
Abstract
Although the image quality from modern distal chip endoscopes is superior, limited mobility of the endoscopic tower prevents this technology from being used in inpatient and emergency departments. In these settings, otolaryngologists commonly use older flexible laryngoscopes with portable light sources. However, these light sources could malfunction. Smartphones are ubiquitous nowadays, and the smartphone’s flashlight may be used alternatively to provide illumination when primary light malfunctions. This study compares the ability of flashlights from various smartphone models in providing adequate illumination for flexible laryngoscopy when compared to a commercially available portable light source. White wall and mucosal images were captured using Olympus P4 flexible scope and lights from the Stryker X8000 endoscopy tower light source, Storz 11301D3 portable light source (control), iPhone 4, iPhone 6, iPhone 8, iPhone X, Galaxy S6, and Galaxy S7. ImageJ was used to quantify pixel intensities with white and black standardized as 250 and 0, respectively. Student 2-tailed t test was used for analysis. The endoscopic tower outperformed all other light sources in all categories. The iPhone 4 and iPhone 6 consistently underperformed in comparison to the Storz 11301D3 portable light source (P < .05). Galaxy S6, Galaxy S7, and newer generation iPhone 8 and iPhone X provide comparable pixel intensities to Storz 11301D3 portable light. Smartphones incorporate different types of light-emitting diodes. Newer Galaxy and iPhone provide adequate illumination for the endoscopic assessment of the airway when compared to commercially available portable light source. However, one should always utilize the best commercially available light source in nonemergent cases.
Introduction
Flexible laryngoscopy is a key diagnostic tool used by otolaryngologists to assess voice, swallowing, and airway complaints in the outpatient, inpatient, and emergency department settings. Currently, most well-equipped otolaryngology offices utilize endoscopic towers with powerful light sources and high-definition distal chip laryngoscopes to provide optimal imaging. These towers can be equipped to record examinations for comparison with future endoscopies, to perform stroboscopy, and sometimes even to perform transnasal esophagoscopy. These capabilities and improved image quality make endoscopy towers the preferred equipment in more predictable outpatient office settings, but the tower itself lacks mobility for use in inpatient wards and emergency departments, especially when these are located in different buildings. Therefore, most otolaryngologists prefer to use a more mobile setup with a fiberoptic flexible laryngoscope and a portable light source when assessing patients outside of their normal office setting.
Although portable light sources are effective, they can malfunction for many reasons including an insufficient battery charge, a burned-out light-emitting diode (LED), equipment wear-and-tear, accidental damage, or even loss. In a nonemergent situation, one will have time to troubleshoot the portable light source or find an alternative light source to perform the airway examination. However, in emergencies such as airway crises, one might not have time to obtain another light source immediately. As an emergency alternative, the tip of the light cable from the laryngoscope may be held against a smartphone’s LED flashlight to provide illumination for assessment of the airway as shown in Figure 1. Panels A and B demonstrate the light intensity at the tip of the scope in a well-lit room and in the dark, respectively.

Utilization of smartphone flashlight as an alternative endoscopic light source (A) in a well-lit room and (B) in the dark.
However, the varying brands and models of smartphone do not have the exact same flashlight setup, making it possible that some models will be more suitable for this application than others. Often, quick tricks such as this appear to work for the user but are never formally tested. The objective of the present study is to compare the commercially available Storz 11301D3 portable light source to various different models of smartphones in providing adequate illumination for visualization of the airway.
Methods
For this study, no institutional review board approval was required as our study included less than 5 patients. One of the coauthors gave consent and served as a test subject for obtaining mucosal images. We used the Storz 11301D3 portable light source as a control and the Stryker X8000 tower as the gold standard. The following smartphones were used as test instruments: Apple’s iPhone 4, iPhone 6, iPhone 8, iPhone X, and Samsung’s Galaxy S6 and Galaxy S7. Models were selected to represent the most popular currently used smartphones and based on availability. Older phones such as the iPhone 4 and iPhone 6 were included since they were still circulating in the market. Images were captured using a Stryker SDP1000 HD camera attached to the Olympus P4 flexible laryngoscope. We first captured images of a white wall in a dark room with different light sources and then proceeded to capture mucosal images. These included images of the sublingual frenulum, the supraglottis, and the glottis. To minimize variability, images were taken from the same location while one person stabilized the scope, the second person switched out the light source, and the third person captured the image. For each cell phone model, the phone was placed face down on a level surface and the tip of the light cable was held vertically in place so that it directly touched the LED flashlight ensuring that all of the light passed through the scope’s light cable with minimal dissipation. The brightness of the LEDs was also adjusted to their maximum using the in-phone applications. Images were uploaded to ImageJ for analysis. All images were converted to 32-bit grayscale to eliminate the need to analyze each image in its separate primary components of red, green, and blue. Thus, the pixel intensity was standardized between 0 and 250, where 0 represents a completely black pixel, and 250 represents a completely white pixel. For each image, the mean, minimum, and maximum pixel intensity were calculated using ImageJ. Statistical analysis was performed using a Student 2-tailed t test against the Storz 11301D3 portable light source with a P value of less than .05 as significant differences.
Results
Figure 2 shows the images captured using different light sources. With a quick assessment of the images, one can qualitatively conclude that the iPhone performed poorly compared to the Galaxy phones and Storz 11301D3 portable light when view side by side. Table 1 summarizes the quantitative values of the mean pixel intensity of various light sources with a graphical format showed in Figure 3.
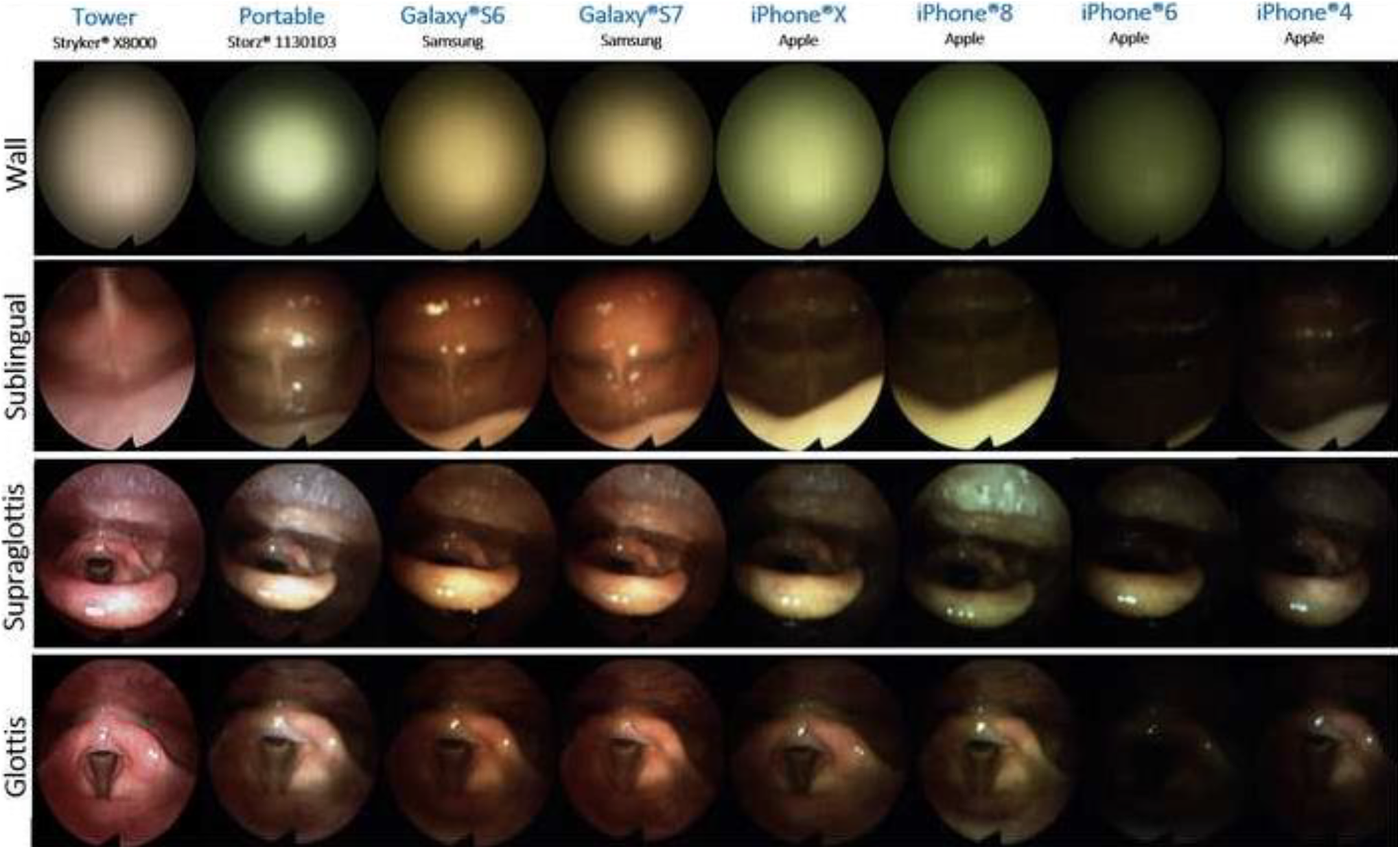
Images of wall, sublingual frenulum, supraglottis, and glottis with various light sources.
Mean Pixel Intensities and P Values for Different Light Sources.
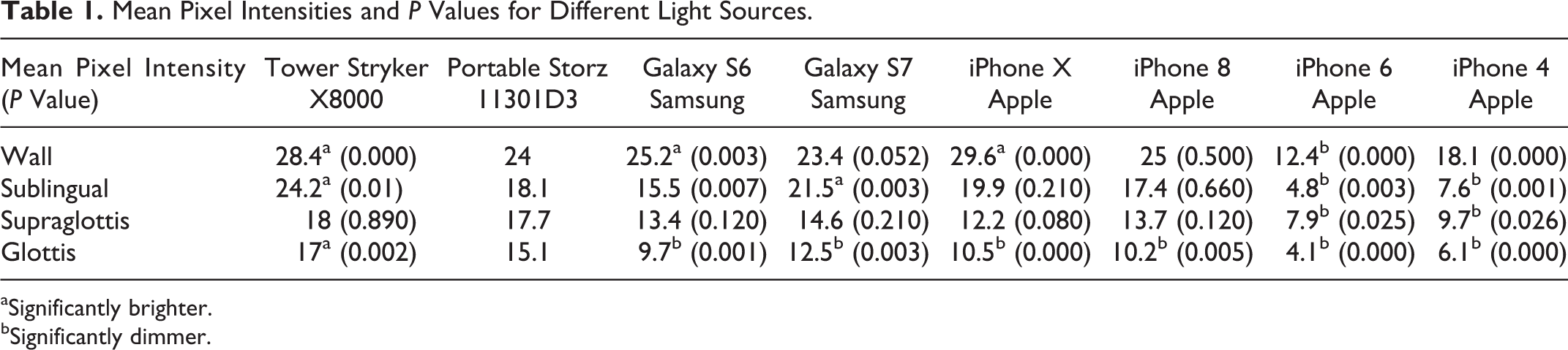
aSignificantly brighter.
bSignificantly dimmer.
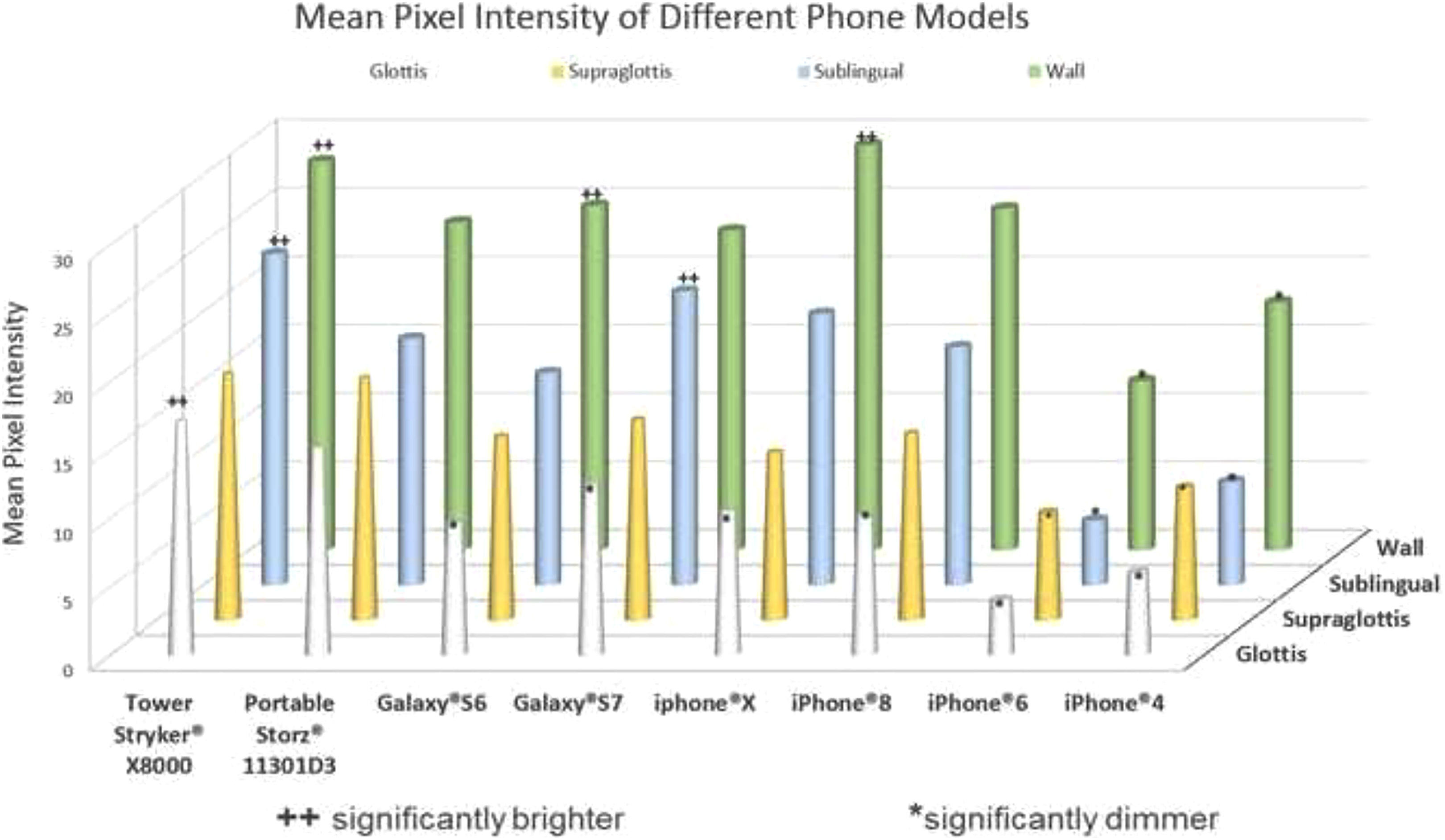
Mean pixel intensities in graphical form with ++ indicating significantly brighter and * indicating significantly dimmer than the control Storz 11301D3 portable light source.
When comparing the mean pixel intensity of images of the white wall, the Stryker X8000 tower, iPhone X, and Galaxy S6 light sources all had a significantly higher mean pixel intensity than the Storz 11301D3 portable light source (P = .00, P = .00, P = .03, respectively). Images captured with iPhone 4 and iPhone 6 had significantly decreased mean pixel intensity compared with the Storz 11301D3 portable light source (P = .00). When analyzing mean pixel intensity of the sublingual images, the Stryker X8000 tower and Galaxy S7 showed significantly better intensity (P = .01, P = .03) than the Storz 11301D3 portable light source, while the iPhone 4 and iPhone 6 again showed significantly lower pixel intensity (P = .003, P = .001). Analysis of supraglottis images showed no phones were able to outperform the Storz 11301D3 portable light source but did again show that the iPhone 4 and iPhone 6 resulted in significantly decreased pixel intensity (P = .025, P = .026). Finally, analysis of glottis images showed mean pixel intensity generated by all tested phones to be significantly lower than the Storz 11301D3 portable light source (P = .000-.001).
Discussion
Smartphones are now increasingly used in the medical field due to mobility, high processing power, and the development of novel health-care applications. 1,2 Liu et al compared the use of a video-recording adapter for an iPhone 5S to a video tower and found no difference in endoscopic video quality and diagnosis when assessed by 13 different otolaryngology faculties and residents. 3 Lozada et al studied the feasibility of using mobile recording by otolaryngology residents for inpatient consults and found it to be effective. Only in 5 of their 79 cases was there a change in diagnosis and management when an attending physician reviewed the recorded examination, and only one case required a repeat laryngoscopy. 4
The intent of our current study was to explore the feasibility of a helpful trick, using the smartphone flashlight as a light source for flexible laryngoscope in emergent clinical situations in which an endoscopy tower or portable light source might not be available. We compared mean pixel intensity of representative images obtained with each light source (tower, portable Storz 11301D3 light, and different smartphone models) of a blank wall and different anatomic regions (sublingual frenulum, supraglottis, glottis). Not surprisingly, the Stryker X8000 tower provided the best light source on both qualitative and quantitative analysis. It consistently captured images with the highest pixel intensity and significantly outperformed the Storz 11301D3 portable light in all test condition. Of the different smartphones, the Samsung Galaxy models generally provided the most intense light, with the Galaxy S6 and Galaxy S7 each outperforming the Storz 11301D3 portable light on the wall and sublingual pictures, respectively. The older iPhone models (iPhone 4 and iPhone 6) consistently provided the worst illumination and showed significantly lower light intensity compared to control in all images. The newer iPhone models (iPhone 8 and iPhone X), however, provided better light intensity, with the iPhone X showing significantly higher light intensity than the Storz 11301D3 portable light source in the wall images. Importantly, when evaluating light intensity of images captured from the glottis, all smartphone models revealed significantly decreased pixel intensity compared to the Storz 11301D3 portable light source. However, the images from Figure 2 indicate that the iPhone 8, iPhone X, Galaxy S6, and Galaxy S7 subjectively provided adequate lighting to assess the glottis airway.
In addition to quantitative analysis of light intensity provided by various light sources, other qualitative factors should be considered when evaluating a smartphone’s ability to illuminate the airway for effective clinical examination. The first factor is the phone’s LED array. Figure 4 shows each particular phone’s LED configuration which will result in unique pattern of light distribution.

Galaxy phones are equipped with a single LED, while different iPhone models utilize multiple LEDs. Note: iPhone 8 and iPhone X models have same LED light. LED indicates light-emitting diode.
The wall images in Figure 2 shows that the endoscopy tower light provides a diffuse light intensity causing the center and surroundings to appear almost homogenously bright. In contrast, the Storz 11301D3 portable light source illuminates a defined center of maximal intensity with a surrounding area of noticeably lower brightness. The Galaxy smartphones grossly provide light distribution patterns similar to the Storz 11301D3 portable light source. The newer iPhone models (8 and X) produce improved global illumination while the iPhone 4’s single LED delivers a small well-defined area of brightness with larger surrounding area of dimmer light. The iPhone 6 produces a diffusely dark image correlating with its consistently lowest values of light intensity throughout all images. These differences in light distribution may have clinical implications. Light sources that provide a diffuse, homogenous pattern of illumination (eg, Galaxy S6 and S7) may allow for simultaneous visualization of the majority of the airway and surrounding mucosa facilitating rapid clinical assessment. Light sources with focal areas of brightness and larger areas of surrounding darkness (eg, iPhone 6) may require increased movement of the endoscope to fully visualize all areas of the airway and surrounding mucosa making a thorough examination more time consuming and uncomfortable for the patient.
Gross differences in light source color are also observed in the images of the blank white wall. As seen in Figure 2, the iPhone models generally result in white wall images with a green tint, while Galaxy smartphones furnishes wall images with a red-orange tint. This is in contrast to the Storz11301D3 portable light source which produces images with a light-green tint, and the Stryker 8000 tower light which produces images with a beige tint. This leads to variation in mucosal color in the endoscopic images. Mucosal color in images captured with the Galaxy S7 is a vibrant pink and appear similar to the mucosal color visualized in images taken with the Stryker 8000 tower light source. Images captured by the Storz 11301D3 portable light source captured pink mucosa but with increased pallor and desaturation. The images taken with different iPhones generally result in a blue-green tinting of the mucosa and also show significant desaturation. These changes may make assessment of some mucosal lesions problematic.
Important limitations must be discussed in relation to this study. Due to the technical difficulty of maintaining a consistent position of the endoscope while taking images in succession, there likely were some minor differences in the position of the scope tip relative to the structures being observed. These variations could have slightly altered the visual field observed when using the different light sources and may have impacted the quantitative and qualitative image analysis. Mucosal movement also occurred during real-time image capture and resulted in variations in light scatter patterns which influenced overall image brightness and quality between light sources. Another factor worth mentioning is the variable amount of light lost that occurred with holding the phone light source up against the light cable of the laryngoscope. It was possible that the researcher could have held the light source of certain smartphones against the light cable in a more optimal manner than others, thus influencing image light intensity and quality, despite our best efforts to keep this standardized. It is also important to realize that the images visualized and analyzed on the computer differ from what is seen by the human eye during real-time endoscopy. When images are recorded by the computer and displayed on the monitor, a significant amount of digital processing occurs. As a result, images undergo slight distortions resulting in color differences, added graininess due to pixilation, and other potential degradations of image contrast, glare, and depth perception. It is likely that these distortions occurred in an evenly distributed manner across images from all light sources, but it was possible that images taken with certain light sources less accurately depicted real-time endoscopic imaging than others. Finally, aside from quantification of light intensity, no assessments of other image quality (eg, glare, color, contrast, pixilation, blur) were performed because they could be subjective and hard to objectively verify. Just looking at the images in Figure 2, it is apparent that there are varying color hues. Although we used grayscale in our analysis to minimize confounders, we may have uncovered more differences between the light sources and we analyzed the red, green, and blue components of each image. Such an analysis would have been more important and our results shown that smartphone LED lights could be consistently used as an alternative light source. Even though smartphones and their applications are increasingly used in the health-care field, the medicolegal aspects of their uses are in flux. 5
In light of the aforementioned possible image distortions that can occur with using a smartphone LED as a light source, we recommend that a smartphone should never be used as a light source to perform laryngoscopy in routine, nonemergent situations or in emergent situations when there is access to a commercially available portable light and video tower. However, when the primary light source fails and when there are no alternatives, an otolaryngologist may potentially utilize a smartphone light as a backup light source to get a general idea of the airway. He or she should remain calm and instruct the nurse and other medical staff on how to hold the light cable against the smartphone’s LED light with the illumination turned to maximum brightness from the in-phone application. The otolaryngologist needs to be aware that by choosing to use a smartphone light source, he or she may be missing details as the entire visual field is not homogenously illuminated.
The Stryker X8000 tower remains the superior light source in terms of pixel intensity when conducting an endoscopic examination of the upper aerodigestive tract. It or another comparable tower light should be the first choice when conducting a routine examination or when evaluating the airway in an emergent situation. However, should these light sources fail, particularly when timing is critical, the first best step is to always ensure a backup light source and additional batteries and bulbs are carried with the physician. Should this backup plan somehow fails, LED lights of the majority of current smartphones have been shown to provide a temporary alternative. Newer smartphone models, such as the Samsung Galaxy S6 and Galaxy S7 and the Apple iPhone 8 and iPhone X performed comparably with the commercial Storz 11301D3 portable light control while older models such as the Apple iPhone 4 and iPhone 6 consistently underperformed. Should a smartphone be needed as a light source in such a case, it is recommended that a newer model Samsung Galaxy or Apple iPhone is used and that at least 2 people are available during the process, one guiding the scope and another directing the light. This “trick” we have described can give a quick general look into the upper aerodigestive tract, but it is important that the user understand crucial details that could impact care might be missed and therefore not recommended when patient’s condition is noncritical. The limitations of this study highlight the need for further analysis to assess whether a smartphone’s LED light can be used in a nonemergent setting.
Footnotes
Authors’ Note
This project was accepted as an oral presentation for the 122nd America Academy of Otolaryngology–Head and Neck Surgery Annual Meeting at Atlanta Georgia in Oct 2018. iPhone is a trademark of Apple, Inc. and Galaxy is a trademark of Samsung Electronics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.