
Abstract

Case Presentation
A 44-year-old male known case of bilateral optic nerve sheath meningiomas treated by radiation therapy presented to the voice unit with progressive change in voice quality. Flexible laryngoscopy showed left vocal cord paresis with incomplete closure of the vocal folds during phonation. Computerized tomography of the neck and chest was normal, and neuromuscular testing that included peripheral nerve conduction did not reveal any primary neuromuscular disease. Workup including cerebrospinal fluid studies for cytomegalovirus, Epstein-Barr virus, culture, cytology, Mycobacterium tuberculosis, and oligoclonal band was negative. Laryngeal electromyography of bilateral thyroarytenoid and cricothyroid muscles showed mild chronic neurogenic changes on the left side, suggestive of injury to the left recurrent laryngeal and external superior laryngeal nerves. The patient elected conservative measures with close observation. Follow-up 2 years later showed worsening of his dysphonia with shortness of breath. On laryngeal examination, there was complete fixation of the left vocal fold with mild paresis of the right vocal fold. Neurologic examination also showed evidence of moderate right hypoglossal nerve palsy. The patient underwent injection laryngoplasty of the left vocal fold using 0.5 mL of cross-linked hyaluronic acid (Restylane Q-Med AB, Uppsala, Sweden). The transanal fiberoptic approach was used for the application of laryngeal anesthesia (laryngeal gargle) and for the injection (Figure 1). The patient tolerated the procedure well and had marked improvement in his voice quality.
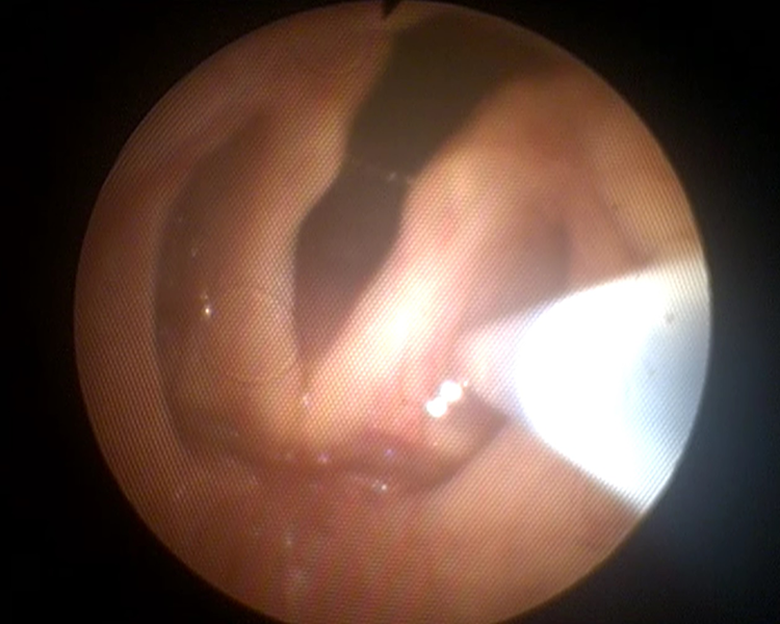
Injection laryngoplasty of the left vocal fold using the transnasal fiberoptic approach.
Discussion
Irradiation-induced cranial neuropathy following treatment of head and neck tumors is a rare complication. The incidence varies from 1% to 9%, with a time lag that may extend up to 35 years. 1 -4 The cranial nerves most commonly affected are the vagus, trigeminal, spinal accessory, oculomotor, abducens, optic, and hypoglossal. 5 -8 Involvement of the recurrent laryngeal nerve with vocal fold paralysis has been described infrequently with a large disparity in the time of presentation. 9 -13 In 1975, Ballantyne described cranial neuropathy as a late sequel of radiotherapy and advocated the protective measures to reduce the rate of radiation-induced complications. 14 Berger and Bataini reported the involvement of the 10th cranial nerve in 9 of 25 patients who developed multiple cranial palsies 12 to 145 months following radiotherapy to head and neck tumors. 7 Takimoto et al reported an 18-year-old female who developed bilateral vocal fold paralysis 5 years following radiation therapy for a nasopharyngeal carcinoma. This complication occurred 10 months after the onset of right hypoglossal palsy. 10 Stern et al reported 3 cases of vocal fold palsy 21 to 34 years following radiotherapy. The authors emphasized the importance of early and long-term follow-up to rule out tumor recurrence or metastasis. 6 Chaudhry and Akhtar reported a case of bilateral vocal fold paralysis years after radiotherapy and noted the difficulty in making the causal association when the complication is late. 15 Based on a report by Lin et al in their study which included 19 cases of irradiation-induced cranial neuropathy, 6 of whom had recurrent laryngeal nerve palsy, the latency period extended up to 20 years. 3 In 2012, Jaruchinda et al reviewed the prevalence of vocal fold paralysis in a group of 70 patients treated with radiation for head and neck cancer. The reported rate was 7.14%, and the lag time varied from 14 to 35 years. 4 Crawley and Sulica reported 10 cases of vocal fold paralysis, all of whom had dysphonia and the majority of whom had dysphagia. The time between irradiation therapy and onset of paralysis ranged between 1 and 27 years. 16
It is important to note that radiation-induced changes to the cricoarytenoid joint may also lead to fixation and/or impaired mobility of the vocal fold. Unless laryngeal electromyography is performed, a misdiagnosis of recurrent laryngeal nerve paralysis is often made. The importance of laryngeal electromyogram in differentiating neural injury from cricoarytenoid joint ankylosis has been emphasized by many authors. 17 How cranial nerves are affected by radiation is not clearly understood. Several mechanisms have been suggested in the literature. One is radiation-induced scarring along the course of the recurrent laryngeal nerve, 11 and a second is vascular insult with ischemia and obliteration of small capillaries leading to degenerative changes. 18 It is worth noting the correlation between the dosage of therapy and vocal fold paresis in patients with lung cancer treated with stereotactic ablative radiation therapy. In the 2 cases reported by Shultz et al, the cumulative dose addressed to the vagal nerve was moderately high in comparison with those who did not develop vocal fold paresis. 12
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.