
Abstract

Vocal fold (VF) hemorrhage is the result of trauma associated with phonation, cough, intubation, external impact, and other causes. Microvascular disruption leads to hematoma that is often limited to the superior surface but can involve the vibratory margin. Patients commonly report sudden voice change that occurred while performing a strenuous vocal task. 1 However, hemorrhage may be asymptomatic or it can lead to temporary or permanent dysphonia, 2 despite a recent publication that suggests that there are no long-term effects. 3 In the author’s (R.T.S.) experience, that is usually true, but not always.
A 37-year-old male singer presented with increased dysphonia for 3 days. The patient had been diagnosed previously with bilateral VF stiffness and scar, bilateral Reinke’s edema, a VF blood vessel running perpendicular to the vibratory margin, right VF ectasia, intermittently incomplete glottic closure, and laryngopharyngeal reflux. He reported a productive cough with yellow mucus that had started a week prior to his current visit. The patient graded his voice as 3/10 (with 10 as perfect voice) compared to 8/10 prior to the infection. The patient was on dexlansoprazole 60 mg and ranitidine 300 mg, alkaline water, Gaviscon, and a low-acid diet. Videostroboscopy revealed no changes in the previous findings except a new, left, mid-VF hemorrhage involving the vibratory margin and additional edema (Figure 1). Prednisone and absolute voice rest were recommended. One week later during a follow-up visit, the patient stated that he had contracted another upper respiratory tract infection (URTI) associated with rhinorrhea, postnasal discharge, and a cold sore. The patient’s videostroboscopy revealed that the left VF hemorrhage had extended (Figure 2). Levofloxacin, valacyclovir, and acyclovir ointment were prescribed. Absolute voice rest was extended for another week. During follow-up 1 week later, strobovideolaryngoscopy revealed that the hematoma had almost resolved, but there was residual stiffness and an irregular left VF vibratory margin. The patient was advised to use his voice gently, restart therapy with our voice team, and continue reflux treatment. During his 6-week follow-up visit, strobovideolaryngoscopy revealed bilateral VF ectasias associated with VF stiffness (Figure 3) and the patient was scheduled for microscopic laryngeal surgery with KTP laser vaporization of the ectasias and superficial VF steroid injection. During his 3-month postoperative visit, the patient was satisfied with his voice and had received many positive comments regarding his singing voice improvement. His strobovideolaryngoscopy revealed no recurrence of ectasia or additional scar formation after the laser treatment and improved VF vibratory function (Figure 4).
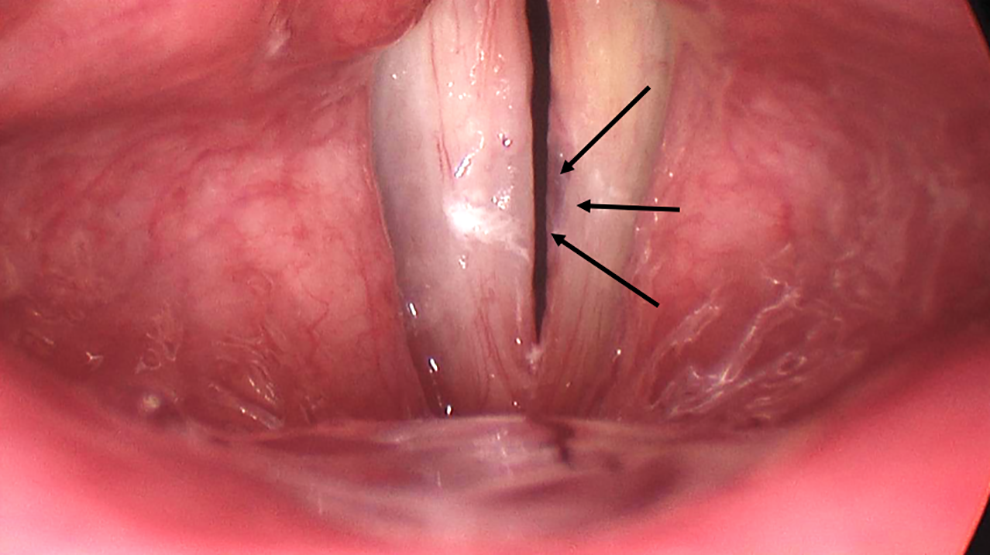
Initial visit: Videostroboscopy shows left focal mid-vocal fold hemorrhage on the vibratory margin (black arrows).
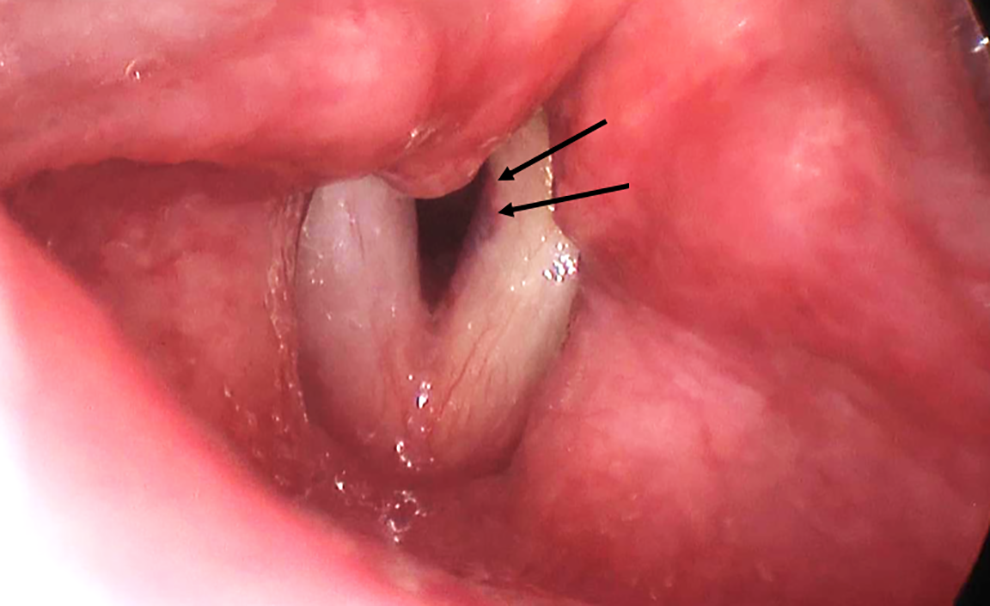
One-week follow-up visit: Videostroboscopy reveals the left focal mid-vocal fold hemorrhage extended posteriorly (black arrows).
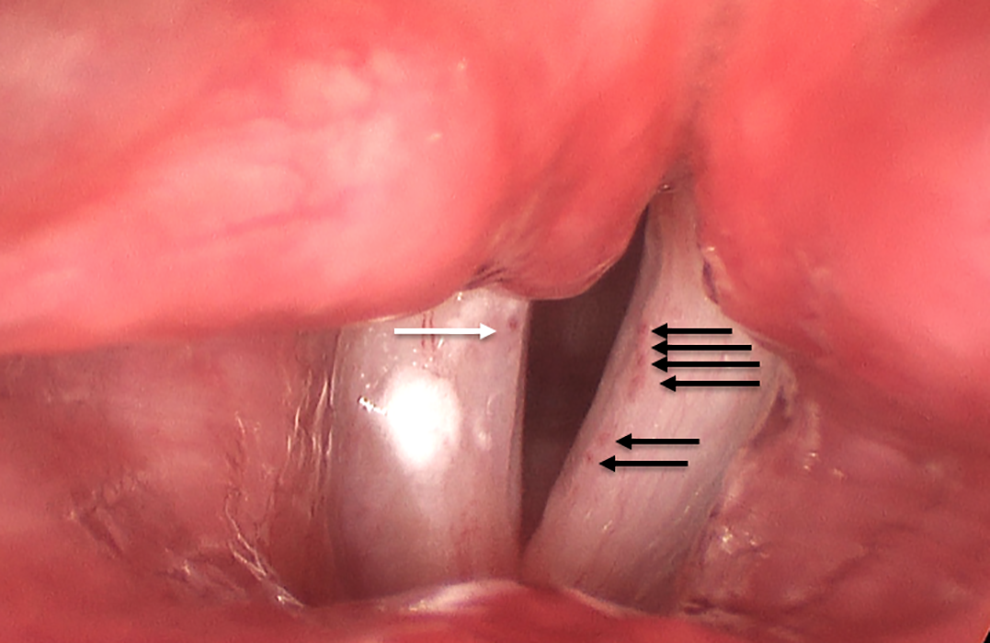
Six-week follow-up visit: Videostroboscopy reveals multiple left vocal fold ectasias (black arrows) and right VF ectasia (white arrow), as well as a deep sulcus on the left vocal fold in the area of previous hemorrhage and current increased stiffness. VF indicates vocal fold.
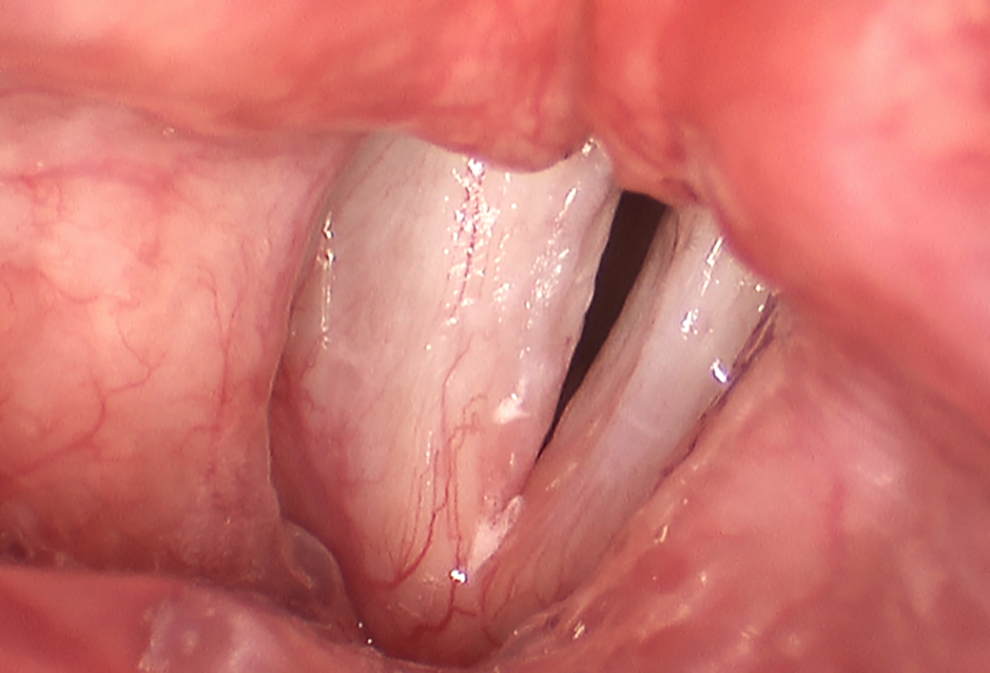
Three-month postoperative visit: Videostroboscopy shows no recurrence of the ectasia and improved left vocal fold sulcus and vocal fold vibratory function.
Risk factors associated with VF hemorrhage include trauma, premenstrual hormonal status, use of anticoagulants (including aspirin and nonsteroidal anti-inflammatory drugs), acute URTI, hyperfunctional voice abuse, reflux laryngitis, and environmental factors (such as air quality, dust, smoke, stage, fog), VF ectasia and varices, and others. Vocal fold hemorrhage usually heals within 7 to 10 days. Total voice rest without throat clearing is advised, although there is no definitive evidence confirming its efficacy. Cough suppressants are used when needed, as well as hydration. 2 -4 Alternative treatment approaches include the use of homeopathic Arnica montana 5 pellets 3 times daily and bromelain 500 mg twice daily, an enzyme from pineapple that reportedly accelerates resolution of clots. 4 Hyaluronidase injection into the VFs was reported by Dr Woo for 3 patients of acute vocal hemorrhage with early fusiform polyp formation, and marked reduction in the size of the polyp with significant reduction in the Voice Handicap Index-10 were noted. 5 Surgical options usually are recommended for recurrent VF hemorrhage or nonresolving cases. 6 With early diagnosis, voice rest and follow-up with appropriate voice therapy and singing training, most patients achieve full recovery. 2,7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.