
Abstract
Laryngotracheal disruption in children is rare but life-threatening, and endolaryngeal injuries may go overlooked. We present the case of a 10-year-old boy who sustained near-complete laryngotracheal separation, multiple laryngeal fractures, and arytenoid and vocal fold avulsion following blunt cervical trauma. These injuries were not identified radiographically and only became apparent intraoperatively. Following surgical repair, the patient was successfully decannulated, eating a normal diet, and had a serviceable speaking voice within 2 months. In children, the diagnosis of severe endolaryngeal injuries may be elusive and therefore require high degree of clinical suspicion. Surgical success requires accurate diagnosis and prompt intervention.
Introduction
Acute airway compromise presents the most obvious and urgent complication of laryngeal trauma; however, disruption of the dynamic elements of the larynx such as the vocal fold and arytenoid complex may also have drastic long-term consequences. 1 -3
In the pediatric population, treatment algorithms are often loosely extrapolated from the adult population and focus primarily on maintaining airway patency and less frequently on long-term voice and swallowing function. 1,4,5 Although arytenoid and/or vocal fold avulsion are often not life-threatening in isolation, external blunt force trauma is also not likely to produce these injuries in the absence of severe disruption of the laryngeal skeleton. Due to other concomitant major injuries to the laryngeal skeleton and other organ systems in the setting of trauma, nonobstructive endolaryngeal lesions are often overlooked at the time of injury and underappreciated in trauma algorithms.
To better illustrate the diagnostic and treatment challenges associated with these injuries, we present a case of traumatic laryngotracheal separation with arytenoid and vocal fold avulsion in a child. Radiographic images, intraoperative findings, and management strategies are discussed, and a review of the literature is provided.
Case Report
A 10-year-old otherwise healthy male presented to an outside emergency department after a bicycle accident. During his fall, his anterior neck fell directly onto the longitudinal axis of the handlebars. He immediately developed dysphonia, hemoptysis, and stridor. In the emergency department, his respiratory distress progressed and orotracheal intubation was attempted. Due to the absence of a visible airway, the decision was made to perform an urgent tracheostomy. Following the procedure, physical examination identified subcutaneous emphysema of the neck and upper chest. Chest radiography revealed a right tension pneumothorax, and a thoracotomy tube was placed. The patient was stabilized and transferred to our institution for further management.
Upon arrival, flexible nasolaryngoscopy demonstrated diffuse and severe laryngeal edema and concern for vocal fold height mismatch. After assessment and stabilization, a neck computed tomography (CT) was performed (Figure 1). Diffuse subcutaneous emphysema involving the cervical soft tissues and mediastinum was noted. The tracheostomy was seen entering the lateral trachea, displacing the carotid artery posteriorly. The nonossified nature of the larynx precluded identification of any obvious laryngeal fracture; nevertheless, there remained a high suspicion of laryngeal framework injury based on the mechanism of trauma and endoscopic findings. The patient was taken urgently to the operating room for panendoscopy, neck exploration, potential reduction of laryngeal fractures, and revision tracheostomy.
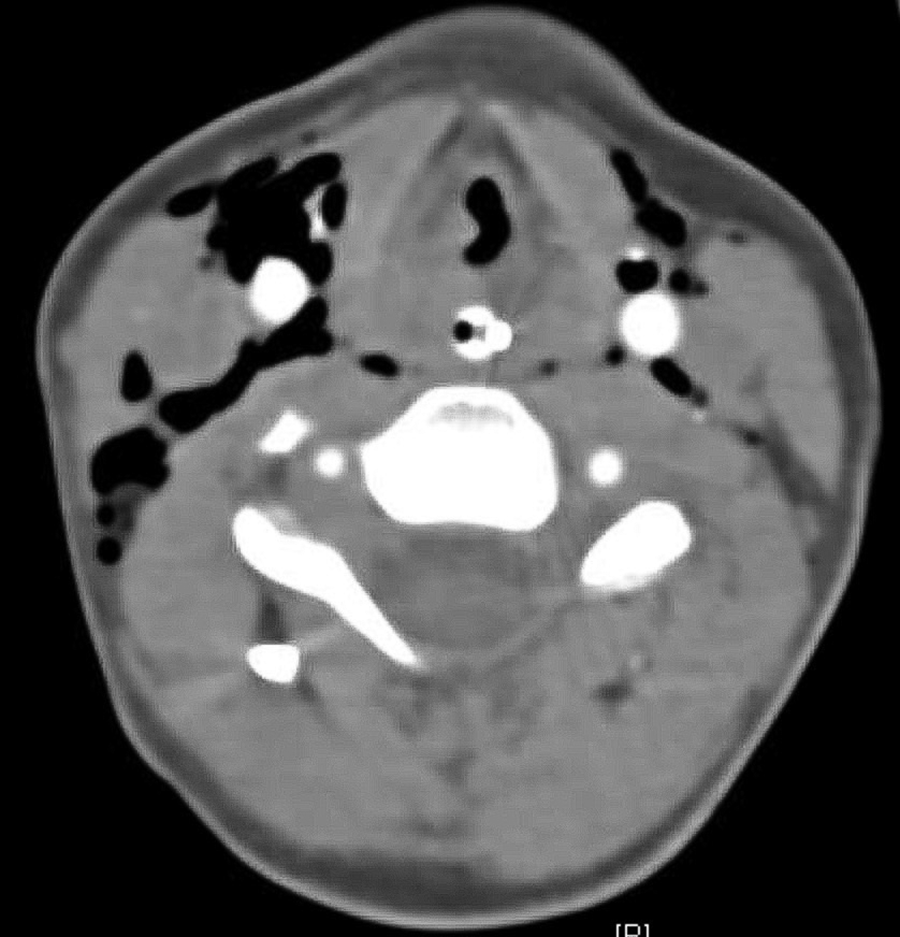
Axial computed tomography (CT) scan with intravenous contrast, at the level of the laryngeal skeleton demonstrating significant subcutaneous emphysema. Note the poorly ossified nature of the laryngeal skeleton, which made the identification of any laryngeal fracture difficult.
Laryngoscopy demonstrated several endolaryngeal abnormalities including a large left vocal fold hematoma, avulsion of the right vocal fold with dislocation and disruption of the mucosa overlying the right arytenoid cartilage, and significant height mismatch of the true vocal folds (Figure 2). The subglottis was occluded, and the cricoid was collapsed medially into the lumen. The esophagus was intact.
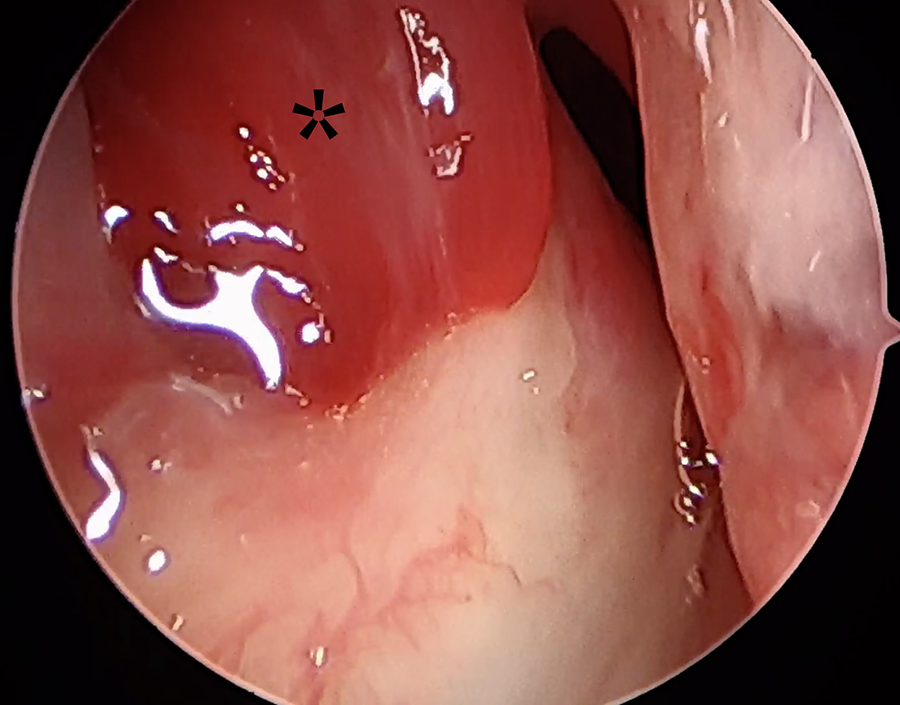
Initial laryngoscopy demonstrating a left vocal fold hematoma (*) and absent right vocal fold body.
An open neck exploration was performed (Figure 3), revealing multiple cricoid fractures and separation of the cricoid cartilage from the remainder of the larynx. Multiple comminuted fractures of the thyroid and cricoid cartilages, arytenoid avulsion, and complete dissociation of the right vocal fold from the anterior commissure were noted. The recurrent laryngeal nerves were exposed bilaterally and noted to be intact; there was severe edema, and the nerves were under tension due to the separation. The endolarynx was visible via the fracture sites, one of which was a near-complete vertical laryngofissure, oriented to the right of midline. The larynx was opened judiciously via the fracture site allowing the mucosa to be further visualized. There were multiple endolaryngeal lacerations, one of which exposed the arytenoid cartilage that was bare and rotated into the lumen of the subglottis. Under magnification, the anterior aspect of the avulsed vocal fold was identified and suspended anteriorly to the thyroid alar cartilage, using the intact left vocal fold as a guide for positioning. In doing so, this allowed for reduction of the arytenoid body, reorienting it to its native position. The mucosa overlying the exposed right arytenoid cartilage was then approximated. The thyroid alar fractures were reduced and stabilized with polydioxanone suture. A 9-mm transglottic suprastomal stent was placed spanning the cricoid and proximal trachea and secured with Prolene suture. The cricoid fractures were reduced over the stent, and the cricoid was resuspended to its native position within the laryngeal framework.
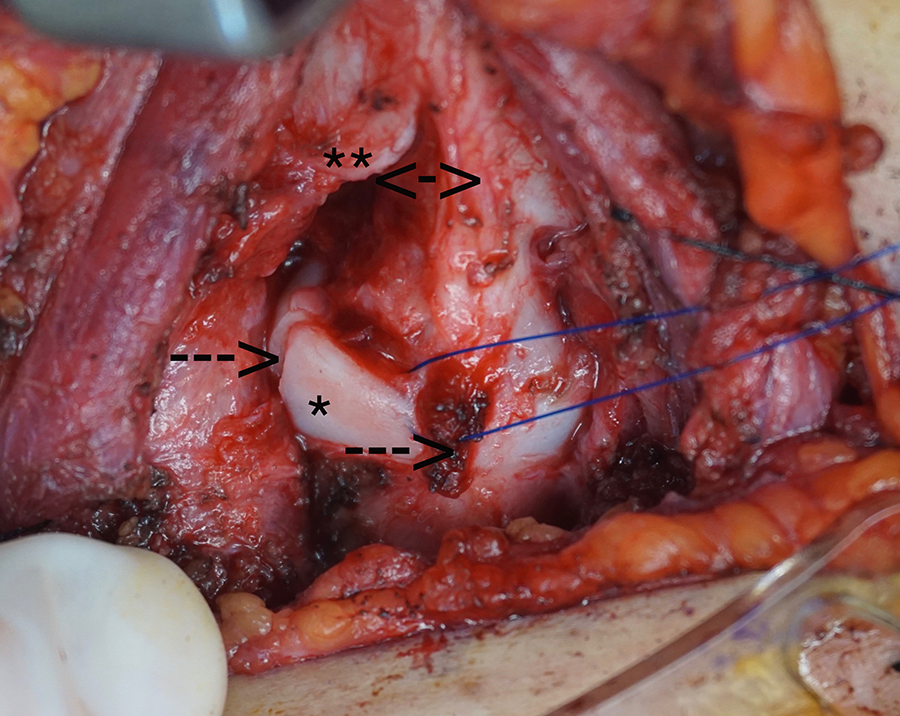
Operative findings demonstrating fractures of the cricoid cartilage (C) and laryngeal cartilage (L) with cricolaryngeal separation.
The remainder of the patient’s initial hospital stay was uneventful. He was discharged home on postoperative day 10 with a tracheostomy tube and stent in place and tolerating a regular oral diet.
Direct laryngoscopy following stent removal at 1 month (Figure 4) demonstrated a widely patent airway with appropriate positioning of the arytenoid cartilages. Two months following the initial injury, he underwent successful decannulation. He underwent temporary injection laryngoplasty to judiciously medialize the right vocal fold, which was hypomobile; however, the vocal fold was appropriate in height and volume. At 1-year follow-up, the patient has a strong speaking voice, continues to eat a normal oral diet, and is participating in normal childhood activities.
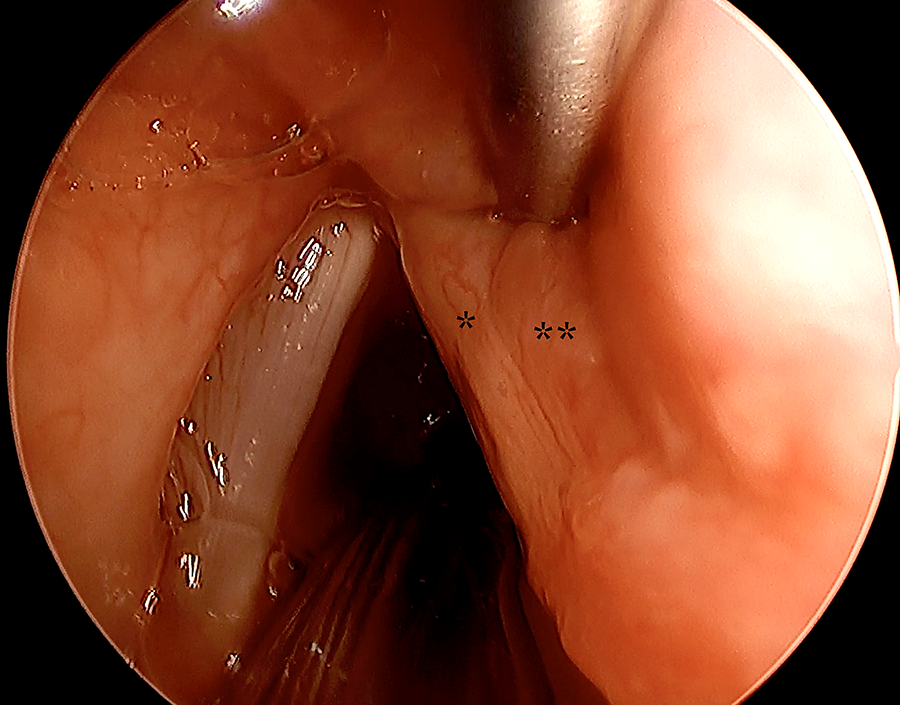
At 1 month from the initial injury, laryngoscopy following stent removal demonstrating a widely patent airway with well-aligned arytenoid cartilages. Notable was right vocal fold edema (*) and supraglottic inflammation (**).
Discussion
Laryngotracheal disruption, although rare, has a high mortality. 1,2 Diagnosis and treatment should be timely, given the possibility of acute decompensation as well as the risks of associated long-term sequelae. 6 While management should include airway security prior to addressing swallow function and voice restoration, the latter should not be underappreciated. Patient and parent counseling should include a discussion of these goals and the expectations at each stage of treatment. While the majority of the existing body of literature regarding pediatric laryngeal injury focuses on the acute management of life-threatening sequelae, 7 this case also demonstrates the importance of addressing more subtle endolaryngeal injuries at the time of the initial intervention so as to achieve better long-term quality-of-life outcomes.
An algorithm for establishing a patent airway, while obviously of the utmost importance, may be difficult to navigate in this setting. Clinicians, and in particular first responders, must balance the urgency of establishing an airway against the risk of worsening existing injury or causing further airway obstruction. Immediate tracheostomy in lieu of orotracheal intubation presents the most controlled method to establish an airway and is utilized in approximately 33% of cases. 6 Nevertheless, tracheostomy may not completely stabilize the airway, and the distal airway may be highly mobile in the case of complete mid-laryngeal disruption as demonstrated here.
Although imaging may help guide surgical intervention, false negatives may exist in the pediatric population due to the lack of laryngeal ossification; thus, imaging findings should not be used in isolation to justify an observational versus surgical approach. In contrast, imaging may delay life-saving intervention, and patient stability and airway security must be carefully assessed prior to obtaining imaging. In addition, radiologic studies are unlikely to identify endolaryngeal injuries that could have longer term implications. Although arytenoid dislocation and vocal fold avulsion are not necessarily life-threatening, in this case, late recognition of these findings would have reduced the ability to recreate the anterior commissure appropriately and to orient the body of the arytenoid cartilage in its native position. With an airway secured via a tracheostomy and no evidence of these findings on CT scan, one may be tempted to wait several days or weeks to reevaluate the airway. This may be a critical mistake that would reduce chances of restoring long-term voice outcomes.
In this case, the existing traumatic opening into the larynx was further distracted to allow for endolaryngeal evaluation, reapproximation of the anterior commissure, and repositioning of the arytenoid cartilage. Had the larynx been managed more conservatively with a simple reduction in fractures, approximation of mucosal lacerations, and stent placement, the patient would have had a severely displaced arytenoid and vocal fold, making short-term airway obstruction and long-term dysphonia and aspiration more likely.
Fortunately, traumatic avulsion of the arytenoid following blunt trauma is rare. Of the reported cases, the majority of vocal fold avulsions are minor in severity and able to be reapproximated endoscopically. 8 There are 2 prior reported cases of open repair of the vocal process, both performed when in the presence of existing fracture to the cartilaginous laryngeal framework, using existing laryngofissures to access the repair as was performed here. 9 In contrast to these reports, the case herein describes complete avulsion of the vocal fold and mucosa of the conus elasticus, requiring a repair of the entire margin of the vocal fold and repositioning of the arytenoid concurrently. Repositioning the anterior margin of the vocal fold under some degree of traction allowed proper seating of the arytenoid. This highlights the opinion of the authors that securing the vocal fold anteriorly prior to attempting to manually position the arytenoid and repair the mucosal lacerations is likely to be met with more success than the performing these steps in the opposite order. By addressing these injuries at the initial intervention, better long-term voice outcomes are more likely to be achieved if subsequent interventions are required.
Conclusion
The diagnosis of laryngeal fractures in children is reliant on a high index of clinical suspicion and will often require surgical exploration. Open management of endolaryngeal injuries is a suitable option in the presence of existing traumatic laryngofissures. Early operative intervention with subsequent interval endoscopic maintenance procedures can achieve very acceptable functional voice and swallowing outcomes.
Footnotes
Authors’ Note
Written informed consent for patient information and images to be published was provided by the patient’s legal authorized representative.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.