
Abstract

During a Head and Neck surgical training camp in Malindi, Kenya, a 25-year-old male with a large mandibular ameloblastoma was evaluated for surgery given persistent growth and deformity secondary to his lesion. The patient underwent oral cavity composite resection and reconstruction with a fibular free flap. On the evening of postoperative day 1, there was concern for venous congestion of the flap. A 20-gauge needle was used to prick the flap, but this bedside maneuver did not allow the team to definitively diagnose nor exclude venous congestion. A portable ultrasound with Doppler functionality (Figure 1) had been heavily implemented during the surgical camp for purposes of workup of thyroid lesions, neck masses, and other tasks amenable to ultrasonography as well as for teaching purposes for the local surgeons involved in the camp. Using the portable ultrasound, both the arterial and venous components of the flap pedicle were identified in the neck and had good flow when Doppler was engaged. The vein was traced proximally until the coupler was identified (evidenced by a subcentimeter round object within the pedicle that produced shadowing). Flow was identified on both sides of the coupler, indicating good venous outflow of the flap (Figure 2). The patient was observed and ultimately progressed without further incident. The use of a portable ultrasound for this somewhat atypical indication allowed the patient to avoid unnecessary reoperation.
Portable ultrasound device. Philips Lumify portable ultrasound system including the L12-4 transducer (Philips Healthcare, Amsterdam, the Netherlands) and a Galaxy 10.1 tablet (Samsung, Seoul, South Korea) with the Lumify system.
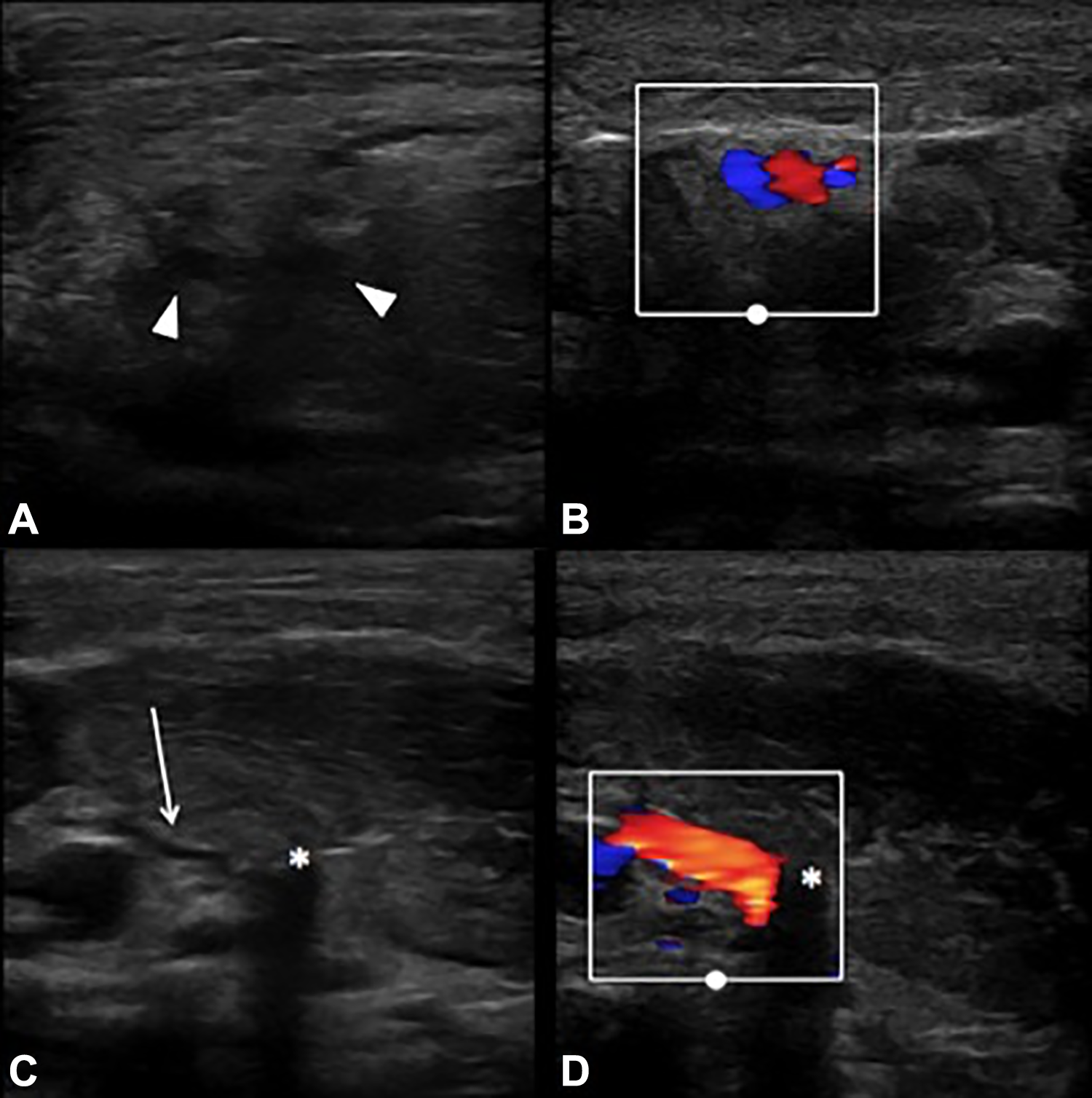
Free Flap pedicle and venous coupler on ultrasound. A, Image of the vein and artery of the flap pedicle. Both vessels are seen in cross section (arrowheads). B, More proximal view of the pedicle with Doppler engaged, showing the close association of the 2 vessels. C, Distal view of the vein which is slightly compressed by the ultrasound probe (arrow) and the venous coupler causing shadow effect (asterisk). D, Doppler engaged showing flow through the venous coupler.
As indicated above, this case occurred in a resource-scarce environment wherein many of the frequently used tools and mechanisms for free flap monitoring are unavailable. Although handheld external Doppler was available to the surgical team, the loss of a Doppler signal can often be a late finding after vascular flow for a free flap has already been compromised. 1 Our team utilized a portable ultrasound device to interrogate the free flap anastomosis in effort to overcome some of the limitations imposed by working in this resource-limited setting. The use of ultrasound to visualize free flap anastomoses is rarely described in the Head and Neck literature 2,3 and is seldom used given the reliability of external Doppler or implantable Doppler technology. 4 Many challenges exist in performing advanced Head and Neck procedures in low- and middle-income countries (LMICs). 5,6 These challenges extend beyond the surgery itself and into the postoperative period as highlighted by the present case. In fact, difficulty with adequate postoperative monitoring and care has previously been described as potentially the greatest challenging in perform advanced procedures in LMICs. 7 As such, those involved in surgical outreach and otolaryngology missions should be prepared to utilize whatever resources are available to their full extent. Along these same lines, we feel that portable ultrasound equipment becomes an almost invaluable tool in the hands of a surgeon well versed in point-of-care imaging and diagnostics.
Footnotes
Acknowledgments
The authors would like to thank Caris Foundation, Kenya for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.