
Abstract
Background:
As the endoscope has become more common in the otolaryngologist’s office, there is a need to reevaluate the value of traditional nasal examination methods. The objective of this study was to determine the sensitivity and specificity of traditional nasal examination tools compared to those of the rigid endoscope.
Methods:
A prospective diagnostic study was conducted. Eligible patients with nasal symptoms were recruited and examined using 4 tools: (1) a nasal speculum, (2) an otoscope, (3) a posterior rhinoscopy mirror, and (4) a rigid nasal endoscope. The diagnostic value of each tool was evaluated.
Results:
There were a total of 53 patients eligible for inclusion in the study. The mean age of all patients was 40.9 years. The most common nasal symptom was nasal obstruction (90.6%). With regard to the tools used in anterior rhinoscopy, the nasal speculum had a sensitivity of 54.69% (95% confidence interval [95% CI]: 41.75-67.18) and specificity of 88.10% (95% CI: 74.37-96.02); and the otoscope had a sensitivity of 57.81% (95% CI: 44.82-70.06) and specificity of 85.71% (95% CI: 71.46-94.57). After application of topical anesthesia and decongestant, the nasal speculum had a sensitivity of 67.19% (95% CI: 54.31-78.41) and specificity of 85.71% (95% CI: 71.46-94.57); and the otoscope had a sensitivity of 65.62% (95% CI: 52.70-77.05) and specificity of 83.33% (95% CI: 68.64-93.03). The posterior rhinoscopy mirror had a sensitivity of 12.50% (95% CI: 5.18-24.07) and specificity of 94.00% (95% CI: 83.45-98.75). All adverse events in this study were minor.
Conclusion:
The traditional nasal examination tools exhibited excellent specificity. However, the sensitivity was only average, meaning that they may not be suitable for screening. We do not recommend routine use of topical anesthesia and decongestants when applying these tools, as the application of these agents did not improve the clinical sensitivity or specificity. The posterior rhinoscopy mirror had a lowest sensitivity. We thus do not recommend using a posterior rhinoscopy mirror to rule out pathologies of the posterior nasal cavity.
Keywords
Introduction
There are various methods of examining nasal pathology including anterior rhinoscopy using a nasal speculum or otoscope, posterior rhinoscopy using a mirror, rigid nasal endoscopy, and flexible fiberoptic nasal endoscopy. The latter 2 methods are gaining in popularity and have become the gold standard for nasal examination.
Anterior rhinoscopy allows direct examination of any mid-to-anterior nasal structures. 1 The instruments traditionally used in anterior rhinoscopy are a nasal speculum and either a head light or head mirror. The otoscope, consisting of a magnifying component and a light source, has also been used in nasal examination. It is designed to illuminate and examine the depths of narrow cavities 2 and has been used to examine septum deviation in newborns. 3 –5
Posterior rhinoscopy is conducted to examine the back of the nasal cavity and nasopharynx. The instruments traditionally used in this procedure are a posterior rhinoscopy mirror and either a head light or head mirror.
However, with the exception of the otoscope, these instruments are usually not available in general hospitals, and it can be inconvenient to transfer them between departments.
Rigid nasal endoscopy 6,7 can detect nasal pathology 30% to 40% more effectively than other methods of anterior and posterior rhinoscopy. However, not all medical facilities can afford the instruments necessary to perform this procedure. 8,9
As the endoscope has become more common in the otolaryngologist’s office, there is a need to reevaluate the value of traditional nasal examination methods. To our knowledge, there is limited evidence available regarding the diagnostic value of the tools used in these procedures. The objective of this study was thus to determine the sensitivity and specificity of traditional nasal examination tools compared to those of rigid endoscopy.
Materials and Methods
Study Design and Setting
This prospective diagnostic study was conducted at Khon Kaen University’s Srinagarind Hospital in Thailand. The study period was 1 year. The inclusion criteria were presenting with nasal symptoms, being alert and able to communicate, and agreeing to participate in the study. We excluded patients who were younger than 15 years, were allergic to xylocaine or ephedrine, or had conditions that contraindicated the use of ephedrine such as hypertension, heart disease, and severe epistaxis.
The nasal cavities of eligible patients were examined via the following 6 methods: Anterior rhinoscopy using a nasal speculum, anterior rhinoscopy using an otoscope, anterior rhinoscopy using a nasal speculum after application of xylocaine and ephedrine, anterior rhinoscopy using an otoscope after application of xylocaine and ephedrine, posterior rhinoscopy using a mirror, and rigid nasal endoscopy.
Procedures
The first consultant otolaryngologist examined the patient’s nasal cavity using a nasal speculum, otoscope, and a posterior rhinoscopy mirror to examine posterior choana and nasopharynx. Then, 4% xylocaine and 3% ephedrine were sprayed into the nasal cavity. After 5 minutes, the first physician examined the patient again. Within 10 minutes, the second consultant otolaryngologist examined the patient using a 30° rigid nasal endoscope. Areas of examination included the nasal vestibule, inferior turbinate, nasal septum, nasopharynx, middle meatus, superior meatus, and sphenoethmoidal recess. The physician examined whether the patient had nasal masses/polyps, pus from the middle meatus or the sphenoethmoidal recess, or septal deviation. 10 Each physician was blinded to the other’s findings.
Outcomes
Data regarding positive signs of nasal masses, nasal polyps, and pus from the middle meatus were used to compare the diagnostic value of the traditional tools described above with that of the rigid endoscope. Anterior rhinoscopy findings included masses/polyps, pus in the middle meatus, and deviated nasal septum. Posterior rhinoscopy findings included pus in the sphenoethmoidal recess and deviated nasal septum.
Statistical Analysis
The sample size was calculated based on the expected sensitivity of 80% ± 20% and specificity of 80% ± 20%, and the significance level was .05. The sample size for this study was 53 patients.
Baseline characteristics and nasal pathologies of all patients were recorded. The diagnostic properties of the traditional nasal examination tools (with and without xylocaine and ephedrine) were calculated using rigid nasal endoscopy as the gold standard. The sensitivity and specificity were calculated with a 95% confidence interval (CI).
Ethical Considerations
This study was approved by the Khon Kaen University Ethics Committee in Human Research (HE531053). Written informed consent to participate in this study was provided by all patients enrolled.
Results
There were 53 patients eligible for enrollment in the study, 37 (69.8%) of whom were female. The mean age of all patients was 40.9 years (range 17-72 years). The most common nasal symptom was nasal obstruction (90.6%) followed by rhinorrhea (77.4%), sneezing (54.1%), and nasal itching (52.8%). The mean duration of symptoms ranged from 1 day to 30 years (average 5.9 years). There were 33 (62.3%) patients in whom rigid nasal endoscopy revealed nasal pathologies: 13 with pus from the middle meatus, 12 with nasal polyps, and 8 with pus from the sphenoethmoidal recess.
All patients underwent nasal examination of both sides of nose, making the total number of examinations 106 for each method.
Anterior Rhinoscopy Without Topical Anesthesia or Decongestants
(1) Nasal speculum
Overall, the sensitivity of the nasal speculum without topical anesthesia or decongestants was average (54.69%; 95% CI: 41.75-67.18), while the specificity was excellent (88.10%; 95% CI: 74.37-96.02), as shown in Table 1.
(2) Otoscope
Similar to the nasal speculum, the sensitivity of the otoscope without topical anesthesia or decongestants was average (57.81%; 95% CI: 44.82-70.06), while the specificity was excellent (85.71%; 95% CI: 71.46-94.57), as shown in Table 2.
Diagnostic Properties of the Nasal Speculum Without Topical Anesthesia or Decongestants.
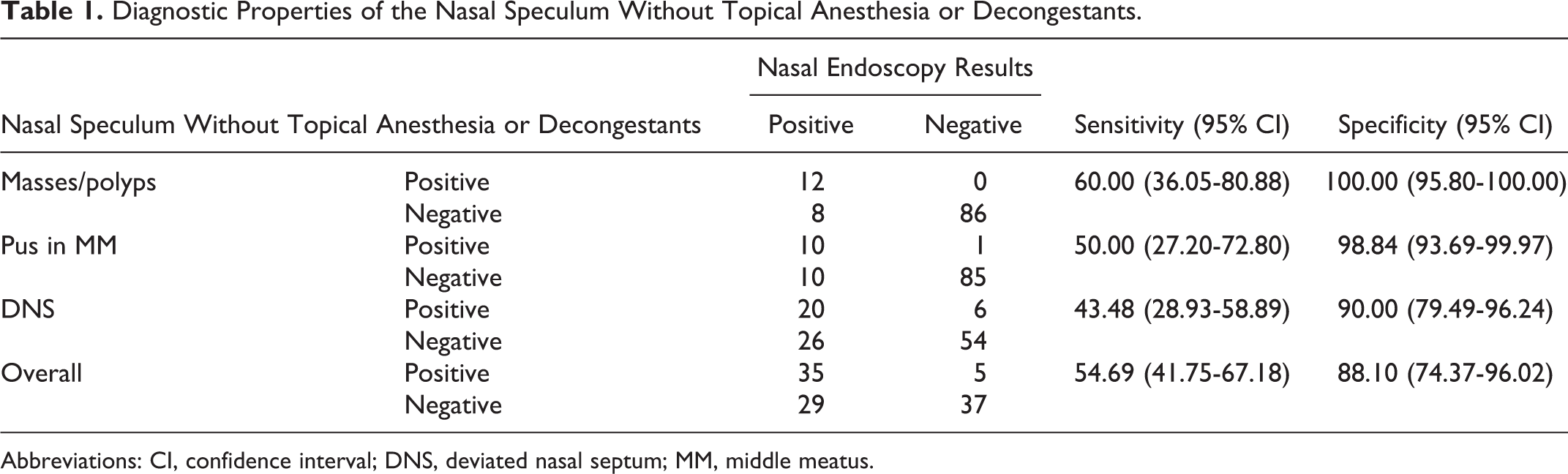
Abbreviations: CI, confidence interval; DNS, deviated nasal septum; MM, middle meatus.
Diagnostic Properties of the Otoscope Without Topical Anesthesia or Decongestants.
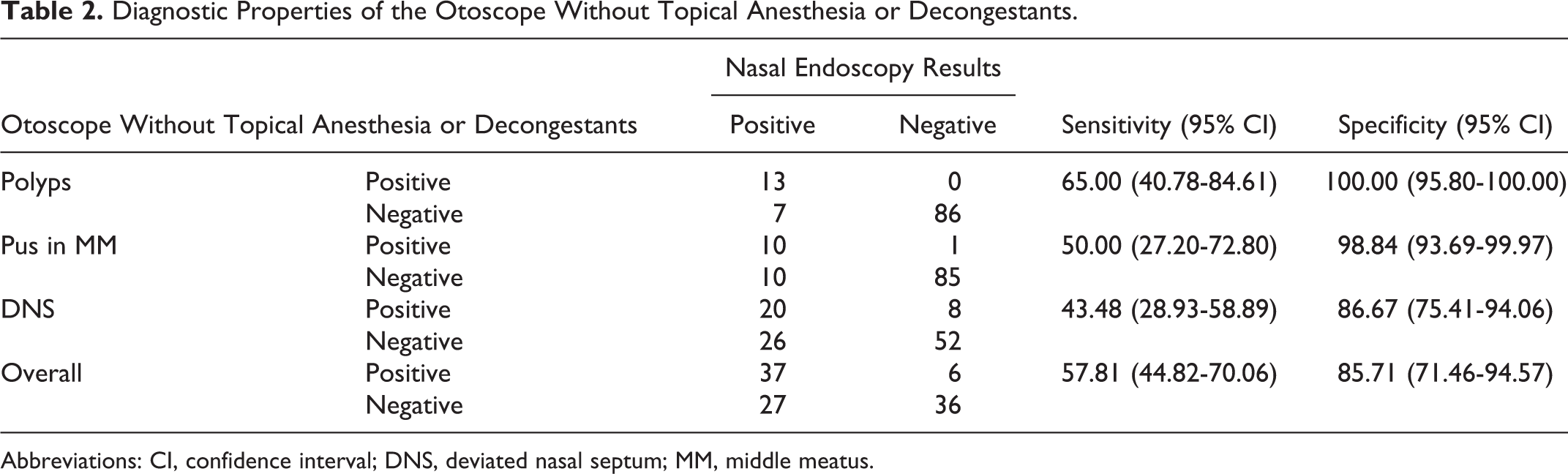
Abbreviations: CI, confidence interval; DNS, deviated nasal septum; MM, middle meatus.
Anterior Rhinoscopy With Topical Anesthesia and Decongestants
(1) Nasal speculum
After applying the topical anesthesia and decongestant, the sensitivity of the nasal speculum increased slightly to 67.19% (95% CI: 54.31-78.41). However, this improvement was not clinically significant. The overall specificity was 85.71% (95% CI: 71.46-94.57), as shown in Table 3.
(2) Otoscope
Application of xylocaine and ephedrine increased the sensitivity of the otoscope to 65.62% (95% CI: 52.70-77.05). However, this improvement was not clinically significant. The overall specificity was 83.33% (95% CI: 68.64-93.03), as shown in Table 4.
Diagnostic Properties of the Nasal Speculum With Topical Anesthesia and Decongestants.
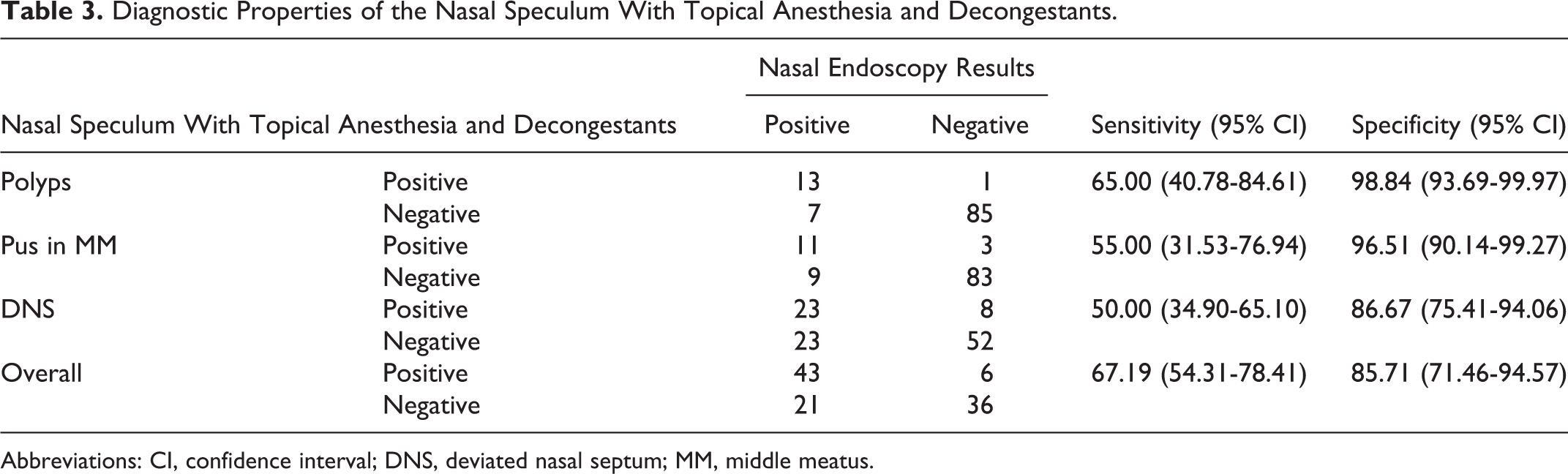
Abbreviations: CI, confidence interval; DNS, deviated nasal septum; MM, middle meatus.
Diagnostic Properties of the Otoscope With Topical Anesthesia and Decongestants.
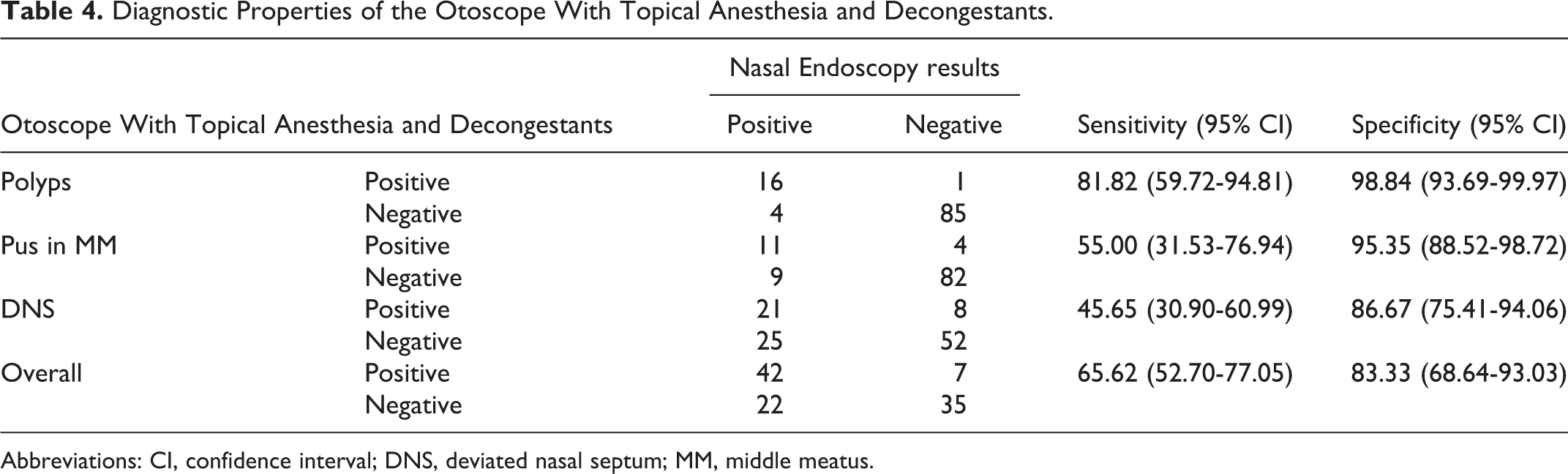
Abbreviations: CI, confidence interval; DNS, deviated nasal septum; MM, middle meatus.
Posterior Rhinoscopy
The overall sensitivity of posterior rhinoscopy using a mirror was 12.50% (95% CI: 5.18-24.07), and the specificity was 94.00% (95% CI: 83.45-98.75; Table 5).
Diagnostic Properties of the Posterior Rhinoscopy Mirror.
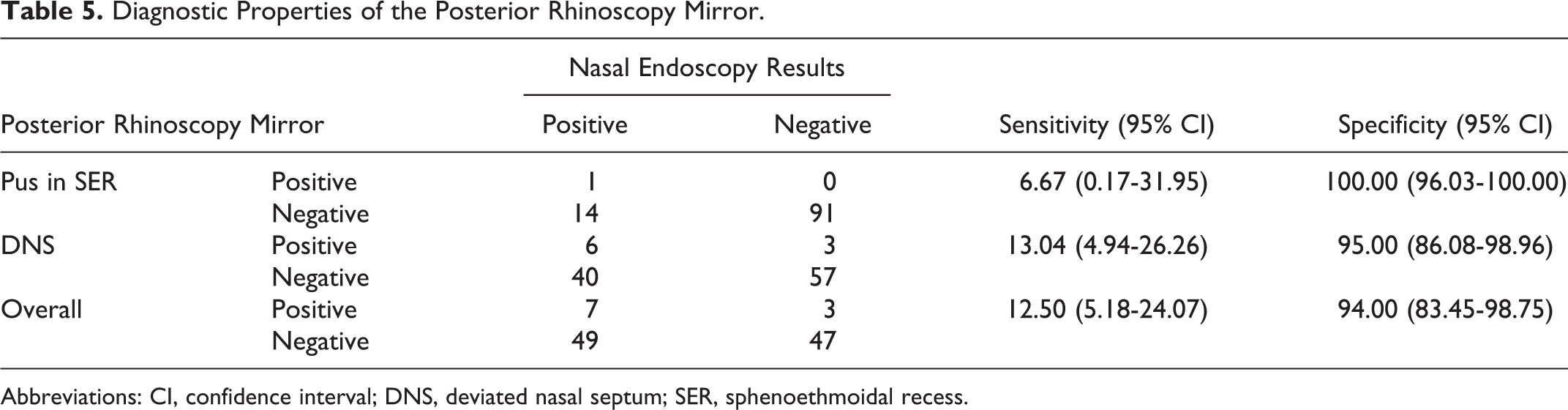
Abbreviations: CI, confidence interval; DNS, deviated nasal septum; SER, sphenoethmoidal recess.
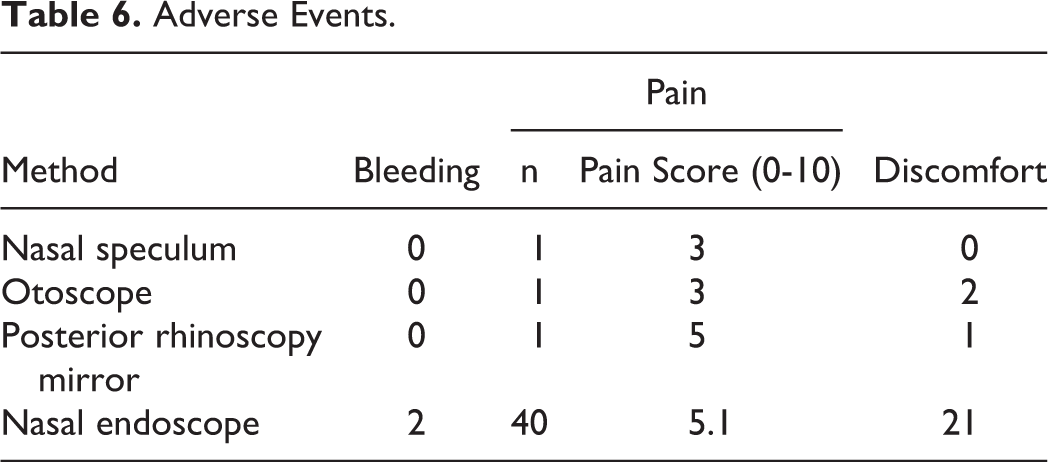
Adverse Events
Use of the nasal speculum, otoscope, and posterior rhinoscopy mirror resulted in fewer complications compared to the nasal endoscope. One patient complained of pain from the nasal speculum, otoscope, and posterior rhinoscopy mirror, with pain scores of 3, 3, and 5, respectively (range 0-10). Nasal endoscopy caused pain in 40 (75.5%) patients (with an average pain score of 5.1), minor bleeding in 2 (3.8%) patients, and discomfort in 21 (39.6%) patients (Table 6).
Adverse Events.
Discussion
Nasal symptoms, such as rhinorrhea and itchy nose, are common presenting symptoms in clinical practice and may have various causes including allergic rhinitis, sinusitis, or nasal polyps. 11,12 Treatment for nasal symptoms is usually effective if the causes are correctly identified.
According to 2013 survey of otolaryngologists, all respondents had regularly performed anterior rhinoscopy, while only 30% of otolaryngologists had used an endoscope. There were no data on posterior rhinoscopy in this survey. The author concluded that anterior rhinoscopy and endoscopy are important components of nasal examination. 1
Levine compared anterior and posterior rhinoscopy with rigid nasal endoscopy. Nasal endoscopy found nasal pathologies that had not been diagnosed by traditional examination in 58 (38.7%) patients. The pathologies found included obstructed natural maxillary sinus ostia and several pathologic disorders in the middle meatus such as polyps and synechiae. 9
Benninger compared the diagnoses made using traditional tools with those made using an endoscope and found that nasal endoscopy played a role in diagnosis in 11% of patients, although in no case did endoscopy change the diagnosis or treatment plan. Endoscopy allowed visualization past an enlarged turbinate or septal deviation in 6 patients, confirmed a suspected diagnosis in 3 by visualization of the middle meatus, and detected the site of a large choanal polyp in 1. In 1 case, endoscopy identified a paradoxical turbinate on the side opposite the symptoms and radiological findings. 13
To our knowledge, there has been no study conducted to evaluate the diagnostic value of traditional nasal examination tools compared to that of the nasal endoscope. As the nasal endoscope is gaining in popularity and its cost has decreased, there was a need to reevaluate whether these traditional tools were still necessary.
The nasal speculum and otoscope were comparable in terms of sensitivity and specificity when used in anterior nasal rhinoscopy. The nasal speculum had a sensitivity of 54.69% (95% CI: 41.75-67.18) and specificity of 88.10% (95% CI: 74.37-96.02), and the otoscope had a sensitivity of 57.81% (95% CI: 44.82-70.06) and specificity of 85.71% (95% CI: 71.46-94.57). Adding topical anesthesia and decongestants did not significantly improve the sensitivity and specificity. After their application, the nasal speculum had a sensitivity of 67.19% (95% CI: 54.31-78.41) and specificity of 85.71% (95% CI: 71.46-94.57). The otoscope had a sensitivity of 65.62% (95% CI: 52.70-77.05) and specificity of 83.33% (95% CI: 68.64-93.03).
The posterior rhinoscopy mirror had the lowest sensitivity at 12.50% (95% CI: 5.18-24.07). We do not recommend using a posterior rhinoscopy mirror alone to rule out pathology of the posterior nasal cavity.
Based on these findings, we recommend either a rigid or flexible endoscope as the primary tool for nasal examination in an ear, nose and throat office setting, as the cost of these tools have decreased. Although the nasal speculum and otoscope had the same diagnostic value for anterior nasal examination, we recommend the otoscope, as it can be used for ear examination as well. The posterior rhinoscopy mirror may not be necessary.
Conclusion
The traditional nasal examination tools exhibited excellent specificity. However, the sensitivity was average, indicating that they may not suitable for screening. We do not recommend routine use of topical anesthesia and decongestants, as the application of these agents did not improve the clinical sensitivity or specificity of the traditional tools. The posterior rhinoscopy mirror had the lowest sensitivity. We thus do not recommend its use in ruling out pathologies of the posterior nasal cavity.
Footnotes
Acknowledgments
The authors would like to thank all of the patients who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.