
Abstract

A 44-year-old man was previously healthy. He developed right cheek paresthesia and swelling for months without obvious progression in size. On palpation, the nontender mass seemed to be multifocal with extension to right parotid, submandibular, and buccal area. The buccal mucosa was grossly smooth and there’s no palpable lymph node along the neck.
Posterior anterior mandible view demonstrated an osteolytic lesion involving right posterior body of the mandible (Figure 1). Computer tomography (CT scan) of oropharynx (Figure 2), with and without contrast, revealed a 7-cm, cystic, and expansile lesion in right mandible with loculated margin with faint peripheral enhancement and compression of right submandibular gland. It is suspicious for a benign or malignant odontogenic tumor. There is also a cystic lesion, measuring 5.5 cm in greatest dimension, at right parapharyngeal space, with tight connection to the right mandibular lesion. The evidence of compression of the right carotid space by the cystic lesion is also noted. Technetium-99m-diphosphonates whole-body bone scan showed moderately increased uptake in the right mandible, reflecting the existing lesion as noticed in CT scan. Incisional biopsy of the mandibular mass reported chronic inflammation with an increased spindle cell in focal area.
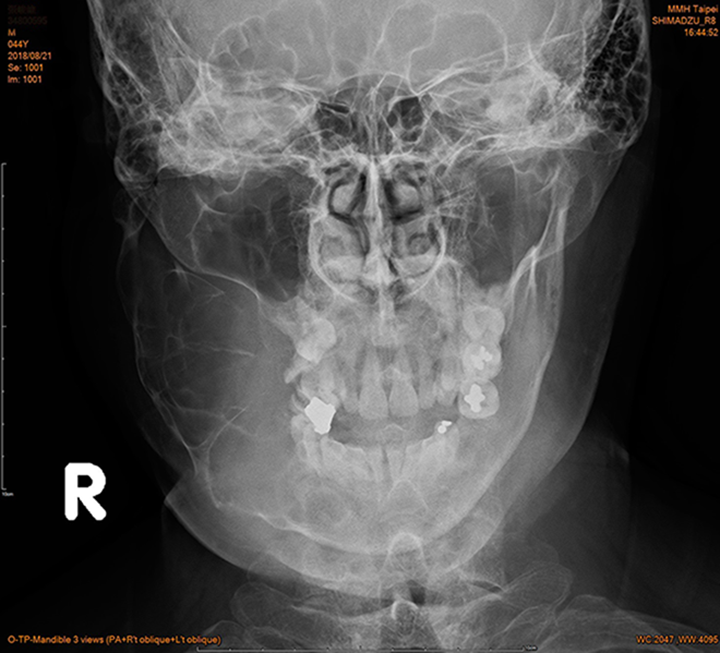
Mandible Posterior-Anterior view—loculated and osteolytic lesion in right mandible.
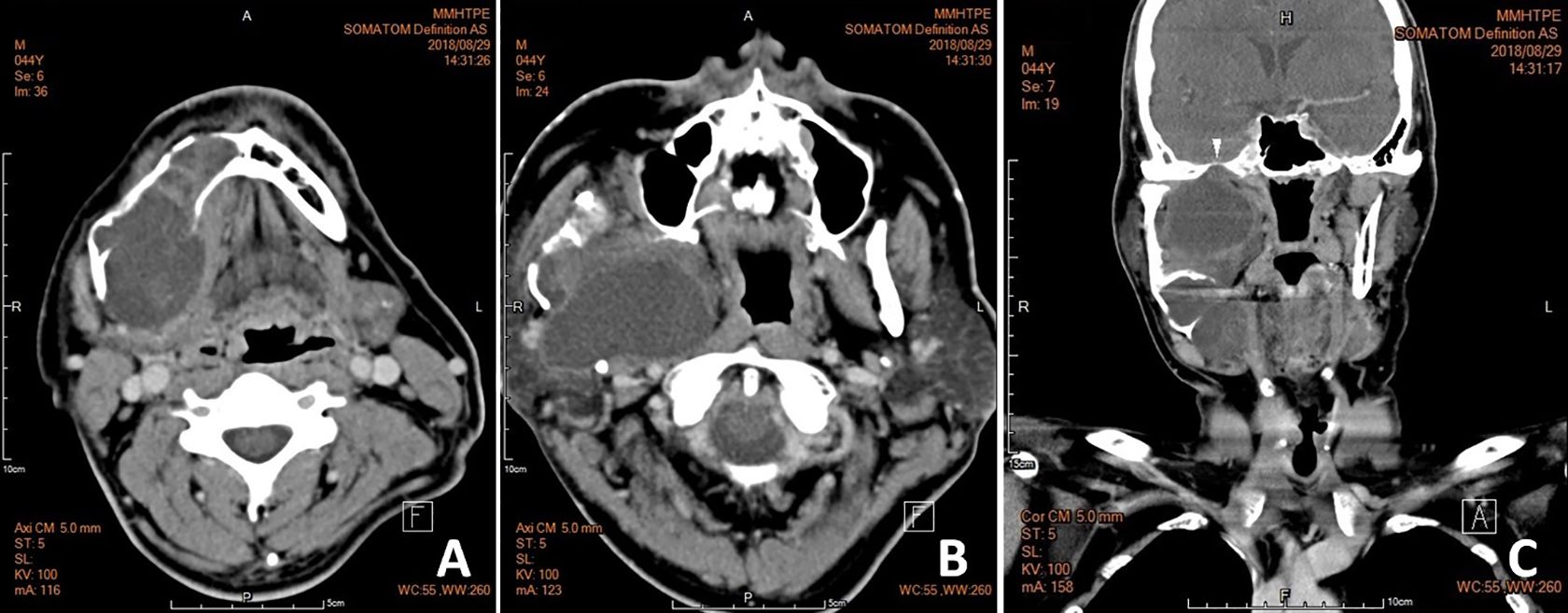
Computer tomography of oropharynx: A, A 7-cm, cystic, and expansile lesion in right mandible with loculated margin, faint peripheral enhancement, and compression of right submandibular gland. B, A right parapharyngeal cystic lesion, measuring 5.5 cm in greatest dimension, with tight connection to the mandibular lesion. C, Widened foramen ovale (arrow head).
En bloc excision of the right mandibular and right parapharyngeal mass, as well as dissection of surrounding submandibular lymph nodes, were performed. Mandibular reconstruction with fibular free flap was then carried out by oral surgeon and plastic surgeon (Figure 3). Microscopically, it shows the presence of streaming fascicles of spindle-shaped cells arranged in a well-organized pattern in focal areas, consistent with Antoni A tissue with adjacent myxoid, and less-organized Antoni B tissue. The spindle cells are further highlighted by immunostaining with S-100 protein. The evidence of cystic change, hemosiderin deposition, and an infiltrate of foamy histiocytes is also noted (Figure 4). The above pictures support the diagnosis of an ancient schwannoma. The dissected lymph nodes showed lymphoid hyperplasia.

Mandibular reconstruction with fibular free flap was performed following en bloc excision of the right mandible and parapharyngeal tumor.
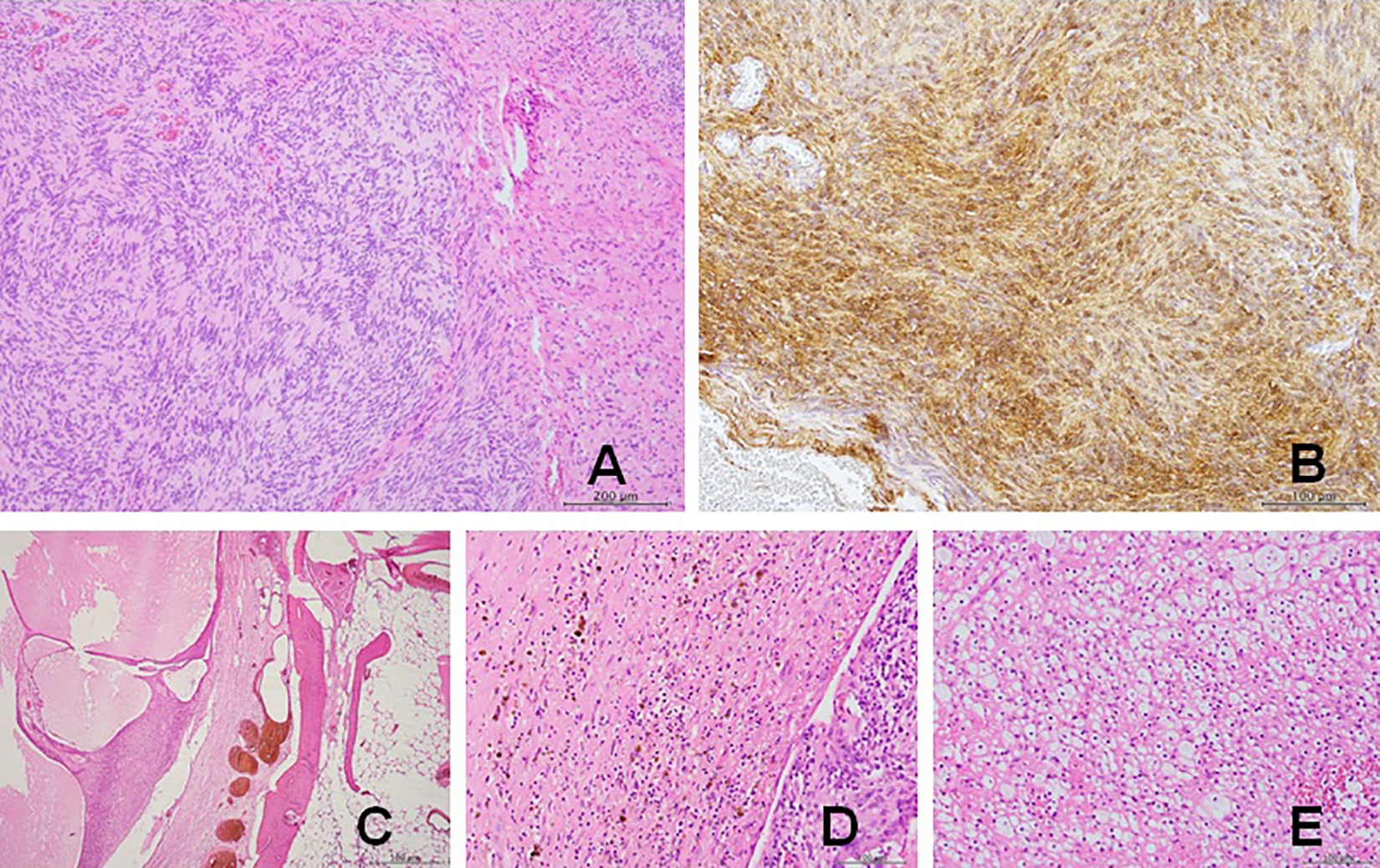
Pathological findings under microscopy: A, The presence of Antoni A tissue and Antoni B tissue (×100), (B) diffuse positive immunostaining with S-100 protein (×200), (C) evidence of cystic change (×40), (D) hemosiderin deposition (×200), (E) increased infiltrate of foamy histiocytes (×200).
On 6-month follow-up after surgery, the patient still felt right mandibular pain occasionally. Oral intake was fair on soft diet then. We arranged swallowing rehabilitation for the patient.
Schwannomas are indolent, benign neoplasms derived from Schwann cells. 1 The clinical presentations are mainly affected by tumor size, surrounding structures, and the nerve of origin (NOO). In extracranial head and neck schwannomas, sympathetic trunk and the vagus nerve are the common NOOs. 2 However, less than 20% of the patients had neurogenic symptoms or signs. 3 Our patient did not have symptoms of paresthesia of the right face until the tumor had increased to a huge size, causing prominent swelling of mandible region.
Trigeminal schwannomas may arise from the trigeminal nerve root, Gasserian ganglion, or 1 of the 3 peripheral branches of the trigeminal nerve. 4 Sun et al reported 2 rare cases of intraosseous mandibular schwannoma, originating from the trigeminal nerve, with intracranial extension along the mandibular nerve. 5 The CT scan of our patient also demonstrates widen foramen ovale when compared to contralateral side, without obvious intracranial invasion could be identified (Figure 2).
There are several diagnostic tools of schwannoma, but histopathology remains the gold standard. 6 The specificity of fine-needle aspiration cytology 7 and imaging 4 studies in making the diagnosis of schwannoma was around 25% and 38%, respectively. Magnetic resonance imaging had been reported as high as 80% diagnostic rate in schwannomas, featured by low signal intensity in T1-weighted images and high signal intensity in T2-weighted images. 8 In our case, degenerative change in ancient schwannoma and a relatively small specimen from incisional biopsy of a huge lesion raise the difficulty in the preoperative diagnosis.
Although tumor excision is the treatment of choice in cases of schwannoma, both the severity of preoperative symptomatology and the anticipated postoperative neurological deficit should be taken into consideration. 8 The size of the tumor, its location, its surrounding structures, and the suspicion of malignancy have great influence on the achievement of total or subtotal excision. The surgical technique of intracapsular excision with gentle dissection between the tumor capsule and normal fascicles minimizes the risk of nerve damage. For extensive schwannomas, nerve sacrifice with reconstruction and rehabilitation is important considerations. 7
With involvement of the mandible and parapharyngeal space, the operation of right hemimandibulectomy and the excision of parapharyngeal tumor were performed in our patient, followed by mandible reconstruction with fibular free flap. The 6-month follow-up of the surgical outcome was satisfying. Swallow rehabilitation program was conducted for improving oral intake and jaw motion. The need of long-term follow-up was controversial. Recurrence is rare and mostly developed in cases with intracranial involvement. 4,7,9
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.