
Abstract
It is known that lymph node metastasis lowers the survival rates in laryngeal carcinoma. This study aimed to investigate the effect of extranodal extension in lymph node metastasis on survival. The demographic characteristics and histopathologic results of 81 patients who underwent total laryngectomy and neck dissection due to advanced larynx squamous cell carcinoma between 2011 and 2018 were reviewed retrospectively. The patients were divided into 3 groups by lymph node metastasis status as reactive lymph node (group 1), lymph node metastasis without detected extranodal extension (group 2), and lymph node metastasis with detected extranodal extension (group 3). Survival analysis was performed between these 3 groups. In the patient population with a mean age of 61.56 years consisting of 6 females and 75 males, demographic characteristics between groups were comparable. Overall survival (OS) rates were detected to be 81% in group 1, 69.2% in group 2, and 61.5% in group 3. Two-year OS rates were detected to be 66.7% in group 1, 46.2% in group 2, and 38.5% in group 3. Statistical difference was detected between group 1 and group 3 both for OS and 2-year OS (P = .014, P = .008, respectively). No statistical difference was detected between group 2 and group 1, and between group 2 and group 3. In this study, we found a negative effect of detecting neck lymphadenopathy metastasis and extranodal extension on survival in patients who underwent total laryngectomy and neck dissection due to advanced laryngeal carcinoma.
Introduction
Approximately 13 000 patients are diagnosed with laryngeal cancer annually, and 85% to 95% of these tumors are squamous cell carcinomas. Most of the patients with advanced larynx cancer have locally advanced disease. 1 Advanced laryngeal cancer has a poor prognosis, and independent from the treatment method, 5-year survival rate is 39% to 60%. This is mostly because of being unable to control the regional and distant spread of the disease. 2,3
Clinical tumor–node–metastasis stage has been used as a criterion in the therapeutic management of patients with head–neck cancer. Cervical lymph node metastasis staging was based on the size, number, and localization of nodes with positive lymph node metastasis staging. 4 However, most of the time, lymph node staging is not an adequate prognostic factor. Therefore, we need to consider the characteristics of lymph node metastasis for postoperative adjuvant therapy following surgical treatment. Detecting extranodal extension (ENE) in cervical lymph node following neck dissection has been demonstrated to be more associated with regional and distant failure rates. 5,6 In the eighth edition of the American Joint Committee on Cancer (AJCC), lymph node staging was reorganized by emphasizing the importance of ENE. 7
This study assessed the lymph node stages of the patients who underwent total laryngectomy and bilateral neck dissection due to advanced larynx cancer and investigated their effects on survival.
Materials and Method
Six female and 75 male patients with a mean age of 61.56 ± 9.1 years who underwent total laryngectomy and bilateral neck dissection due to advanced (stage 3-4) squamous cell laryngeal carcinoma between March 2011 and November 2018 were evaluated retrospectively. All patients were retrospectively investigated after receiving approval of local ethics committee (2018/15-10). All patients gave informed consent before the surgery. The lesions in the larynx were assessed according to the eighth edition of the AJCC cancer staging manual. 7
Data regarding age, sex, smoking status, tumor localizations, histological grades, laryngeal cartilage invasion status, the presence of lymph node metastasis, ENE in patients with lymph node metastasis, comorbidities, death status, adjuvant therapy, overall survival (OS), and 2-year survival rates of the patients were collected. We recorded the death status of the patients from national citizenship services.
The treatment modalities for each patient were discussed at multidisciplinary head and neck oncology team meetings consisting of experienced surgical, medical, and radiation oncologists. Indications for adjuvant therapy (radiotherapy or chemoradiotherapy) were determined based on the pathologic findings of each patient, such as status of resection margins, local invasiveness, and cervical lymph node involvement.
Patients who were detected to have distant metastasis, patients who previously underwent partial laryngectomy and radiotherapy, patients who were detected to have comorbid thyroid carcinoma, and patients with tumoral continuity at surgical margin were excluded from the study. Microscopic margins smaller than 1 mm were considered positive.
All lymph nodes excised in neck dissections were assessed for ENE by the pathology department. The patients were divided into 3 groups by lymph node metastasis status as reactive lymph node (group 1), lymph node metastasis without ENE (group 2), and lymph node metastasis with ENE (group 3).
The data were evaluated using the IBM SPSS Statistics 22.0 (IBM Corp, Armonk, NY, USA) statistics package software. Descriptive statistics were given as number of units (n), percentage (%), mean ± standard deviation
Results
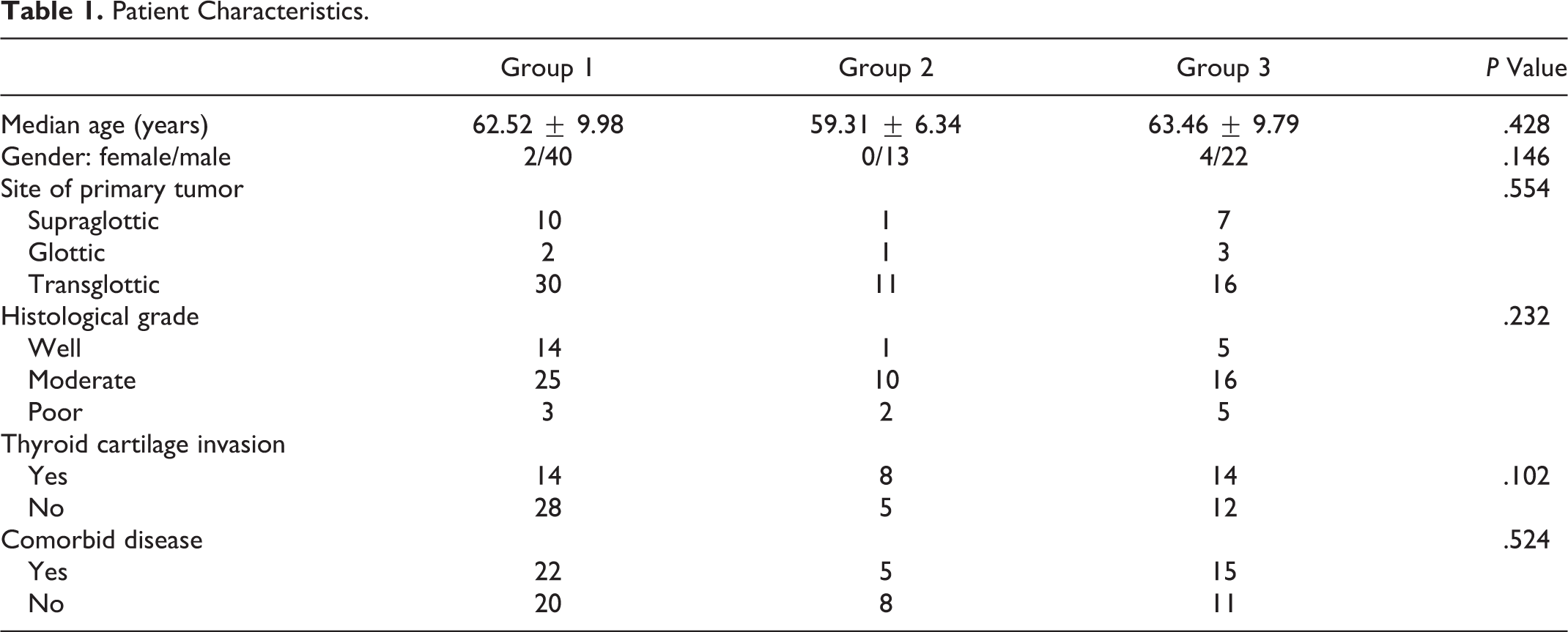
The mean postoperative follow-up period was 57.12 months (range: 2-93 months). When the data were evaluated, 59 patients were found to be alive and 22 patients were dead. Recurrence was detected in 5 patients who died. Forty-two (51.85%) patients were detected in group 1, 13 (16.04%) in group 2 and 26 (32.09%) in group 3. All patients were observed to be smokers. In group 1, 14 (33.3%) patients were referred to adjuvant therapy. In group 2 and 3, all patients were referred to adjuvant therapy. There was no statistically significant difference in terms of age, gender, tumor localization, histological grade, thyroid cartilage invasion, comorbidities, and adjuvant therapy between group 1, group 2, and group 3 (Table 1). The OS rates were detected to be 81% in group 1, 69.2% in group 2, and 61.5% in group 3. Median OS was 70.67 months (95% confidence interval [CI]: 58-82) in group 1, 44.54 months (95% CI: 31-57) in group 2, and 41.55 months (95% CI: 28-54) in group 3 (Figure 1). Two-year OS rates were detected to be 66.7% in group 1, 46.2% in group 2, and 38.5% in group 3. Two-year median OS was 64.32 months (95% CI: 53-75) in group 1, 36.75 months (95% CI: 23-49) in group 2, and 33.30 months (95% CI: 21-45) in group 3 (Figure 2). Statistical difference was detected between group 1 and group 3 both for OS and 2-year OS (P = .014, P = .008, respectively). No difference was detected between group 1 and group 2, and group 2 and group 3 for both OS and 2-year OS (P = .214, P = .259, respectively). No difference was detected between group 2 and group 3 for both OS and 2-year OS (P = .440, P = .341, respectively).
Patient Characteristics.
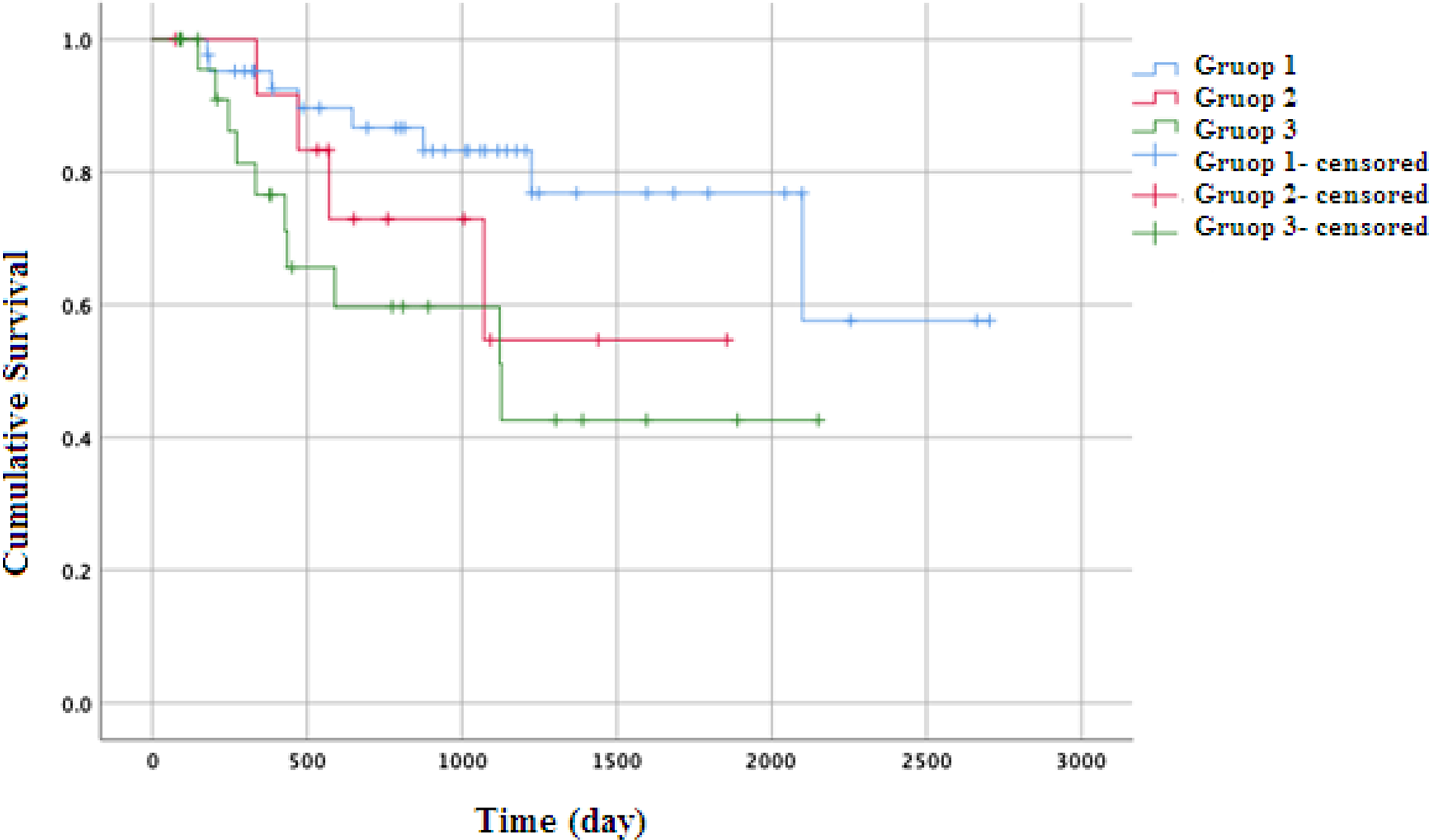
Kaplan-Meier curves for overall survival (95% confidence interval).
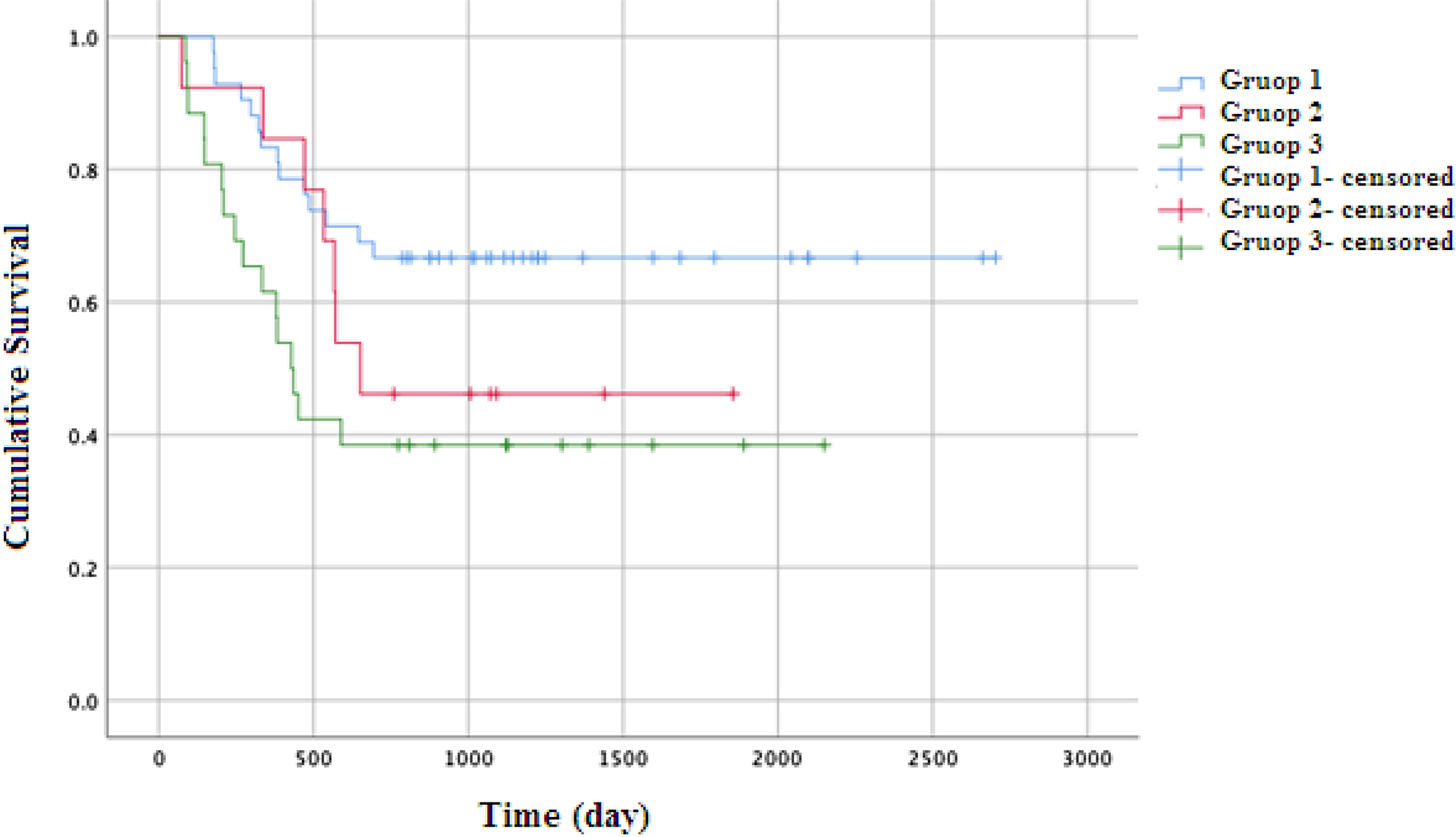
Kaplan-Meier curves for 2-year overall survival (95% confidence interval).
Discussion
The prognosis of laryngeal carcinoma following curative surgery is estimated based on T classification, origin region, resection margins, presence of lymph node metastasis, and disease stage. In their study, Papadas et al stated that advanced laryngeal carcinomas (stage 3-4) are associated with a decrease in survival and detected a 5-year OS of 53% and 33% for stages 3 and 4, respectively. 8,9
Controlling the cervical lymph node metastasis and determining the prognostic factors are important for determining the prognosis of laryngeal carcinoma. In their study, Khoueir et al stated that lymph node involvement affects the survival more than T stage. 10 If cervical lymph node metastasis is ignored, the number of patients with poor prognosis due to postoperative regional recurrence or distant metastasis may increase greatly. 11 –13 In our study, while 2-year OS rate was 66.7% in patients without lymph node metastasis in neck, it was 46.2% in patients with lymph node metastasis without ENE. This shows that lymph node metastasis greatly affects the survival rate even without ENE.
Extranodal extension is stated to be tumor spread to the soft tissues other than lymph nodes. 14 Since the first time ENE was defined by Bennett et al, several studies have reported that ENE is associated with poor prognosis. 13,15,16 Additionally, single lymph node metastasis detected in early-stage laryngeal carcinoma surgery requires postoperative radiotherapy if ENE positivity is present but does not require postoperative radiotherapy when ENE is not considered. 17 Moreover, a patient who was determined to be at N1 stage with ENE positivity using old lymph node staging (AJCC, seventh edition) was increased to stage N2a according to the latest staging (AJCC, eighth edition) and a patient who was determined to be at N2 stage with ENE positivity according to the old lymph node staging to N3b according to the new lymph node staging. 4,7 Extranodal extension has been demonstrated to be associated with poor prognosis not only in patients with laryngeal carcinoma but also in patients with oral cavity, oropharynx and hypopharynx carcinomas. 5,16,18 In our study, 2-year OS was 46.2% in patients with detected lymph node metastasis without ENE and decreased to 38.5% in patients with detected lymph node metastasis with ENE. We attributed the fact that there was no statistical difference between the results with the low number of patients.
Greenberg et al divided ENE into 2 groups microscopically as ENE below and above 2 mm in a patient group with tongue cancer and stated there was no statistical difference between the 2 groups. 19 In their study, Barroso Ribeiro et al statistically demonstrated that the more the number of the lymph nodes with ENE is, the lower the OS is. 20
The drawbacks of this study are being a retrospective study, the fact that genetic tumor characteristics were not assessed, the fact that the number of lymph nodes and lymph node localization were not specified, and disease-free survival was not assessed. Long-term follow-up of the patient is very difficult and patients with advanced-stage laryngeal cancer usually delay their health control. Therefore, we did not evaluate the free-disease survival as it would not be the correct evaluation.
Conclusion
Extranodal extension is an important issue that was emphasized in many studies over the years. This study showed the poor prognostic effect of ENE, which is included into lymph node classification in the AJCC, eighth edition, on OS in patients who underwent total laryngectomy and neck dissection in our clinic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.