
Abstract
Verrucous squamous cell carcinoma (VSCC), sometimes called Ackerman tumor, is a highlight differentiated, low-grade squamous cell carcinoma (SCC) variant that is characterized by an exophytic, warty growth, and a broad, pushing border of infiltration below the level of the adjacent uninvolved epithelium basement membrane, comprised of cytologically bland, amitotic squamous epithelium. As a SCC variant, it is strongly associated with tobacco and alcohol abuse. The vast majority of tumors are identified in the oral cavity (Figure 1), with the remaining tumors identified in the larynx, sinonasal tract, and pharynx. Women are affected more often than men by oral cavity tumors, with the reverse in the larynx. Patients present in the sixth and seventh decades of life with large tumors are seen as broad-based, fungating, exophytic, firm masses, generally lacking ulceration. Conservative surgery is usually employed without neck dissection or radiation to achieve an excellent >90% 5-year survival.
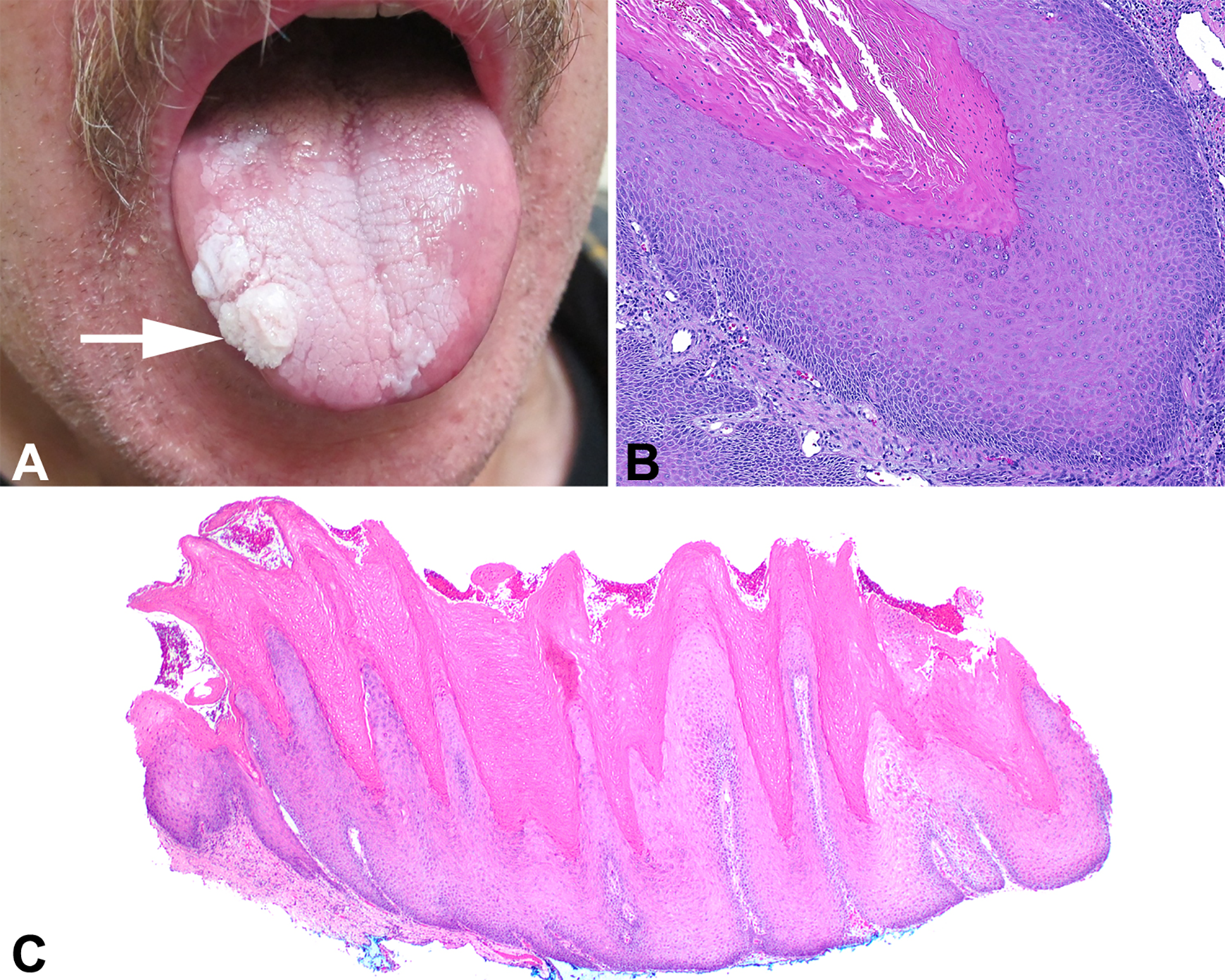
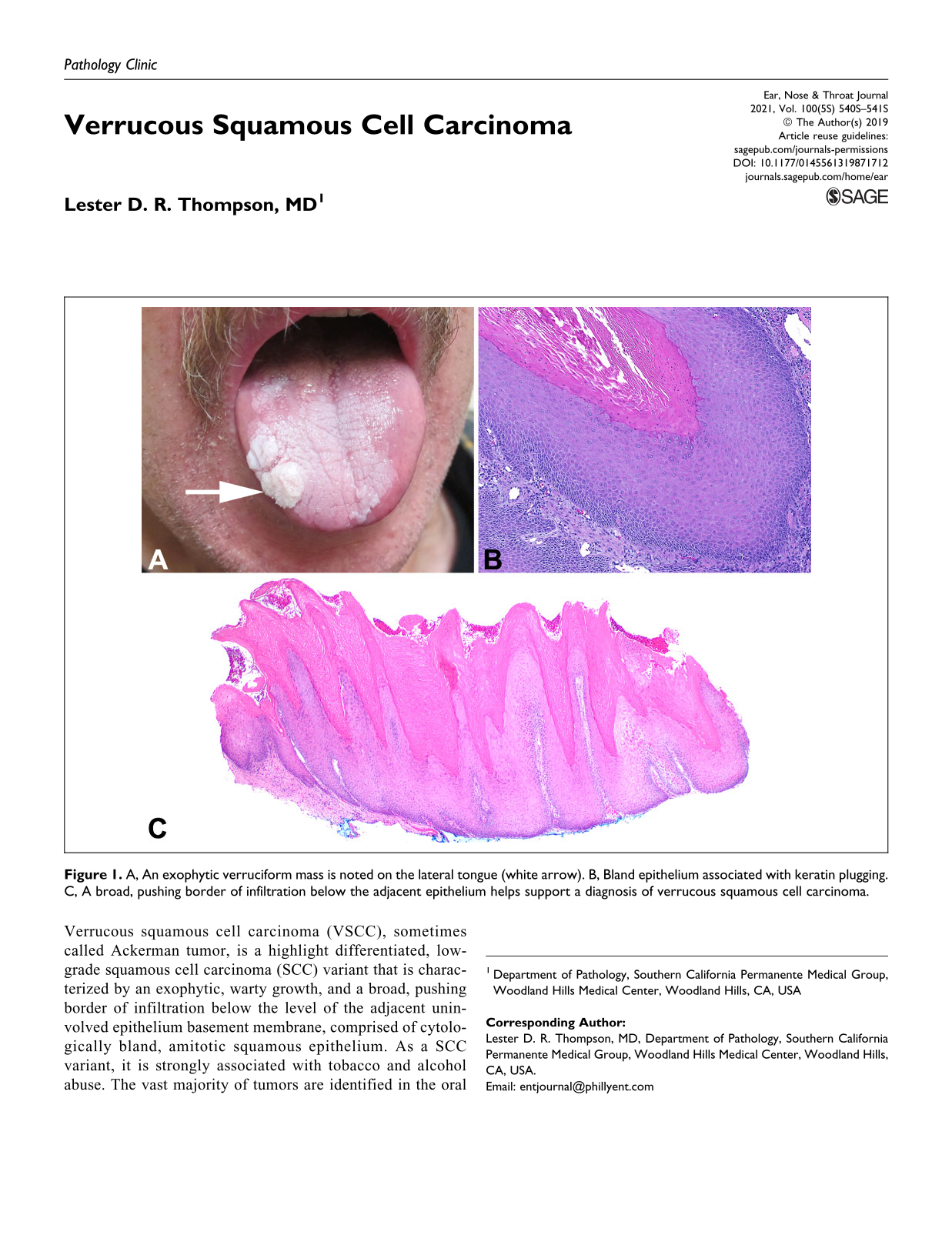
A, An exophytic verruciform mass is noted on the lateral tongue (white arrow). B, Bland epithelium associated with keratin plugging. C, A broad, pushing border of infiltration below the adjacent epithelium helps support a diagnosis of verrucous squamous cell carcinoma.
Most importantly, VSCC is a very well-differentiated variant of SCC in which the epithelium lacks cytologic criteria of malignancy. As such, there is maturation toward the surface, no significant pleomorphism, and generally an absence of mitoses, although rare basal mitoses can be seen. The surface shows marked epithelial hyperplasia of multiple, filiform, finger-like projections of well-differentiated squamous epithelium associated with marked keratosis (hyperkeratosis, church-spire keratosis), parakeratosis, and parakeratotic crypting/keratin plugging (Figure 1). However, it is the thickened, club-shaped, or elephant foot–like broad pushing border of stromal infiltration below the level of the adjacent uninvolved epithelium basement membrane that is required for the diagnosis (Figure 1). This downward dipping of the epithelium creates a cup or “arms” at the periphery, while there is still an intact basement membrane. An inflammatory infiltrate is often present at the advancing edge. In about 10% of cases, clear cut pleomorphism is seen as part of conventional SCC, and in these cases, SCC must be the diagnosis, as it informs management and outcome. Importantly, adequate sampling of the tumor is required to document areas of conventional SCC. Frozen sections are exceptionally difficult to interpret due to sample inadequacies, lack of stromal interface, and tangential sectioning and are thus discouraged. Verrucous squamous cell carcinoma is notoriously difficult to diagnosis, especially when the clinical size or presentation is not known by the pathologist. Verrucous hyperplasia, keratosis of uncertain significance, verruca vulgaris, squamous papilloma, proliferative verrucous leukoplakia, pseudoepitheliomatous hyperplasia, and papillary SCC must be considered in the differential diagnosis and excluded. The diagnosis is only reliably rendered when there is close cooperation and communication between the clinician and pathologist.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.