
Preoperative and postoperative best-corrected visual acuity; intraocular pressure; average, superior, and inferior retinal nerve fiber layer thickness; and total, superior, and inferior ganglion cell complex thickness in both eyes for all patients were within normal limits. There was no statistical difference between preoperative and postoperative values (P > .05).
Conclusion:
We concluded that periorbital edema after septorhinoplasty causes no significant complications affecting intraocular pressure and visual acuity. We believe that when osteotomies and local anesthetic injections are undertaken correctly, periorbital complications do not affect vision.
Keywords
Introduction
The open rhinoplasty has been performed for over 50 years. 1 The surgeon aims to achieve the combination of aesthetic suitability with the surrounding facial features and protection or correction of nasal function and support. 2
Rhinoplasty has a risk of minor and major complications in severe cases. 3,4 The rate of complications following rhinoplasty surgery is 5% to 18%. 5 Periorbital and orbital complications can be vascular, infectious, or traumatic in rhinoplasty. 6 -8 Lateral osteotomies cause most of the sudden orbital–periorbital complications. The shearing or tearing of the tissue involving the angular vessels can cause orbital hemorrhage. Because of the confined space of the orbit, significant orbital hemorrhage can increase intraocular pressure (IOP). Regular IOP is necessary for normal vision. The aqueous formation and drainage affects the IOP. The IOP elevation can cause cataract, iris atrophy, corneal edema, and optic nerve atrophy. Sensation of pressure in the eyes, epiphora, blurred vision, headache, nausea, or vomiting are the symptoms of increased IOP. 9 The relationship between conventional and endoscopic sinus surgery and IOP has been described in some articles. 10 -12 However, no reports have delineated the possible effects of septorhinoplasty on IOP.
The other reported serious orbital complication is related to injection of local anesthetics. Injection of local anesthetic into artery while doing mucosa injection during surgery can lead to occlusion of the vessels of the optic nerve. There are few cases which had visual loss following injection of local anesthetic into the nasal mucosa during septorhinoplasty. 13 -15 Furthermore, there is only one case that showed a possible association between postoperative stress and central serous chorioretinopathy in a rhinoplasty patient using xylometazoline. 16
Optical coherence tomography (OCT) provides cross-sectional images of ocular tissues. 17,18 It has been used to quantify different retinal layers in retinal diseases as well as retinal nerve fiber layer (RNFL). 19
To the best of our knowledge, there are no studies in the literature examining the impact of septorhinoplasty on the eye by means of objective tests. The aim of this study was to evaluate the possible effects of septorhinoplasty on IOP and the retina.
Materials and Methods
This prospective study was conducted at our otorhinolaryngology clinic. The study was approved by the ethics committee of our hospital on March 16, 2016, no: 2011-KAEK-25 2016/05-02. All patients signed informed consent prior to participation in the study.
Patients
In our clinic, both eyes of 40 patients were examined preoperatively by an eye specialist for visual acuity, IOP, RNFL, and ganglion cell complex (GCC) thickness. The patients’ periorbital edema and periorbital ecchymose were assessed and graded separately from 0 to 4 according to Gürlek’ grading system. 20 The study group included 10 patients with grade 4 periorbital edema and grade 4 periorbital ecchymose (5 males, 5 females; mean age was 27.7 ± 8.1 years; Figures 1 and 2). Patients without periorbital edema or orbital complication, patients with diabetes mellitus, hypertension, glaucoma, ocular hypertension, history of sinonasal or ocular surgery, previous ocular trauma, and previous use of topical corticosteroid eyedrops were excluded.

Patient 1 with periorbital edema ecchymosis.

Patient 2 with periorbital edema ecchymosis.
Preincisional surgical field infiltration was performed with lidocaine (2%) and epinephrine (1:200,000). All patients underwent open rhinoplasty with bilateral lateral osteotomies with the authors in our otorhinolaryngology clinic. Blood pressure was monitored during surgery and the postoperative period. Following anesthetic induction, all patients received a continuous remifentanil infusion of 0.2 to 0.5 μg/kg/min to maintain a mean arterial pressure of 85 to 90 mm Hg. All patients had silicone nasal packing for 7 days postoperatively. Both eyes of 10 patients were examined preoperatively and postoperatively seventh day by an eye specialist for visual acuity, IOP, RNFL, and GCC thickness, prior to removal of packing. Physiological factors, such as heart rate and systolic and diastolic blood pressures, were recorded 10 minutes following each IOP measurement.
Ocular Tests
Binocular visual acuity for each eye was measured in all patients with a Snellen 10 ft wall chart and recorded as a decimal representation of 10/×, such that 10/10 = 1.0 and represents “normal” visual acuity. Best-corrected visual acuity was 10/10 = 1.0 in all patients preoperatively.
Intraocular pressure (mm Hg) for each eye was measured with Topcon noncontact tonometer CT-1P (Topcon, Tokyo, Japan). Average, superior, and inferior RNFL thickness (µm) and total, superior, and inferior GCC thickness (µm) for each eye were measured using spectral domain optical coherence tomography (SD-OCT; Avanti RTVue XR100-2; Optovue Inc, Fremont, California; Figures 3 and 4).
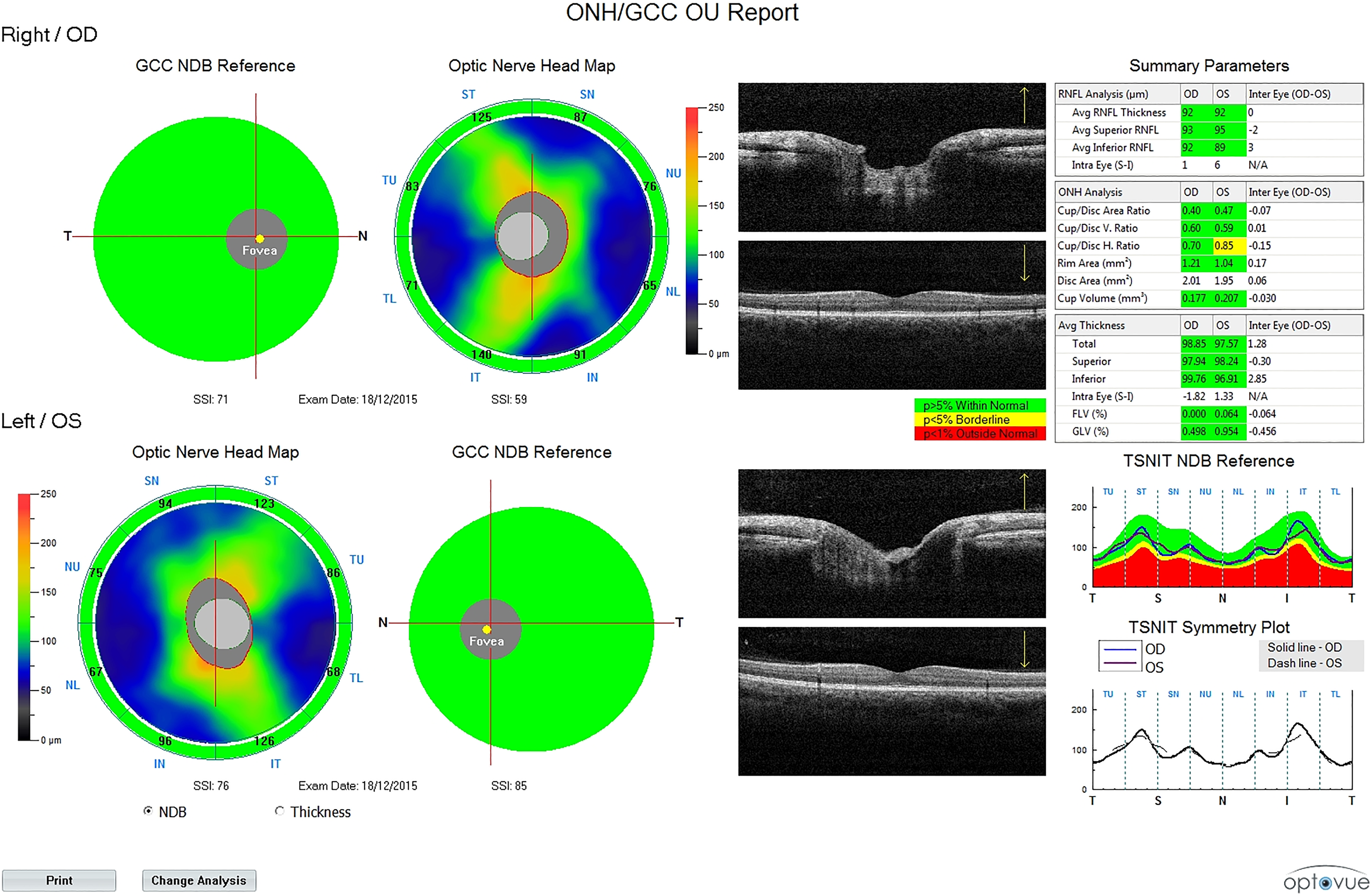
Preoperative spectral domain optical coherence tomography report.
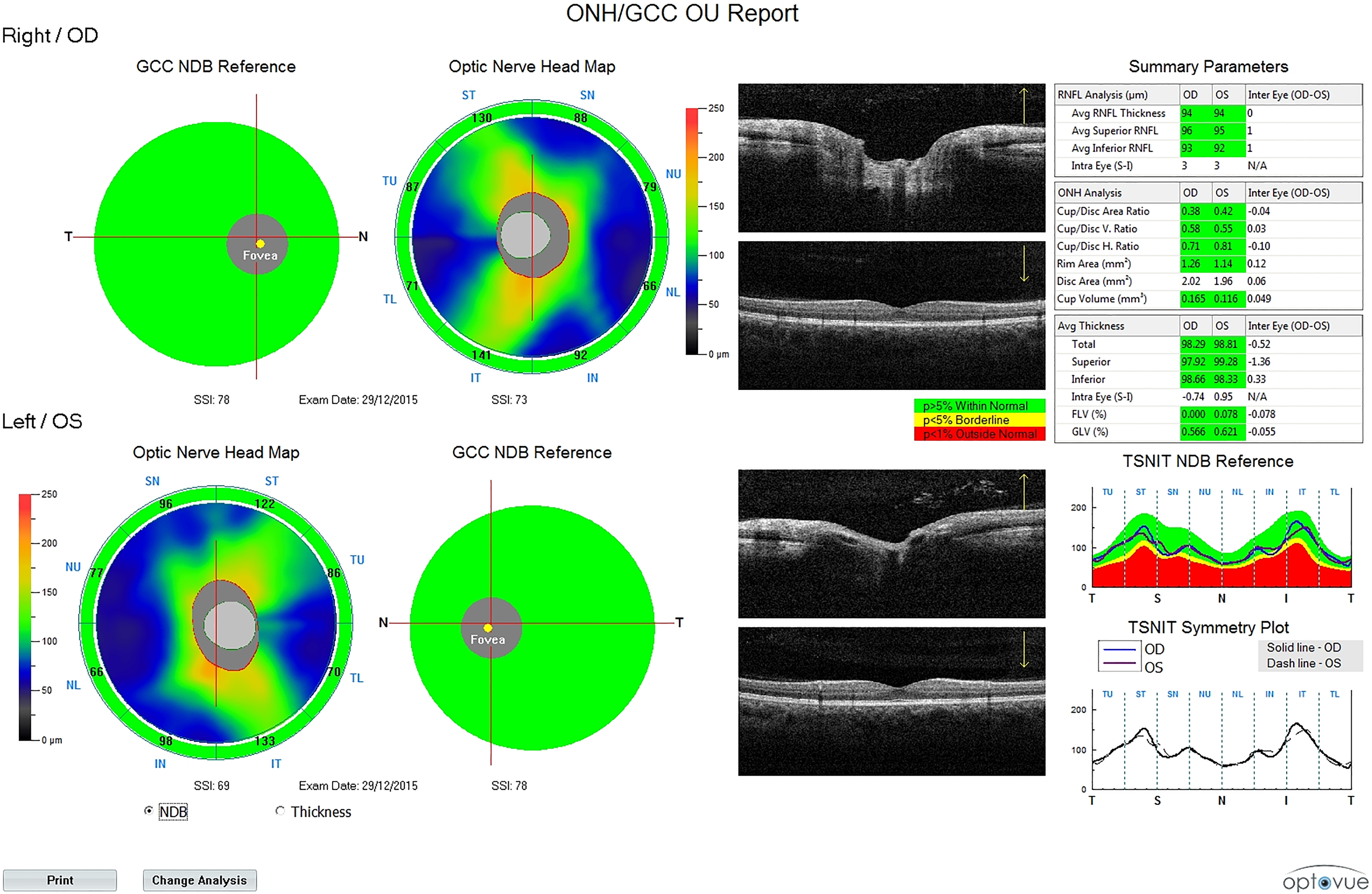
Postoperative spectral domain optical coherence tomography report.
Statistical Analysis
SPSS software (SSPS version 16.0) was used for statistical calculations. Results were expressed as mean ± standard deviation. Wilcoxon signed-ranks test was used. A P value of <.05 was considered to indicate statistical significance.
Results
Subconjunctival ecchymosis was present in 2 patients. All patients had grade 4 periorbital edema and grade 4 ecchymosis. The subconjunctival ecchymosis resolved in 14 days. Other complications were also recorded.
Best-corrected visual acuity was 10/10 = 1.0 in all patients preoperatively and postoperatively. Preoperative and postoperative IOP for all patients were within normal limits. The mean IOP of each eye preoperatively was right 15.10 ± 2.23 mm Hg (range, 12.0-19.0 mm Hg), left 14.70 ± 1.63 mm Hg (range, 11.0-17.0 mm Hg), and postoperatively was right 15.60 ± 2.91 mm Hg (range, 12.0-20.0 mm Hg), left 15.50 ± 1.77 mm Hg (range, 13.0-18.0 mm Hg) on day 7 prior to removal of the nasal packs (Table 1).
Age, Gender, Right and Left Visual Acuity, Preoperative and Postoperative Intraocular Pressure for Each Eye, Blood Pressure (mm Hg).
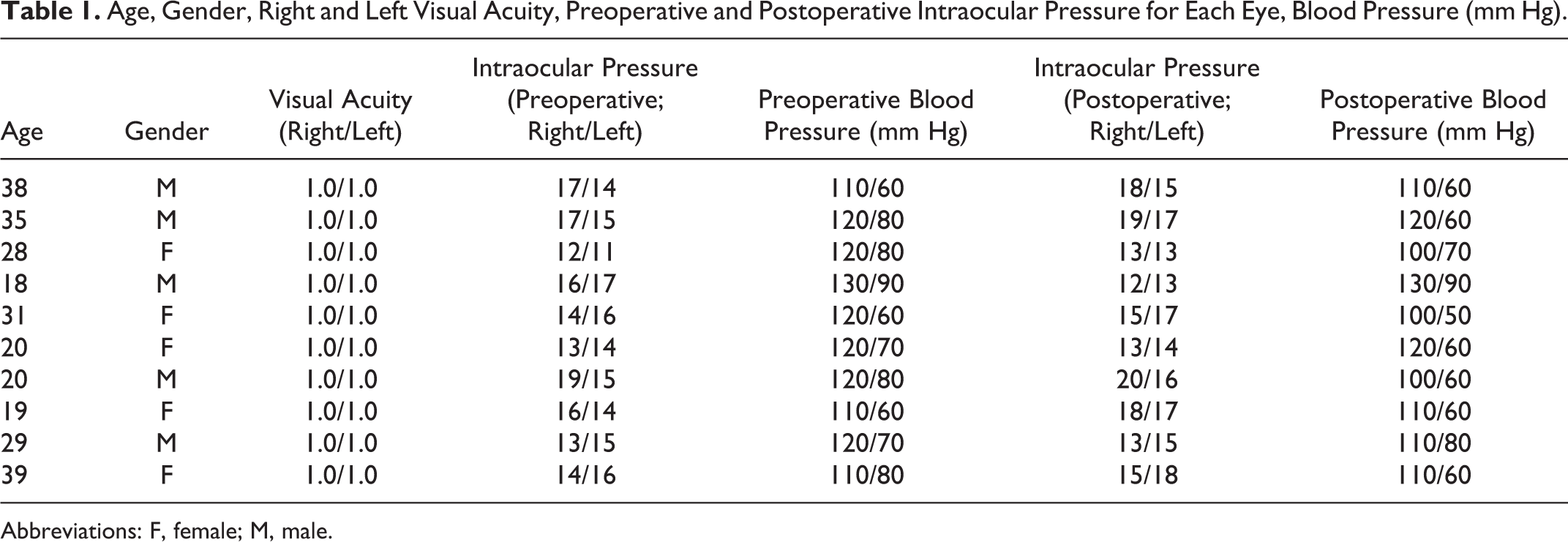
Abbreviations: F, female; M, male.
The mean systolic blood pressure 10 minutes after each IOP measurement was 118 ± 6.3 mm Hg preoperatively and 110 ± 8.1 mm Hg postoperatively. Mean diastolic blood pressure 10 minutes after each IOP measurement was 73 ± 10.5 mm Hg preoperatively and 64.5 ± 10.6 mm Hg postoperatively. Mean heart rate 10 minutes after each IOP measurement was 82.00 ± 10.05/min preoperatively and 85.00 ± 5.27/min postoperatively (Table 1). The IOP-related factors of heart rate and systolic blood pressures also showed no significant difference (P > .05). Diastolic blood pressures showed significant difference (P = .046; Table 2).
Changes in Left and Right Intraocular Pressure, Systolic Blood Pressure (mm Hg), and Diastolic Blood Pressure (mm Hg), Heart Rate (beats/minute).
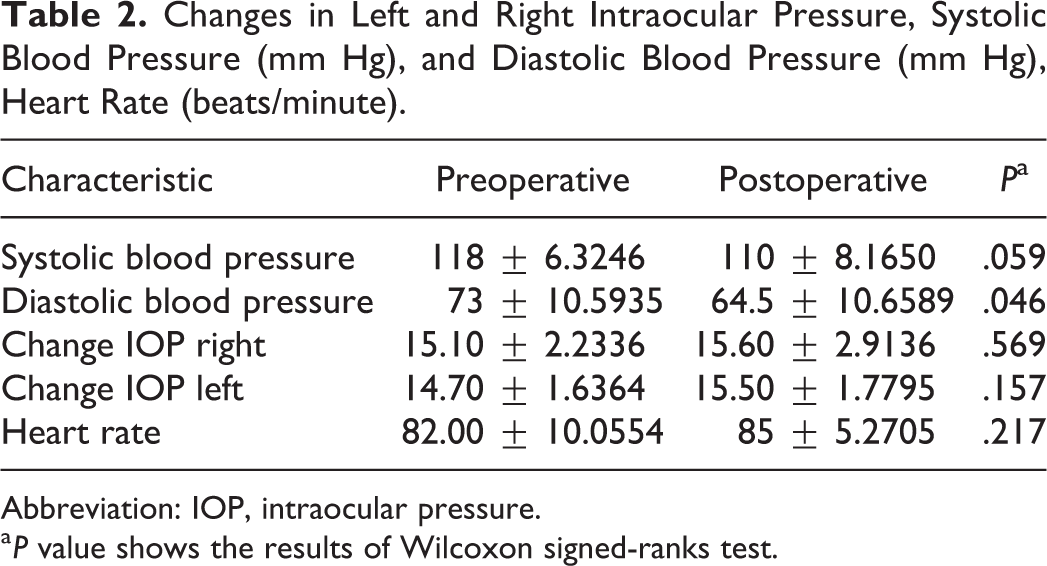
Abbreviation: IOP, intraocular pressure.
a P value shows the results of Wilcoxon signed-ranks test.
Preoperative and postoperative average, superior, and inferior RNFL thickness and total, superior, and inferior GCC thickness for each eye were within normal limits (Tables 3 and 4). There was no statistical difference between preoperative and postoperative average, superior, and inferior RNFL thickness and total, superior, and inferior GCC thickness for all patients’ values (P > .05; Table 5).
Total, Superior, and Inferior Ganglion Cell Complex Thickness (µm) for Each Eye Was Measured Using Spectral Domain Optical Coherence Tomography: Preoperative and Postoperative.
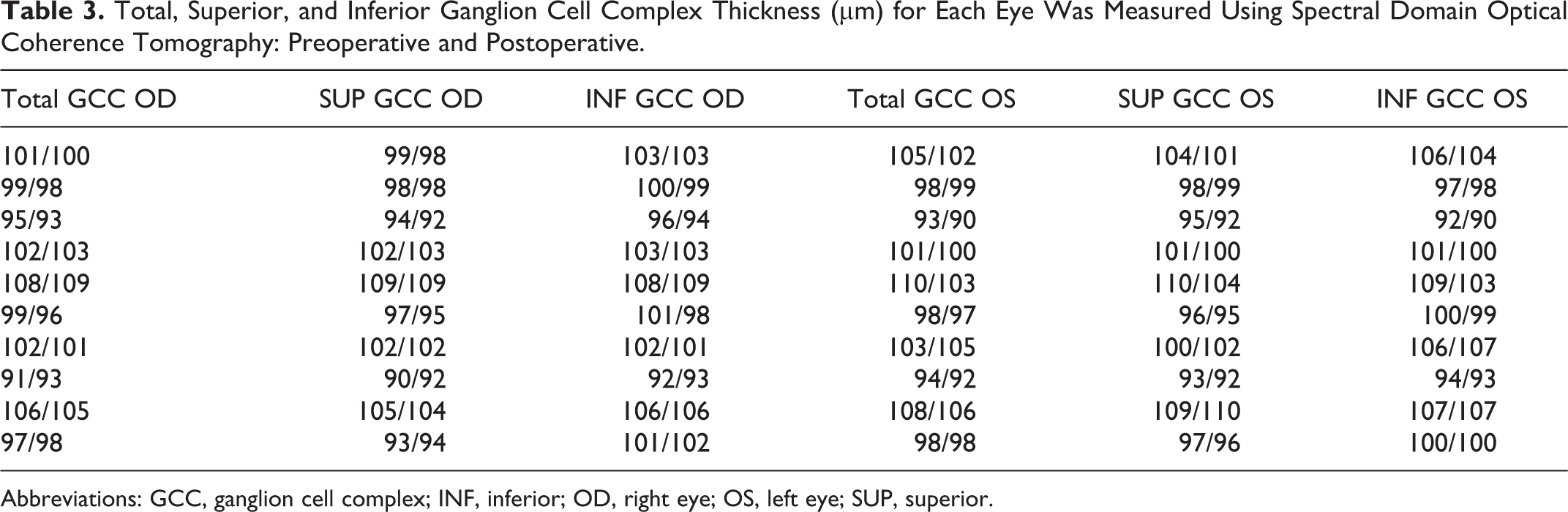
Abbreviations: GCC, ganglion cell complex; INF, inferior; OD, right eye; OS, left eye; SUP, superior.
Average, Superior, and Inferior Retinal Nerve Fiber Layer Thickness (µm) for Each Eye Was Measured Using Spectral Domain Optical Coherence Tomography: Preoperative and Postoperative.
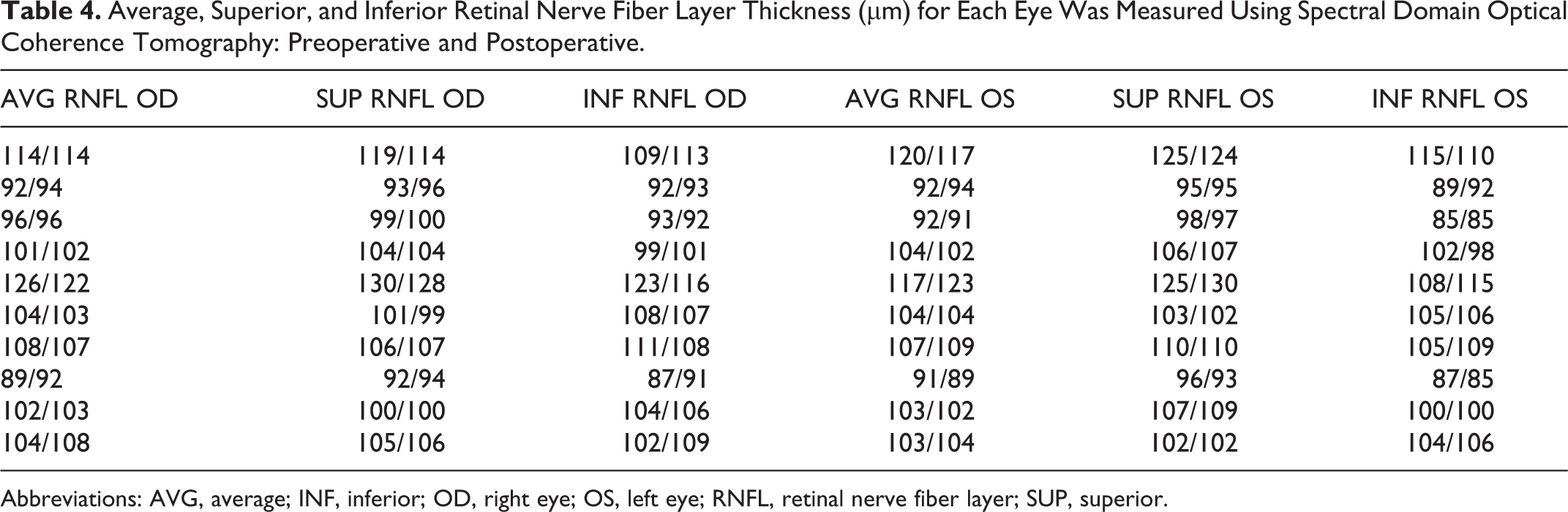
Abbreviations: AVG, average; INF, inferior; OD, right eye; OS, left eye; RNFL, retinal nerve fiber layer; SUP, superior.
Statistical Results of Average, Superior, Inferior Retinal Nerve Fiber Layer Thickness (µm), Total, Superior, Inferior Ganglion Cell Complex Thickness (µm) at Preoperative and Postoperative Period.
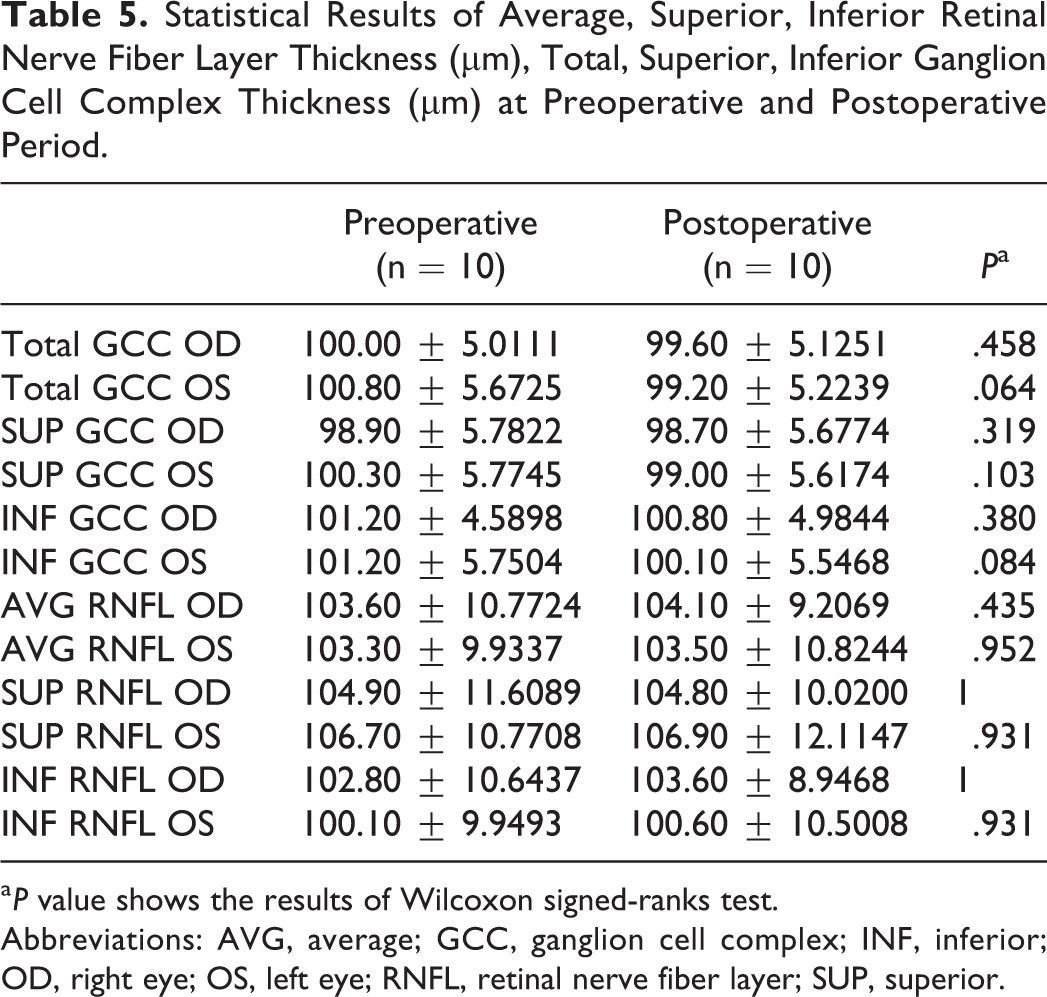
a P value shows the results of Wilcoxon signed-ranks test.
Abbreviations: AVG, average; GCC, ganglion cell complex; INF, inferior; OD, right eye; OS, left eye; RNFL, retinal nerve fiber layer; SUP, superior.
Discussion
As a result of the development of late complications resulting from nasal healing, techniques have changed from more invasive to more conservative procedures in rhinoplasty. 21,22 The intranasal continuous method and the transcutaneous perforating method were used to facilitate lateral nasal osteotomy in rhinoplasty. 23
Orbital complications of rhinoplasty vary widely from periorbital edema and ecchymosis to blindness. Lateral osteotomies can cause periorbital ecchymosis. Ecchymosis may heal in 2 to 4 weeks after surgery. 24 Ecchymosis and periorbital swelling may not be apparent instantly after surgery. Resolution of ecchymosis and periorbital swelling may take up to 2 to 3 weeks. The rate of subconjunctival ecchymosis was 19.1% in studies. Subconjunctival ecchymosis appeared unilaterally or bilaterally in the first 2 days following surgery. Subconjunctival ecchymosis disappeared in approximately 11 ± 3 days. 25 Periorbital edema and minimal ecchymosis were evident in our patients. Subconjunctival ecchymosis was seen in 2 (2%) patients, compatible with the literature. Complete resolution of subconjunctival ecchymosis took approximately 14 days in our patients. No other complications were recorded in our patients. In the literature, there was no reported association between these minor complications and IOP changes and retinal problems. This inspired us to design this study.
The causes of orbital complications occurring secondary to nasal surgery are: (1) direct mechanical trauma, (2) vascular disturbances, and (3) infectious. 14 In the literature, there are several reports about orbital–periorbital complications like necrotizing periorbital cellulitis, enophthalmos, and orbital hemorrhage. 6,26 Central retinal artery or vein occlusion, ischemic optic neuropathy, and cerebral ischemia are causes of postoperative visual loss. 14,27 -30 Retrograde flow of intra-arterial injections can cause vascular diseases. Ophthalmic artery has the anterior and posterior ethmoidal arterial branches. Nasal injections to the ophthalmic artery route can theoretically affect the ocular blood supply with pressure. 15
During lateral osteotomy, soft tissues and bone are affected by the force of the chisel. In this way, the chisel can lacerate nasal soft tissues and sometimes damage main vessels. The risk of bleeding and periorbital ecchymosis can increase because of the laceration. 31 Orbital hemorrhage following lateral osteotomies is a rare type of perioperative hemorrhage, unlike intranasal bleeding. The latter form of hemorrhage is common and can cause secondary periorbital ecchymosis anterior to the orbital structures. However, because of the confined space of the orbit, significant orbital hemorrhage can increase IOP. The increased IOP with resultant vascular compromise can result in retinal ischemia and/or optic nerve ischemia, 32,33 and increased IOP with resultant vascular compromise can lead to visual loss. 33
Intraocular pressure can be measured clinically by noncontact tonometer, applanation tonometer, and Tonopen. 34 We used Topcon noncontact tonometer CT-1P. It proved to be accurate and as reliable as the Goldmann tonometer in the assessment of IOP. 35,36
Intraocular pressure is affected from blood pressure and heart rate. Mitchell et al 37 showed that a 3 mm Hg linear IOP increase over the clinical spectrum of blood pressure level was evident. We measured the heart rate and diastolic and systolic blood pressures of the patients, 10 minutes following each IOP measurement. The IOP-related factors of heart rate, diastolic and systolic blood pressures also demonstrated no significant difference.
Optical coherence tomography was first developed in 1991. 38 Optical coherence tomography is a noninvasive imaging method that emits near-infrared light and selectively processes light reflected directly from tissues to create high resolution in vivo cross-sectional representations of anatomical structures. 39 The earliest medical uses were in ophthalmology. 40 Optical coherence tomography is used to evaluate and manage retinal disease. Optical coherence tomography is a noninvasive test and useful in the detection and quantification of macular and optic nerve head pathologies. 41 We used SD-OCT which provides excellent visualization of all retinal layers compared with previous generations of OCT devices. 42 The introduction of OCT in ophthalmology resulted in better understanding and treatment of several diseases affecting the retina and optic nerve by doctors. 38 A case was reported of central serous chorioretinopathy, whereby the patient complained of deterioration of vision in the right eye 4 days following rhinoplasty. In this case, the OCT sections through the macula depicted a mild neurosensory retinal detachment with an increase in retinal thickness equal to 245 μm. 16 In this study, we used OCT to monitor the effects of edema, minor bleeding into the orbita, and local anesthetic injections to the retina, choroid, and optic nerve. We believed OCT would be able to determine eye problems earlier than other tests. However, OCT values were within normal limits in our study and there was no difference between preoperative and postoperative values. In our cases, the IOPs, visual acuities, and OCT values were within normal limits, suggesting that ecchymosis and edema do not affect the eye directly.
Subcutaneous emphysema is a rare complication in the periorbital region. Its treatment is conservative. 8 The increased pressure can be associated with high pressure mask ventilation or with gagging or gasping during recovery. 43 It is also hypothesized that air leakage to the orbital region can lead to visual loss via compressive optic neuropathy. 44 We did not see emphysema in our patients. However, surgeons must be vigilant to prevent any visual loss as a result of emphysema.
In our study, all patients received administration of local anesthetic injections and their visual acuity remained unchanged preoperatively and postoperatively. There was no effect on visual acuity. We believe that with appropriate and careful administration of local anesthetic injections, the risk of complication is very low. In the presence of these findings, we believe that when osteotomies and local anesthetic injections are undertaken correctly, periorbital complications do not affect vision.
Conclusion
In conclusion, this study demonstrates that periorbital edema after septorhinoplasty causes no significant complications affecting IOP and visual acuity. We believe that when osteotomies and local anesthetic injections are undertaken correctly, periorbital complications do not affect vision.
Footnotes
Authors’ Note
Oğuzhan Dikici, MD, Süay Özmen, MD, and Gülçin Kazaz Dikici, MD, contributed to design, planning, data collection, intellectual review of the results, writing, and approved the final manuscript. Nuray Bayar Muluk, MD, and Çağla Çapkur Akkuzu, MD, contributed to design, planning, intellectual review of the results, writing, and approved the final manuscript. The study was approved by the Ethics Committee of Bursa Yüksek İhtisas Training and Research Hospital on March 16, 2016, no: 2011-KAEK-25 2016/05-02. All patients signed informed consent prior to participation in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.