
Abstract

A 67-year-old woman with a history of type 2 diabetes was referred to our hospital and reported painful swelling on the left neck over a 2-week period. She had visited another hospital where she was administered oral antibiotics, but her symptoms deteriorated. Her temperature, pulse, and blood pressure were 35.3°C, 107 bpm, and 92/50 mm Hg, respectively. During physical examination, bruising, tenderness, and severe swelling of the left neck were noted (Figure 1A). Laboratory data revealed the following: a white blood count of 11 340/µL, a hemoglobin level of 10.3 g/dL, a creatinine level of 1.9 mg/dL, a blood sugar level of 696 mg/dL, and a C-reactive protein level of 31.09 mg/dL. Computed tomography of the neck without contrast revealed a large lesion with air bubbles and sternocleidomastoid muscle infiltration on the left neck (Figure 1B and C). Deep neck infection with necrotizing fasciitis was impressed, and emergent incision and drainage with fasciotomy was performed in the operation room and revealed a substantial amount of pus, necrotic fascia, and necrosis of the sternocleidomastoid muscle (Figure 1D). Pathology was proven to be necrotizing inflammation, and the pus culture confirmed the presence of Klebsiella pneumoniae. During her hospitalization, antibiotics with intravenous vancomycin and ceftazidime were prescribed and multiple debridement procedures were performed (Figure 1E). After 2 weeks of treatment, delayed primary suture was performed, and the patient was discharged. Augmentin was prescribed for 2 weeks, and the patient had an uneventful recovery (Figure 1F).
Necrotizing fasciitis is an infection of deep soft tissues that results in progressive destruction of the muscle fascia and overlying subcutaneous fat. 1 Necrotizing fasciitis of the neck constitutes an aggressive form of deep neck infection that is associated with a high mortality rate. 2 Treatment for this condition requires critical medical and surgical intervention. Necrotizing fasciitis of the head and neck can result from a breach in oropharynx mucous membrane integrity following surgery or instrumentation and can develop in cases of odontogenic infection. 3 Suspicion of this rare critical entity is necessary for treating patients with type 2 diabetes or those with immunocompromised conditions. The physician should secure the airway, perform repeated debridement, and proceed with reconstruction after the wound has been cleared. 2
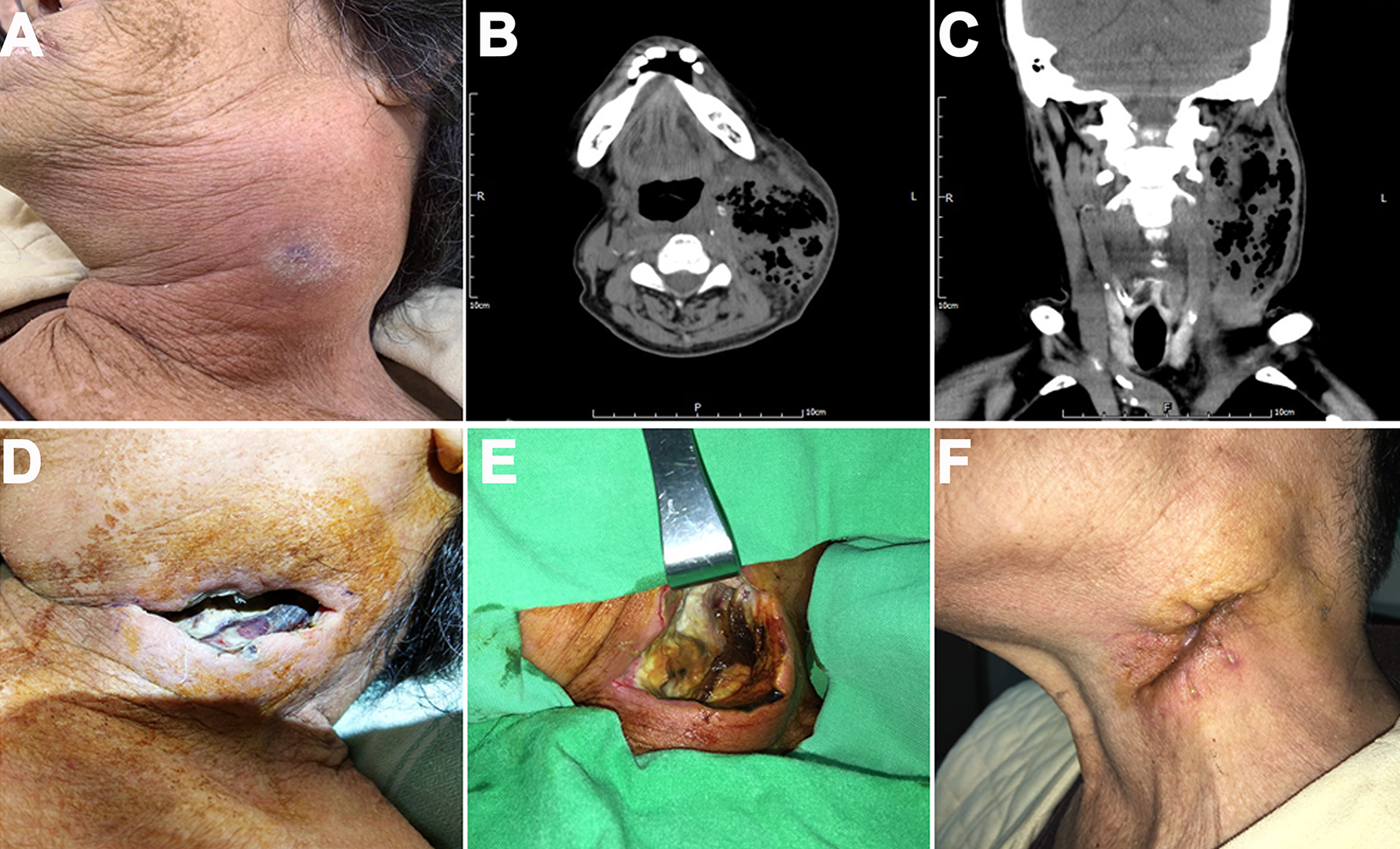
A, A bruising lesion in the central part of the diffuse reddish swelling in the left neck was noted. B and C, Respective axial and coronal view of computed tomography scan without contrast revealed a large lesion with air bubbles and sternocleidomastoid muscle infiltration of the left neck. D, Wound wet dressing was changed on postoperative day 1. E, The wound with necrotic tissue and muscle were showed before debridement on postoperative day 3. F, The wound was uneventful after 5-week follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-C108-037 to H. C. Chen).