
Abstract

By definition, the subglottis is the area of the larynx immediately below the vocal folds extending to the level of the inferior border of the cricoid cartilage. This area represents the narrowest portion of the pediatric airway and is the most common site of iatrogenic stenosis. This stenosis is generally secondary to increased rates of intubation in infants of prematurity. 1 Evaluation and treatment for subglottic stenosis represents one of the most common airway consultations within pediatric otolaryngology. Goals of therapy include securing a safe airway and restoring subglottic patency. 1 In this clinical case, we present a unique pattern and presentation of subglottic stenosis requiring urgent tracheostomy.
A 16-day-old (ex-37-week-old) male infant with no significant past medical history presented to the emergency department of a tertiary care pediatric hospital with respiratory failure including tachypnea, fevers, and subcostal/suprasternal retractions. He was transferred to the pediatric intensive care unit and placed on bilevel positive airway. However, his respiratory status declined, and he was intubated with a 3.0 cuffed endotracheal tube the same day of admission. Shortly thereafter, he was diagnosed with rhinovirus bronchiolitis and later found to have methicillin-sensitive Staphylococcus aureus tracheitis on hospital day (HD) 6. He was extubated on HD 11 to continuous positive airway pressure. His postoperative course was complicated by complete left lung atelectasis on HD 12, but he was weaned to room air on HD 20 and was transferred to the medical floor. The next day he was noted to have intermittent, mild stridor with feeds and poor oral intake. He did not have noisy breathing or respiratory distress at rest. On HD 21, bedside flexible laryngoscopy demonstrated normal airway above the vocal folds, while suboptimal subglottic visualization demonstrated mild narrowing. His weight fluctuated as did the intermittent stridor with oral feeds; however, he remained stable on room air over the next 2 weeks. Airway evaluation in the operating room was deferred until 4 to 6 weeks from initial presentation to decrease airway reactivity contributed by viral infection.
On HD 35, he was taken to the operating room for flexible laryngobronchoscopy with mask ventilation. This revealed a thick horizontal scar band in the subglottis diving the airway into the anterior and posterior subglottic webs, each with 1- to 2-mm lumens (Figures 1 and 2). The patient was diagnosed with grade III subglottic stenosis, and an urgent tracheotomy was performed over a laryngeal mask airway. On postoperative day (POD) 7, he underwent cold knife subglottic scar division, balloon dilatation, and steroid injection. On POD 21, he underwent a second airway evaluation showing resolution of the subglottic scar and a 10% subglottic narrowing. No subglottic intervention was performed; however, suprastomal granulation was excised with an airway shaver. He was quickly weaned to tracheotomy collar and discharged on HD 77 to a long-term care facility. Approximately, 3 months after the original procedure, the airway was evaluated with flexible laryngobronchoscopy, which reveal resolution of subglottic stenosis (Figure 3).

Subglottic stenosis appreciated from the level of the hypopharynx.

Thick horizontal scar band in the subglottis dividing the airway into the anterior and posterior subglottic webs, each with 1- to 2-mm lumens.
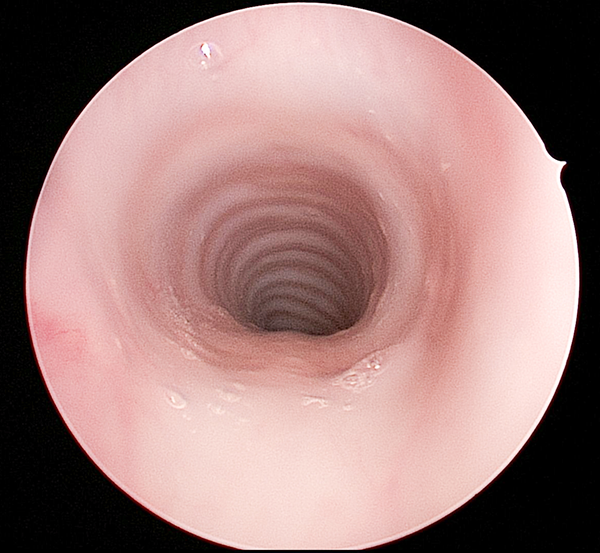
Subglottic area approximately 3 months after the original procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.