
Abstract
The aim of this study was to reveal clinical features of benign paroxysmal positional vertigo (BPPV) through comparing idiopathic BPPV and BPPV secondary to vestibular neuritis (VN). The clinical data of the 189 BPPV patients admitted to our tertiary care hospital including otolaryngological, audiological, vestibular, neurological, and radiological evaluations were reviewed. Patients diagnosed with idiopathic BPPV (n = 145) and BPPV secondary to VN (n = 44) were grouped as I and II, respectively. The clinical data of 2 groups were compared. The findings of the study showed that the patients with secondary BPPV due to VN are much younger, have symptoms of only posterior semicircular canal involvement, and require more treatments compared to patients with idiopathic BPPV. The clinical features of patients with BPPV secondary to VN and idiopathic BPPV differ on several aspects. More extensive studies are needed to investigate the underlying etiology in patients with BPPV encountered after VN.
Introduction
Benign paroxysmal positional vertigo (BPPV) is among the most common peripheral vestibular disorders. Benign paroxysmal positional vertigo is characterized by spontaneous resolution after a period of time (benign), short-lasting episodes (paroxysmal), and the symptoms provoked by head movements (positional). Several studies suggested a higher incidence in women with the age of onset between the fifth and seventh decades of life. 1 -4 Elderly people are reported to be at higher risk. 5
In most cases, BPPV is termed as “primary” or “idiopathic” in the lack of evident etiology. The idiopathic BPPV accounts for 50% to 70% of the cases. Head trauma and vestibular neuritis (VN) are the most common causes of “secondary” BPPV, accounting for 7% to 17% and up to 15%, respectively. 2,6 Acute VN is a common vestibular disorder and the patients who had experienced VN can have recurrent attack and subsequent BPPV. 7 Meniere disease, migraines, and inner ear surgery are also shown to be strongly associated with BPPV. 8 -11
The aim of this study was to evaluate the demographic data and clinical features of patients with BPPV through the comparison of idiopathic and secondary to VN.
Patients and Methods
This study involved the retrospective analysis of data of 319 patients who had been admitted to otorhinolaryngology, head and neck surgery clinic of our tertiary care hospital between January 2015 and March 2018 due to BPPV. The data of 189 patients whose criteria are eligible for the study and diagnosed with BPPV were included. Both the study protocol and the use of data were approved by the institutional review board (June 19, 2018; approval no: 2022). All aspects of the study were conducted in accordance with the principles of the Declaration of Helsinki. Patients with a history of inner ear surgery, incomplete clinical data, and with a known etiology including trauma, migraine, and Meniere disease were excluded from the study.
Demographic characteristics and clinical data of the patients including otolaryngological, vestibular system, audiological, neurological, and radiological evaluations were recorded. The medical history including VN, Meniere disease, diabetes mellitus, prior episodes of BPPV, and head trauma preceding BPPV symptoms was revealed.
The diagnosis of BPPV confirmed with positional maneuvers such as Dix-Hallpike or Roll test through the observation of typical nystagmus. The diagnosis of previous VN was defined as acute unilateral vestibular loss lasting at least 24 hours without hearing impairment and concurrent neurological signs with/without caloric test within 18 months before BPPV attack.
Outcome measures included demographic data, the side, semicircular canal (SSC) involved, and the number of sessions required for the treatment and documented resolution of symptoms. The number of sessions required for the treatment was defined as the visits where at least one repositioning maneuver was performed until symptom resolution. The symptom resolution was defined as patient-reported relief from majority of symptoms with the concurrent conversion from a positive to a negative diagnostic maneuver.
The patients were then grouped as primary or idiopathic BPPV (group I) when an etiology was not detected and secondary (group II) when associated with VN. Secondary BPPV was defined as the presence of the previous VN attack within 18 months of BPPV onset. Previous VN attack was referred when participants reported a history of acute unilateral vestibular loss lasting at least 24 hours and decreasing symptoms daily, without cocurrent neurological symptoms and hearing impairment. Peripheral vestibular examination revealed as VN by an ENT specialist within 12 months of the onset of BPPV. The data of the caloric tests if present showing the canal paralysis during the VN episode were also collected.
The patient demographics, the side, semicircular canal involved, and the number of sessions required for the treatment were evaluated for each group and compared between the groups.
Statistical Analysis
The Windows Statistical Package for the Social Sciences program (version 15.0; IBM Corp, Chicago, Illinois, 2008) was used for statistical analysis. The numbers and percentage were used as descriptive statistics for categorical variables, while mean, standard deviation, minimum, maximum, and median were used for numerical variables. When the numerical variable did not meet the normal distribution condition, independent 2-group comparisons were made by Mann-Whitney U test. The ratios in the groups were tested by χ2 analysis. A P value of <.05 was considered to be statistically significant.
Results
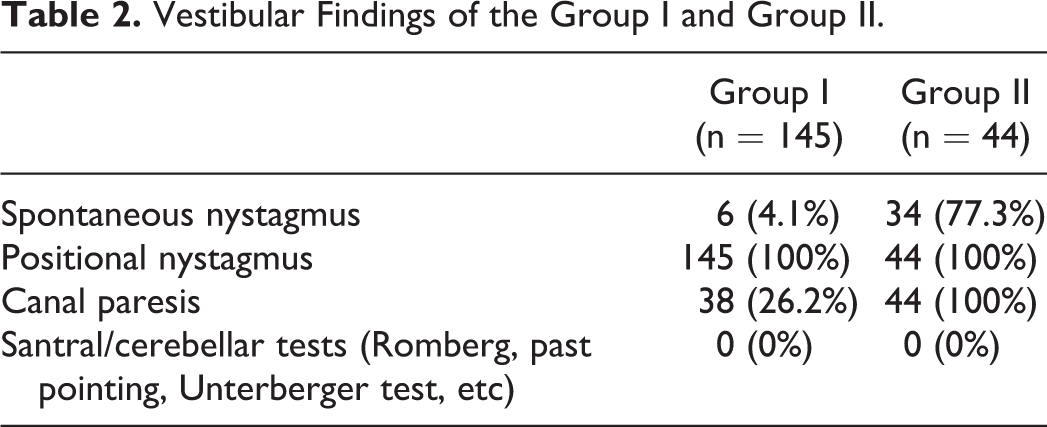
The data of 319 patients with the diagnosis of BPPV between January 2015 and December 2017 were evaluated. The medical records of 62 patients were incomplete, the treatment sessions and follow-up of the 20 patients were not in our clinic, 8 patients had the diagnosis of Meniere disease, and 40 patients had head trauma history prior to BPPV attack. The data of these patients were excluded and the remaining 189 patients were evaluated. The patients were divided into group I and II. The group I consisted of 145 patients with primary BPPV (99 females, 46 males; age between 20 and 92, with a mean age 49.3 ± 15.1). The group II consisted of 44 patients with secondary BPPV after VN (36 females, 8 males; age between 18 and 69, with a mean age 40.9 ± 11.5; Table 1). Of the 44 patients with previous VN, the diagnosis of VN of 17 patients was made by means of positive history and caloric test showing unilateral canal paresis. Remaining 27 patients’ diagnosis had been made on positive history with positive head impulse test and vestibular findings supporting VN diagnosis. Findings of vestibular tests of group I and II are listed in Table 2.
Demographic Features of the Groups.
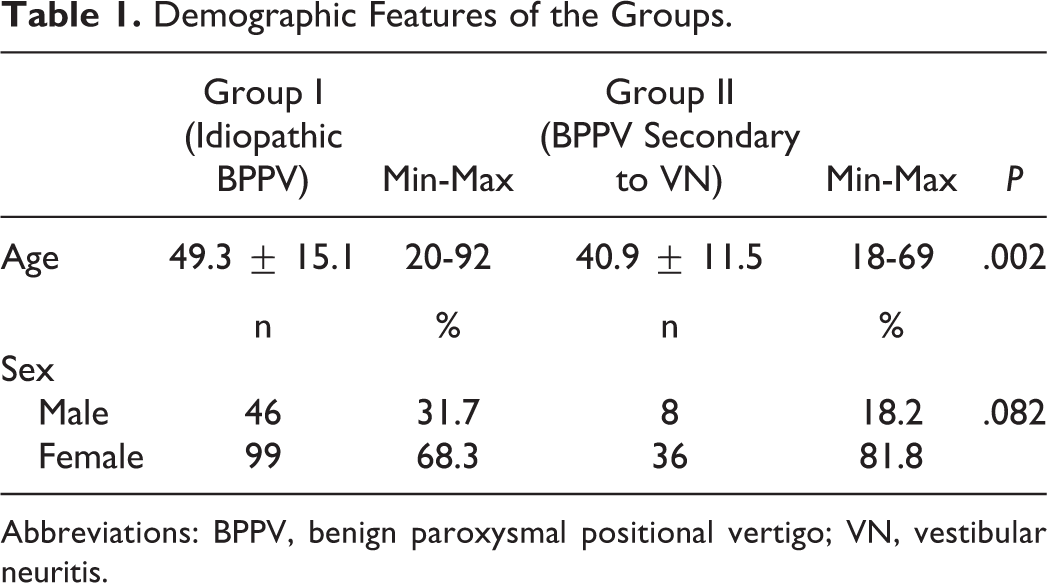
Abbreviations: BPPV, benign paroxysmal positional vertigo; VN, vestibular neuritis.
Vestibular Findings of the Group I and Group II.
The mean age and gender distribution of group I and II were compared. While there was no statistically significant difference in terms of sex distribution between the groups, the mean age of patients was different in group I and II (P = .002).
In terms of SCCs involvement, there was statistically significant difference between the groups (P = .013). All of the patients in group II had experienced only posterior SSC involvement ipsilateral to the involved side during VN attack, whereas 82.1% of the primary BPPV patients had posterior SSC involvement, 13.8% of the patients had lateral SCC BPPV, 2.8% had posterior and lateral SCC BPPV, and 1.4% had superior SSC BPPV (Table 3).
Distribution of the Affected Channels During the BPPV Episode of the Patients.
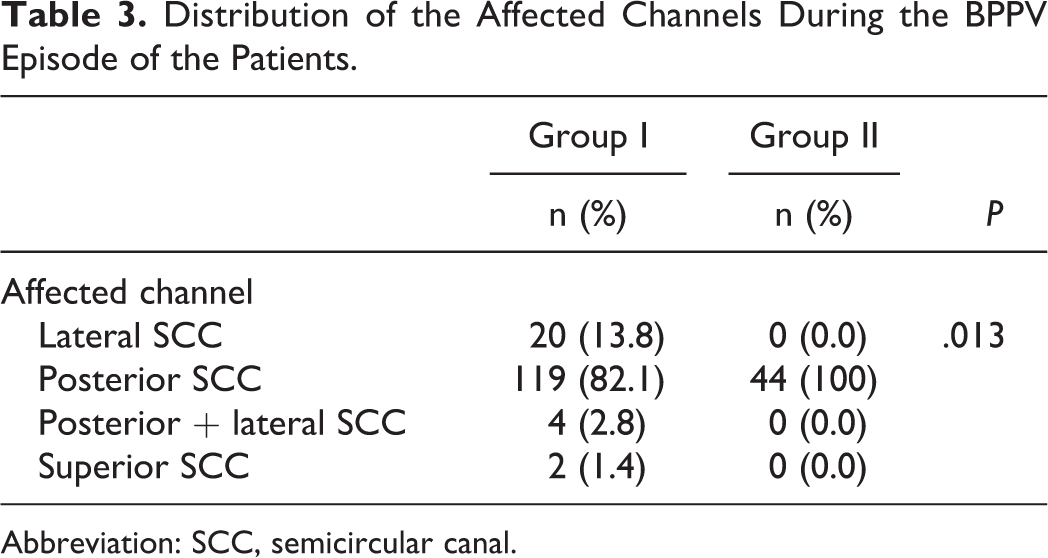
Abbreviation: SCC, semicircular canal.
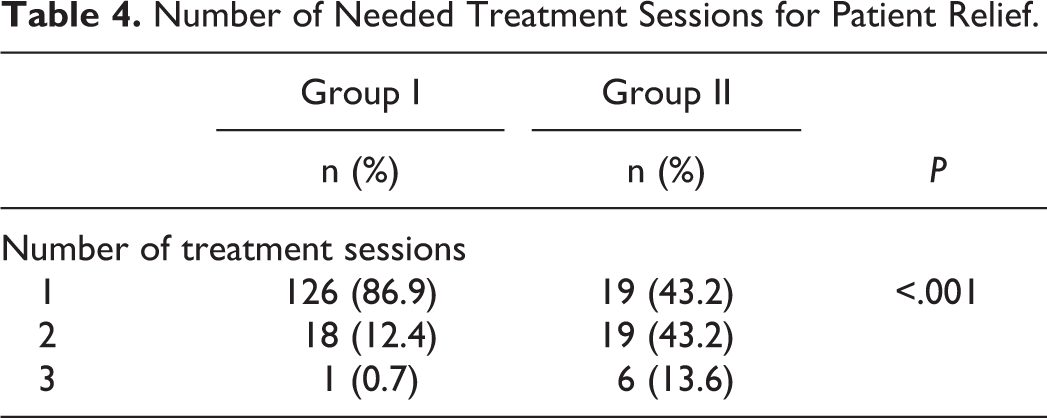
The number of sessions necessary for treatment was higher in group II compared to group I. The difference between the groups was statistically significant (P < .001; Table 4).
Number of Needed Treatment Sessions for Patient Relief.
Discussion
Acute VN and BPPV are common causes of peripheral vestibular vertigo. Benign paroxysmal positional vertigo secondary to VN has been occasionally reported. 12,13 The differences between primary and secondary BPPV with respect to clinical, characteristics, management, and prognosis are not clear.
In our study, the mean age of secondary BPPV patients was detected low that is compatible with the findings of Balatsouras et al. 13 In another study conducted by Mandala et al, the mean age of VN patients with recurrence or subsequent BPPV was lower than whole VN patients. 12 Considering these findings, it can be argued that BPPV is more common with age and VN can occur at any time of life and may increase the risk for BPPV.
All of our patients in group II had BPPV associated with the same side involved during VN. This was concordant with previous reports. 12 -14 This finding implies a pathogenetic relation between the 2 conditions.
The relationship between VN and BPPV is unknown. The underlying mechanism of BPPV secondary to VN may be associated with the anatomical distribution of the vestibular nerve in the inner ear. 7 Vestibular neuritis, usually of viral etiology, often affects the superior vestibular nerve that is more susceptible to the inflammation due to longer pathway in the bony canal compared to inferior vestibular nerve. 15,16
The manifestation of pure posterior canal BPPV implies the preservation of the inferior vestibular nerve in VN. The macula of the saccule and crista of the posterior canal are innervated by the inferior vestibular nerve. In the course of VN, direct damage to macula and utricle results in detachment of otoconia. The detached otoconia via entering to intact functioning posterior SCC duct causes posterior canal BPPV. 17,18
Another suggested mechanism of secondary BPPV to VN is thrombus or ischemic distress of the anterior vestibular artery supplying horizontal SCC and the utricle. 18 The most cases experience posterior canal BPPV at different times after initial episode of acute vertigo and nystagmus. 18,19 In the present study, it was observed that the secondary BPPV group had only posterior SSC BPPV. Previous studies also reported the only posterior SSC BPPV involvement secondary to VN attack. 12,13 We found out that all BPPV episodes observed secondary to VN were in the ipsilateral ear and affected the posterior canal.
In the present study, the number of sessions needed for relief of the symptoms was higher in secondary BPPV compared to idiopathic BPPV. The interval between sessions was 3 days. The 86.9% of patients with idiopathic BPPV had symptomatic relief with concurrent reversion from positive to negative diagnostic maneuver after one treatment session, while patients with secondary BPPV required 2 or more therapeutic sessions (43.2% and 13.6%, respectively). The higher treatment session number in patients with secondary BPPV might be to due subclinical vestibular injury caused by the previous VN attack.
There are few limitations to this study. First, decrease in the number of included patients (189) due to exclusion of 62 patients lacking full data and patients lost to follow-up. Second, since patients’ records were reviewed retrospectively, some patients were lost to follow-up. Also there is lack of caloric test results of all patients, and only some of them had recorded canal paralysis via caloric test. Another limitation is, although it is not an epidemiological study, of the 189 patients, 44 patients were diagnosed with BPPV secondary to VN. A bias toward more increased rates than actual ones could be hypothesized. An explanation for this higher incidence could be due to the fact that our setting is specialized in the management of vertigo and the patients presenting difficulties in diagnosis and treatment are referred from other settings. Besides some patients mostly diagnosed as idiopathic BPPV were diagnosed and treated in emergency department via our consultant doctor. The past medical history and documentation of the sessions applied to them were not recorded in detail in emergency department and thus were not included in the study. Increased patients with BPPV secondary to VN referred from other settings and the excluded idiopathic BPPV patients managed at the emergency department both result in the increased incidence of BPPV secondary to VN in the present study.
The findings of the present study implies that idiopathic and secondary BPPV differ on several aspects including treatment outcome. The patients with BPPV secondary to VN are younger in terms of age with sole involvement of posterior semicircular canal and require more treatment sessions compared to idiopathic BPPV. The detailed evaluation of etiology and clinical course may provide more information in the management of BPPV. Additional studies focusing on underlying pathophysiology are needed.
Footnotes
Authors’ Note
The study was carried out at Otorhinolaryngology Head and Neck Surgery Department, Şişli Hamidiye Etfal Training and Research Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.