
Abstract
Aims:
Many procedures in ear, nose, and throat (ENT) day surgery are carried out under local anesthesia in Finland, whereas many other countries use general anesthesia. We investigated overstay and readmission rates in local and general anesthesia at Helsinki University Hospital.
Material and Methods:
We conducted a retrospective study on ENT (n = 1011) day surgery patients within a 3-month period using the hospital’s surgery database to collect data pertaining to anesthesia, overstays, readmissions, and contacts within 30 days of surgery.
Objectives:
We examined the effect of American Society of Anesthesiologists (ASA) class, age, sex, type of procedure, and anesthesia type on overstay, contact, and readmission rates.
Results:
A multivariable logistic regression model included ASA class, age, sex, type of procedure, and anesthesia (local vs general). Sex, age, and type of procedure had an effect on the outcomes of overstay, readmission, or contact. With general anesthesia, 3.2% (n = 23) had an overstay or readmission compared to 1.4% (n = 4) after local anesthesia. This was mainly explained by the number of study outcomes in tonsillar surgery that was performed only in general anesthesia.
Conclusions:
Day surgery could be done safely using local anesthesia, as the number of study outcomes was no greater than in general anesthesia. Sex, type of procedure, and age affected the rate of study outcomes, but ASA class and anesthesia form did not. Our overstay, contact, and readmission rates are on the same level, or lower, than in international studies.
Introduction
As surgical techniques improve, more and more procedures are carried out as day cases. As of 2011, day surgery procedures composed 63% of all surgery in the Helsinki and Uusimaa Hospital District, totaling 34 490 procedures of which 25 228 were performed at Helsinki University Hospital. 1 Ear, nose, and throat (ENT) surgery comprises up to 28% of all day surgery in Finland and is the second most common day surgery specialty. 2 In some countries, however, some procedures deemed safe for day surgery are still performed as inpatient surgery, for example, tonsillectomies in Austria. 3 It has been stipulated that procedures should be performed as day surgery only when readmissions remain below 2% to 4%. 4 An audit by the Royal College of Surgeons of England showed an average readmission rate of 2.8% after ENT day surgery, with vomiting, hemorrhage, and inadequate recovery from anesthesia composing 72% of readmissions. 5 A study in the United States showed a 30-day readmission rate of 2.0% for ENT outpatient surgery. 6 Readmission after pediatric day surgery is increased in children less than 2 years of age as well as those undergoing ENT surgery. 7
We set out to investigate the overstay, readmission, and contact rates for ENT day surgery in Helsinki University Hospital. The majority of these procedures are performed under local anesthesia in Finland, as opposed to many other countries, where general anesthesia is used. We set out to examine whether the broad use of local anesthesia affected overstay, contact, and readmission rates. The ENT specialty was chosen due to the volume of procedures and their representation of a large part of day surgery procedures in Finland.
Definitions
We defined an overstay as a patient not being discharged after the procedure as planned from the day surgery unit but rather requiring treatment on the ward. A contact is defined as a patient returning to hospital after discharge but not requiring treatment on the ward and a readmission as one who does. In the contact group, we have also included phone calls to the emergency department or outpatient clinic in regard to problems connected to the day surgery procedure in question.
Patients and Methods
Study Design
We conducted a retrospective study on all ENT day surgery patients with a procedure performed between January 1, 2015, and March 31, 2015, at Helsinki University Hospital. We extracted these patients from the surgery database of the hospital (GE Healthcare Centricity Opera OR Management Software), which is a register containing all procedures performed in the Helsinki and Uusimaa Hospital District. The procedures are classified according to the Nordic Medico-Statistical Committee (NOMESCO) Classification of Surgical Procedures. 8 Patients’ personal information, date, time, surgeon, assisting surgeon, and surgical specialty, among other pre-, intra-, and postoperative data were collected. The 15 most common procedures were then chosen for ENT specialty using NOMESCO procedural codes and by grouping similar procedures (Table 1). The procedures were then divided into subgroups based on the type of procedure: ear surgery, nasal surgery, tonsil and adenoid surgery, or miscellaneous.
Table of Day Surgery Procedures.
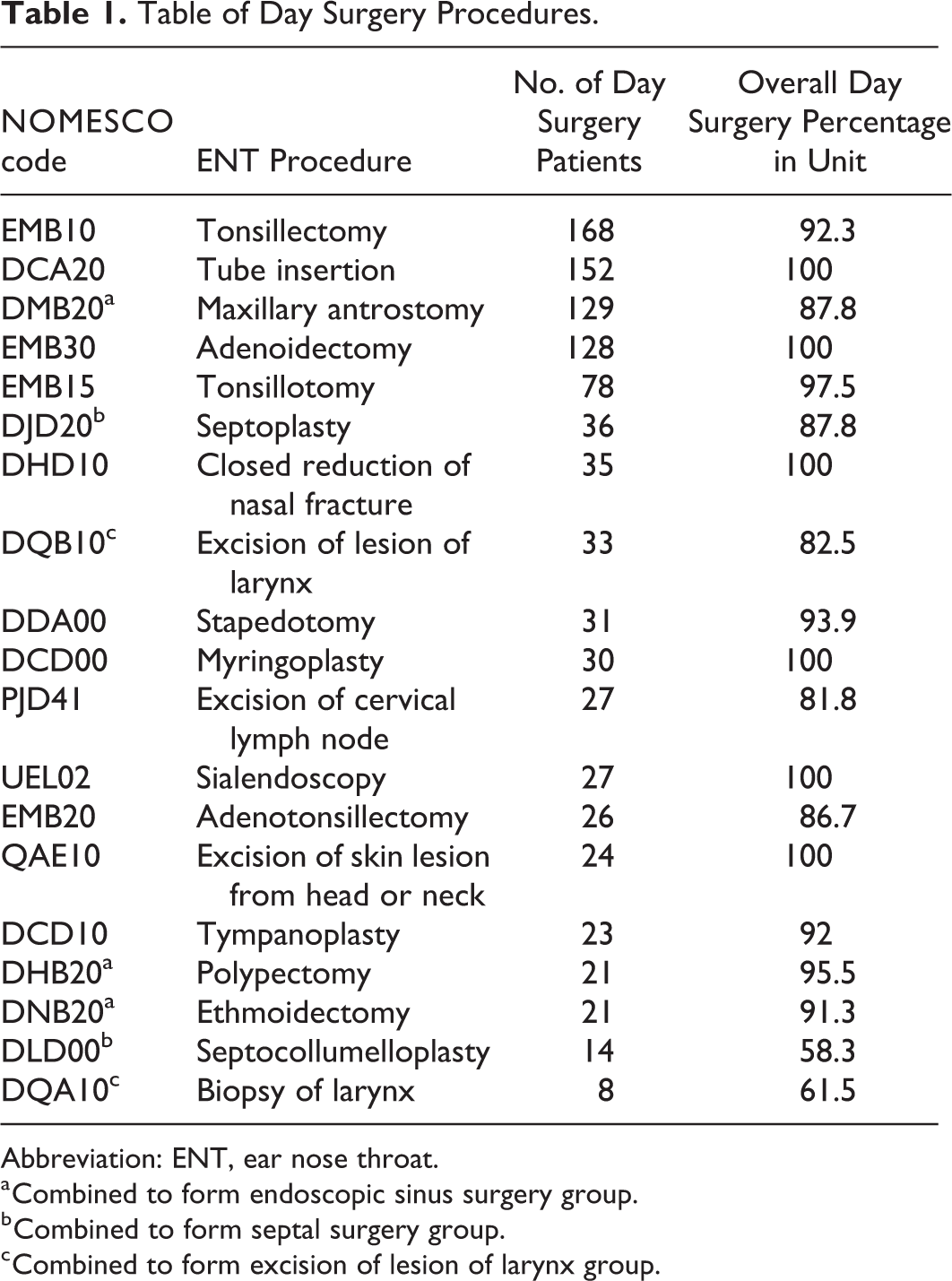
Abbreviation: ENT, ear nose throat.
a Combined to form endoscopic sinus surgery group.
b Combined to form septal surgery group.
c Combined to form excision of lesion of larynx group.
According to national law, this study did not require ethics committee approval, as this was a registry study with no patient intervention involved. However, we applied for and received permission from the Research Administration of the Hospital District for this study. The results of this study are reported according to STROBE guidelines.
Participants
Only those who were planned as day surgery patients during the preoperative visit were included in the study. Day surgery criteria of our clinic conform to international day surgery standards. 9 We collected data on age, sex, type of procedure, and American Society of Anesthesiologists (ASA) class for these day surgery patients (Table 2) and reviewed hospital records for information pertaining to overstays, readmissions, and contacts within 30 days of day surgery.
Patient Demographics in 1011 Day Surgery Procedures.
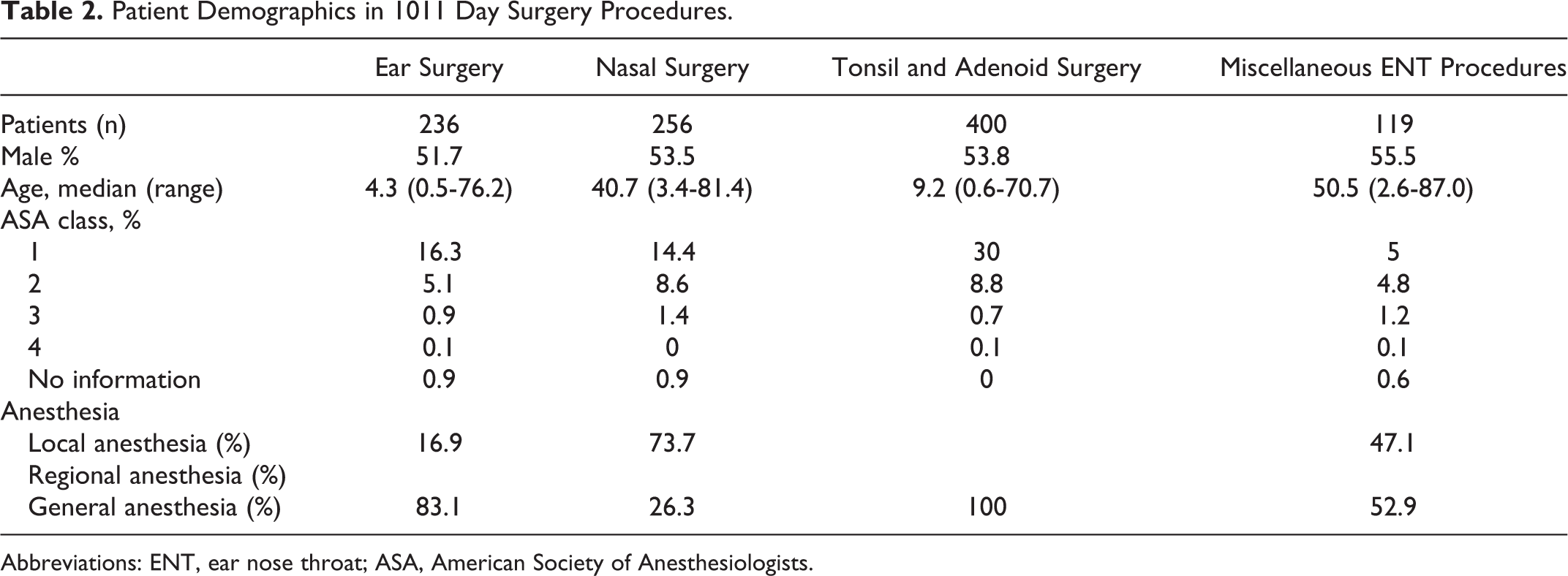
Abbreviations: ENT, ear nose throat; ASA, American Society of Anesthesiologists.
Those undergoing one of the procedures mentioned in Table 1, but deemed unfit for day surgery when surgery was scheduled, were removed from the study. Anesthesia, the surgical procedure, as well as pain, and postoperative nausea and vomiting prophylaxis and management were carried out according to the protocol of the clinic. Local anesthesia was used whenever possible from a medical point of view, whereas patients were offered the option to opt out of local anesthesia and receive general anesthesia upon request. Some procedures, for example, tonsil surgery, were always performed under general anesthesia due to the nature of the surgery.
Statistical Analysis
Data are described with numbers and percentages. The effects of ASA class (1, 2, 3, and 4), age class (0-15, 16-44, 45-64, and 65 or older), sex, procedure category, and form of anesthesia on the outcome of overstay, readmission, or contact were analyzed with univariable and multivariable logistic regression. Results are expressed using unadjusted and adjusted odds ratios (OR) with 95% confidence intervals (CIs). P values <.05 were considered as statistically significant. Statistical analysis was done using IBM SPSS Statistics version 22.0 (IBM Corp, Armonk, New York; RRID: SCR_002865).
Results
A total of 1011 ENT patients underwent day surgery during the 3-month period. Of the procedures included, the majority was performed as day surgery in our clinic (Table 1). Twenty overstays occurred among ENT patients, with nausea or vomiting (n = 8) and operation site bleeding (n = 5) being the most common causes for overstay overall. Other reasons included fatigue (n = 2), more extensive surgery than originally planned (n = 2), pain (n = 1), dizziness (n = 1), and slow recovery from anesthesia (n = 1).
One hundred sixteen ENT patients contacted the hospital 149 times for varying causes, with the most common being operation site bleeding (n = 39), pain (n = 25) and pressure, swelling, or nasal stuffiness (n = 14).
A total of 14 readmissions of 13 ENT patients were recorded during the 30-day postoperative period. The most common reasons for readmission overall were operation site bleeding (n = 3), dizziness (n = 3), and seizures (n = 3), with 1 patient each having obstructive bronchitis, pulmonary empyema, pneumonia, unspecified bacterial infection, and acute kidney failure leading to dialysis with aspiration pneumonia and sepsis.
Of general anesthesia patients, 3.2% (n = 23) had an overstay or readmission compared to 1.4% (n = 4) of local anesthesia patients. Two procedures did not involve any contacts, overstays, or readmissions: septocollumeloplasty (n = 14) and biopsy of the larynx (n = 8). No patients died during the follow-up period.
In our data, the overall readmission rate was 1.4%, overstay rate 2.0%, and contact rate 14.7%. Overall, 138 patients had an outcome of some kind. The majority of phone contacts were for suspected infections, the prescribing of an antibiotic, or renewal of prescriptions, for example, for pain medication.
The results of logistic regression are presented in Table 3. In univariable analysis, the age-group of 16 to 44 years was associated with the highest risk of an overstay, readmission, or contact (<.001), while the ASA class (P = .185) and the form of anesthesia (P = .344) were not significant predictors. Sex did affect the outcome significantly, with 17.3% of females having an overstay, readmission, or contact and only 10.5% of males (P = .002). Type of procedure did not have a significant effect on study outcomes (χ2 test P = .173). Using a multivariable logistic regression model including ASA class, age, sex, type of procedure, and form of anesthesia, ASA class and form of anesthesia did not predict overstay, readmission, or contact. Age (P = .000) and sex (P = .028) remain significant predictors in the multivariable analysis. The odds of an outcome were higher in the age groups of 16 to 44 and 45 to 64 years than in other age groups. Females had 53% greater odds of an outcome than males (adjusted OR: 1.53, 95% confidence interval [CI]: 1.05-2.24, P = .028). Of procedure categories, tonsil and adenoid surgery was a significant risk for an outcome (adjusted OR: 2.61, 95% CI: 1.22-5.62, P = .014).
The Associations of Factors With an Outcome (Overstay, Readmission, or Contact) by Univariable and Multivariable Logistic Regression Analysis.
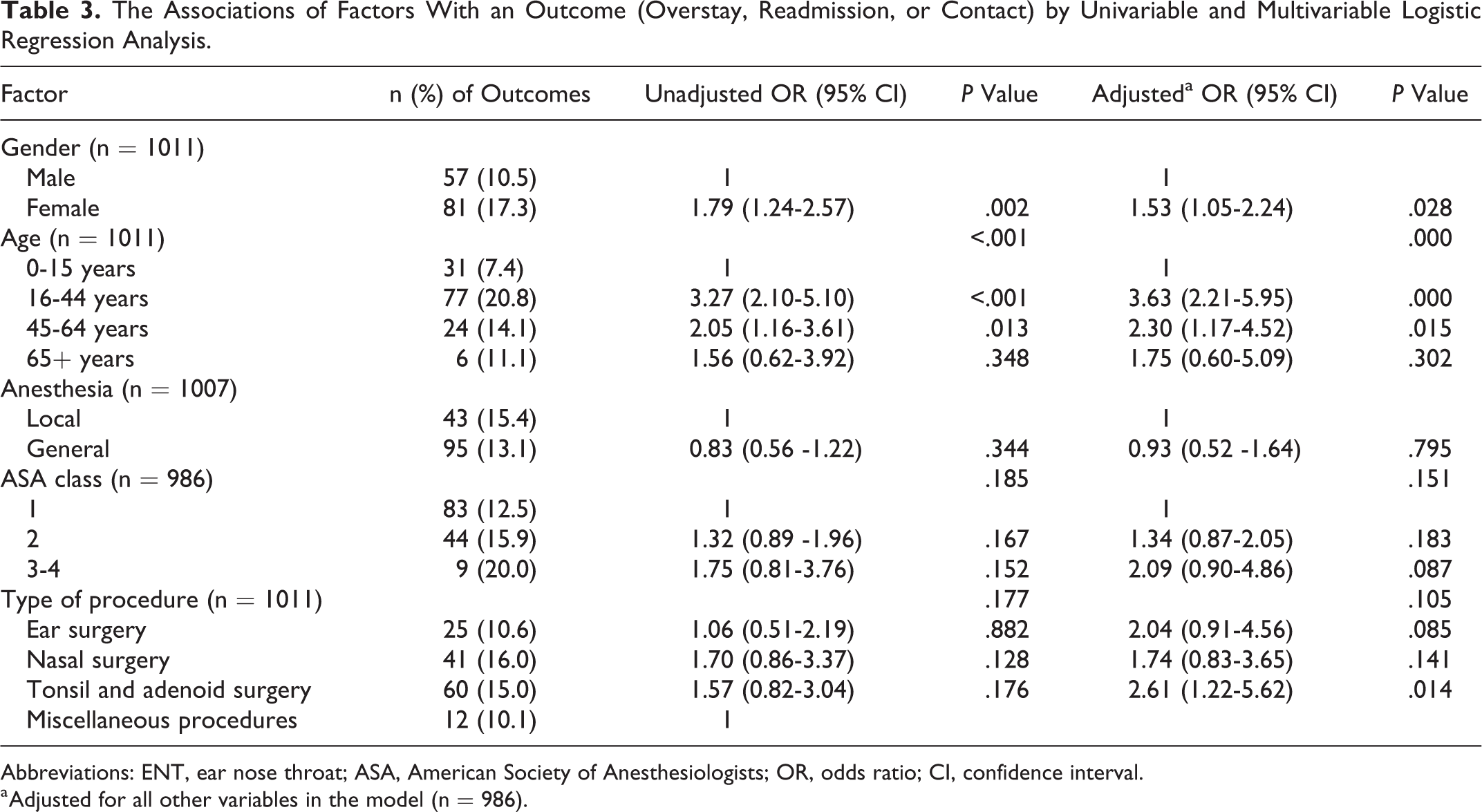
Abbreviations: ENT, ear nose throat; ASA, American Society of Anesthesiologists; OR, odds ratio; CI, confidence interval.
a Adjusted for all other variables in the model (n = 986).
In total, we recorded 29 episodes of post-tonsillectomy bleeding, 2 episodes of post-tonsillotomy bleeding, and 2 episodes of postadenoidectomy bleeding, comprising a postoperative hemorrhage rate of 14.9%, 2.6%, and 1.3%, respectively. Of post-tonsillectomy hemorrhages, 24 received bipolar coagulation under local anesthesia in the emergency department, 6 hemorrhages resolved before arrival at the emergency department, and 3 required a return to the operating room. These 3 patients, however, were small children younger than 6 years old, which was the reason for return to the operating room, not the severity of the hemorrhage.
We examined the form of anesthesia used for each patient (Table 2). All tonsil and adenoid surgeries were performed under general anesthesia. The majority of ear procedures were tube insertions in small children, which were performed under general anesthesia. Of other ear procedures, half were performed under local anesthesia and half under general anesthesia. Of nasal surgery procedures, the majority of each procedure was performed under local anesthesia, except for ethmoidectomies, of which 57% (n = 12) were under general anesthesia. Of the 20 overstays and 14 readmissions, which occurred during our study period, only 4 overstays and 2 readmissions involved local anesthesia. Of 149 contacts, 63 (42.3%) contacts occurred among local anesthesia patients.
Discussion
The most common reason for overstay was nausea and vomiting. Studies have shown that up to 55% of day surgery patients experience nausea and up to 16% vomiting after surgery. 10 Of the 8 overstays due to nausea and vomiting, 3 adults (all female and all tonsil surgery) and 2 children (both male and both adenoid surgery) were affected after tonsil and adenoid surgeries. Nausea and vomiting are known to be common problems in tonsil and adenoid surgeries, especially in the pediatric population, in whom a rate of up to 54% has been reported. 11,12 It has been speculated that gastrointestinal irritation from swallowed blood, diathermy use, tracheal intubation, trigeminal nerve stimulation, and opioid use are all contributing factors. 13 After ENT surgery, gastric decompression seems to be effective in the prevention of postoperative nausea and vomiting. 14
The most common reason for both readmissions and contacts for ENT patients was operation site bleeding after tonsil and adenoid surgery. Adult patients had a post-tonsillectomy contact rate of 11.6% in a US study. 15 Sarny et al discovered a post-tonsillectomy hemorrhage rate of 15% and a post-tonsillotomy rate of 2.3%. 16 These figures are consistent with later studies. 17,18 Tolska et al found an adult post-tonsillectomy hemorrhage rate of 14.5% at our clinic in a previous study. 19 Rates of 0.05% to 0.5% for postadenoidectomy hemorrhage have been documented. 20,21
Readmissions rates have been shown to be 2.01% for ENT day surgery in the United States. 6 Overstay rates in nasal surgery were shown to be 9.62% in the United Kingdom. 22 In our data, readmission rates are below the guidelines set forth by the Royal College of Surgeons.
In myringoplasties (DCD00), stapedotomies (DDA00), maxillary antrostomies (DMB20), and tonsillectomies (EMB10), overstays, readmissions, and contacts were overrepresented in both young adults and females. Of myringoplasties, all patients with overstays and readmissions were both 16 and 44 years of age and female. Of stapedotomies and tonsillectomies, all patients with overstays and readmissions were 16 to 44 years of age, with the majority of tonsillectomy patients also being female. All or the majority of contacts connected with these 4 procedures involved females, with the majority of these also being 16 to 44 years of age. While planning day surgery, patients in these risk groups (females and young adults) should be listened to, and their wishes in regard to anesthesia should be heard. If the patient is uneasy about day surgery, the option to stay overnight should be offered. While women had more study outcomes than men in this study, this may be, at least partially, due to women using health-care services more than men on the whole. 23 -25
While form of anesthesia did not affect study outcomes, we suggest that local anesthesia should be favored when medically and procedurally possible. Of course, due to the nature of some procedures, namely, tonsil surgery, general anesthesia must be used when necessary and cannot be completely eliminated.
This study has some limitations. While local anesthesia had no effect on outcomes of overstay, readmission, and contacts, we did not investigate patients’ care experience or satisfaction postoperatively. The suitability of local anesthesia for septoplasty patients has been investigated at our clinic. Hytönen et al found that only 3.6% of all septoplasty and septocolumelloplasty patients were not satisfied with pain prevention and treatment, with 90% of patients undergoing local anesthesia. 26 One may not be able to extrapolate our experiences to other clinics as pain, and how it is experienced and expressed, is a very culturally and generationally bound phenomenon. This may also explain why patients aged 65 and older faired so well. Age and sex had an effect on outcomes of overstay, readmission, and contacts. This is most likely because the internationally used day surgery criteria select a rather homogenous low-risk group of patients for eligibility for day surgery. Another shortcoming of this study is that we only had access to the contacts and readmissions of patients presenting in the Helsinki and Uusimaa Hospital District hospitals and emergency departments. We have no knowledge of those presenting to their own general practitioner, to the private health-care sector, or visiting the hospital in another municipality. However, these patients most likely number few as in general, patients presenting with postoperative issues tend to be referred to the hospital where the procedure was performed. Also, private health-care centers are usually unable to treat emergency postoperative issues, such as hemorrhage, and thus, the Helsinki University Hospital cares for the majority of these patients. This is a retrospective study, which is completely based on patient files. The weakness of this type of study is that it is based solely on what has been charted. Some phone calls may not have been charted, for example, if the patient did not introduce themselves, and were just given general advice. We did not contact patients to verify how many times they contacted health-care professionals or to inquire about their treatment experience or recovery.
During the past few years, there have only been a few studies concerning ENT day surgery. Since the topic is important both for the patient safety and the operational efficiency of the departments involved, we wanted to improve the knowledge on the factors that affect the outcome of day surgery within various therapeutic areas. 27
Conclusions
At our hospital, criteria for choosing day surgery patients seem to be appropriate. Our overstay, contact, and readmission rates are on the same level, or in some cases even lower, than in previous international studies. While there was no difference in study outcomes in regard to anesthesia (local vs general), general anesthesia does require longer postoperative stays in hospital and is more costly than local anesthesia. Thus, as more procedures are performed under local anesthesia, cost and recovery time will decrease.
Footnotes
Acknowledgments
The authors would like to thank statistician Tero Vahlberg for his statistical analysis and Drs. Annika Takala, Karin Blomgren and Maija Hytönen for their expert advice in their respective fields of anesthesiology and rhinology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Finnish Governmental Grant, The Finnish Medical Association and the Otologic Research Fund of Finland.