
Abstract
Nasal polyposis (NP) is characterized by polypoid outgrowths of chronically inflamed respiratory mucosa. The presence of squamous metaplasia and dysplasia on the mucosal surface of nasal polyps (NPs) represents different manifestations of epithelial atypia. The aim of this investigation was to evaluate the presence of epithelial squamous metaplasia and dysplasia in ethmoidal NPs. This retrospective analysis of prospectively collected data involved 212 patients with NP undergoing endoscopic ethmoidectomy. To evaluate possible etiological factors for epithelial atypia, the patients in whom we histopathologically detected the presence of epithelial atypia were compared with patients with “normal” NPs in accordance with the following characteristics as found in the patients’ medical records: gender, age, main symptoms, preoperative extent of sinus disease on computed tomography, atopic status, aspirin sensitivity, cigarette smoking, and occupational exposure to different noxious factors. Epithelial atypia were detected histopathologically in 44 (20.7%) NP patients, whereas features of “true” dysplasia were found in only 1 (0.5%) patient. The presence of atypia was more frequent in males than in females (P = .008). The association with aspirin-exacerbated respiratory disease and with long-term occupational exposure to different noxious chemicals, especially in workers exposed to salts of heavy metals, was more frequent in NP patients with epithelial atypia than in patients without atypia (P = .023; P = .006, respectively). Our results suggest epithelial atypia in NPs are associated with aspirin sensitivity and occupational exposure to different noxious chemicals. Although extremely rare, epithelial dysplasia may occasionally be noted in NPs, a fact potentially useful for both rhinologists and pathologists.
Introduction
Nasal polyps (NPs) are nonneoplastic, chronic inflammatory outgrowths of the respiratory mucosa that usually arise bilaterally from the middle meatus and ethmoid sinus. 1 The polyps are lined by pseudostratified respiratory epithelium. The basement membrane is variably thickened and in some instances has underlying areas of stromal hyalinization. The bulk of the lesion is presented by edematous stroma with fibrosis and inflammatory infiltrate composed of a mixture of eosinophils, lymphocytes, plasma cells, and neutrophils. 2 According to histological studies, inflammatory NPs can be classified into 4 types: edematous or eosinophilic polyps, fibroinflammatory polyps, polyps with hyperplasia of seromucinous glands, and polyps with stromal atypia. 3,4 Cellular atypia in stromal cells of NPs is well recognized as a peculiar response of fibroblasts and fibrohistiocytes to increased intercellular fluid and/or vascular compromise. 3,4 However, there is little information in the literature on the incidence of epithelial atypia in routine nasal polyp specimens. The presence of squamous metaplasia on the mucosal surface of NPs, the so-called “transitional” epithelium, as well as different signs of epithelial dysplasia, including marked basal nuclear atypia with hyperchromasia and suprabasal mitotic figures, are manifestations of epithelial atypia in inflammatory NPs. 5 Possible etiological factors for squamous metaplasia and dysplasia in nasal mucosa are cigarette smoking, environmental ozone, noxious chemicals such as ammonia, benzene, nitrates, and, especially, heavy metals. 5
The aim of this investigation was to evaluate the presence of epithelial squamous metaplasia and dysplasia in NPs of patients with chronic rhinosinusitis with NPs (CRSwNP), the so-called “nasal polyposis” (NP), to assess the potential influence of these forms of epithelial atypia on clinical characteristics, and to evaluate possible etiological factors for the development of epithelial atypia. To our knowledge, this is the first study since 1998 to investigate these questions, and the first one that exclusively investigates the presence of epithelial atypia in surgically excised polyps of patients with ethmoidal NP.
Material and Methods
This observational retrospective analysis of prospectively collected data involved 212 (n = 212) patients (130 males and 82 females) with mean age of 45.22 years, ranging from 18 to 72 years, who were diagnosed with CRSwNP and treated by endoscopic sinus surgery (ESS) between January 2008 and December 2017 in the Department of Otorhinolaryngology and the Institute of Pathology of the Military Medical Academy, Belgrade, Serbia, and was conducted according to the Declaration of Helsinki. The cases of previously nonoperated NP patients were included in consecutive order. The institutional review board approval was obtained from the ethics committee of the Military Medical Academy Faculty of Medicine. Written informed consent was obtained from all individual participants included in the study to use their medical data. All NP patients were treated before surgery by intranasal corticosteroids (fluticasone furoate nasal spray, 110 μg daily, 2 sprays in each nostril in the morning) for 4 months, without success. Other medications, such as oral steroids and antibiotics, were not administered. All patients were preoperatively evaluated for main nasal symptoms (nasal obstruction, rhinorrhea, postnasal discharge, and hyposmia) and for the extent of paranasal sinus disease as assessed by computed tomography (CT) scans of the paranasal sinuses. The findings from CT scans were assessed in accordance with the Lund-Mackay score. 6
The diagnosis of CRSwNP was done according to the guidelines established by the Rhinosinusitis Task Force document, published by the American Academy of Otolaryngology, Head and Neck Surgery, 7 and by the European Position Paper on Rhinosinusitis and Nasal Polyps from 2007 8 and 2012. 9 The exclusion criteria were previous nasal and paranasal sinuses surgery, choanal polyps, respiratory and mesenchymal hamartomas, exophytic and inverted papillomas, other benign and malignant tumors with polypoid appearance, systemic diseases affecting the nose (cystic fibrosis, primary ciliary dyskinesia, Wegener granulomatosis, etc), pediatric patients, and pregnancy.
Histopathological Analysis
A detailed histological analysis of appropriately labeled NP specimens excised during ESS from the middle meatus, anterior and posterior ethmoid, and embedded in paraffin molds, was performed by an experienced pathologist employing the hematoxylin and eosin histopathological technique. Tissue specimens of the NPs were fixed immediately after the surgical excision for 24 hours in 4% buffered formaldehyde solution. Then, the specimens were washed by water and dehydrated by concentrated ethanol (70% up to absolute). They were then lipofilled in xylene and embedded in paraffin. During our investigation, the pathologist who had access to the paraffin molds made the section series of prepared tissue specimens. Paraffin blocks were sectioned at a thickness of 3 to 5 micrometers. The sections were then stained with hematoxylin and eosin. The sections were examined under microscopy to determine the types of epithelial atypia. Two types of epithelial atypia were considered: squamous metaplasia (so-called “transitional” epithelium) and epithelial dysplasia. Metaplasia was defined as a transformation of the type of epithelium, for example, from ciliated columnar to stratified squamous epithelium. Dysplasia was defined as disturbed molding of the layered structure of the stratified squamous epithelium.
To evaluate the possible etiological factors for epithelial atypia, the patients in whom we found the presence of epithelial atypia were compared to patients with “normal” NPs in accordance with their characteristics found in medical data: gender, age, atopic status evaluated by skin prick tests, aspirin sensitivity, cigarette smoking (minimum 10 cigarettes daily for more than 5 years), and occupational exposure to different chemical factors for more than 4 years.
Statistical Analysis
We categorized the patients into different categories (Table 1), and we used the Fisher exact test to determine the statistical significance of the association between the presence of epithelial atypia and factors, such as gender, age, main symptoms, preoperative extent of sinus disease on CT, atopic status, aspirin sensitivity, cigarette smoking, and occupational exposure to different noxious factors. P values < .05 were considered significant. The analysis was done by using the Statistical Package for the Social Sciences, version 15.0 software (SPSS Inc, Chicago).
Possible Etiological Factors in NP Patients With and Without Epithelial Atypia, According to Available Medical Data.
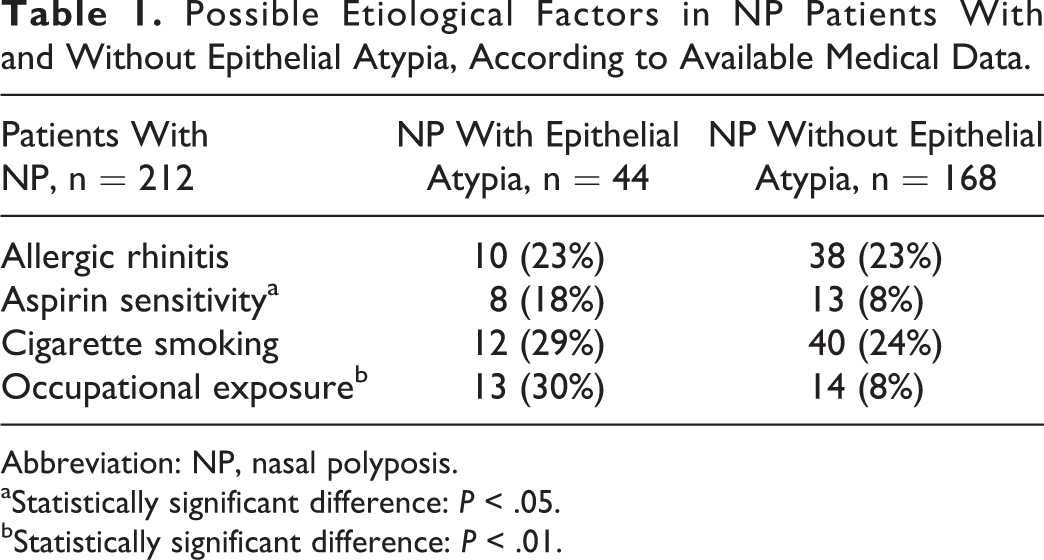
Abbreviation: NP, nasal polyposis.
aStatistically significant difference: P < .05.
bStatistically significant difference: P < .01.
Results
Demographic and clinical characteristics of all patients included in our study are presented in Table 2. Among 212 NP patients, we have detected the histopathological findings of epithelial atypia in 20.7% or 44 patients. The presence of atypia was more frequent in males than in females (P = .008). We found no statistically significant differences between NP patients with and without epithelial atypia regarding age, preoperative frequencies of main nasal symptoms, and the preoperative extent of sinus disease on CT scans.
Demographic and Clinical Characteristics of Patients With NP With and Without Epithelial Atypia.
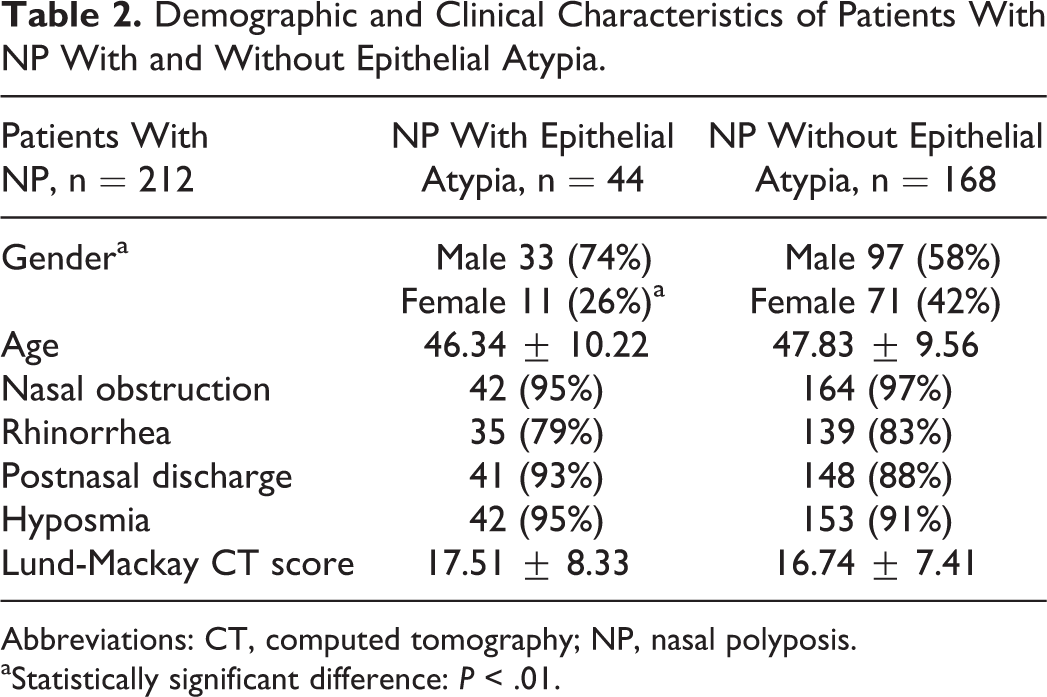
Abbreviations: CT, computed tomography; NP, nasal polyposis.
aStatistically significant difference: P < .01.
Also, no differences were found between smokers and nonsmokers, and between NP patients with and without allergic rhinitis with regard to histopathological findings. The squamous metaplasia of NP epithelium was more prominent, and in 43 patients, the pseudostratified respiratory epithelium (Figure 1) was replaced by stratified, the so-called “transitional” epithelium. However, features of keratinization were not found (Figure 2). The association with aspirin-exacerbated respiratory disease (AERD, aspirin sensitivity) and with long-term occupational exposure to different noxious chemicals was more frequent in NP patients with epithelial atypia than in patients without atypia (P = .023; P = .006, respectively). According to the patients’ medical records, of the 13 NP patients who were exposed to noxious factors through their professions, 3 were woodworkers, 2 were tanners, and 8 were workers employed in copper and nickel metalworking companies. In all workers, the duration of exposure to professional noxious factors was more than 4 years. However, among those patients, we found only 1 case of epithelial dysplasia, the so-called “carcinoma in situ.” So, according to our results, the prevalence of this strong degree of epithelial atypia in NPs is only 0.5%. This was a case of an otherwise healthy 27-year-old man, who had been professionally exposed to copper and nickel salt dust for 6 years. After performing an endoscopic ethmoidectomy on this patient under general anesthesia, the histopathological examination of the removed mass showed inflammatory NPs with edematous stroma and respiratory epithelium. In one of the excised polyps, we found a big area of high stratified squamous epithelium with a rich cellularity (Figure 3A). In this area, the nasal epithelium showed a high level of anisocytosis and hyperchromatosis (Figure 3B). The basal membrane was preserved. The patient recovered well from the surgery and he was well at the time of the follow-up examination 24 months later. Endoscopic examination of the nasal cavity 2 years after the surgical treatment showed no recurrence of lesion. The data on possible etiological factors are presented in the Table 1.
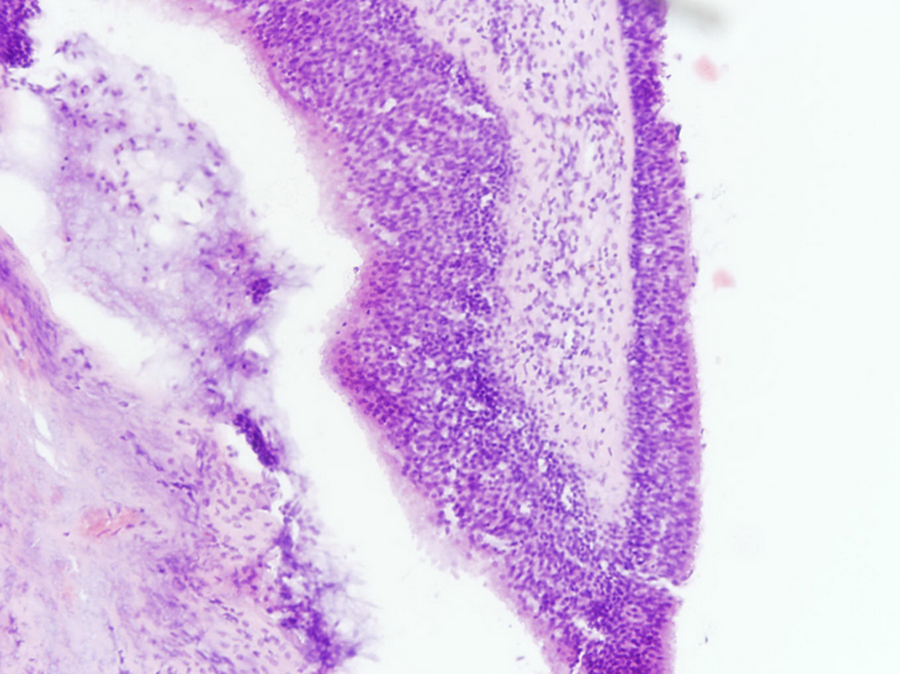
Nasal polyp without epithelial atypia. Note the presence of pseudostratified ciliated respiratory epithelium, stromal edema, and strong inflammatory infiltrate, consisted predominantly of eosinophils and lymphocytes (hematoxylin and eosin stain, magnification ×200).
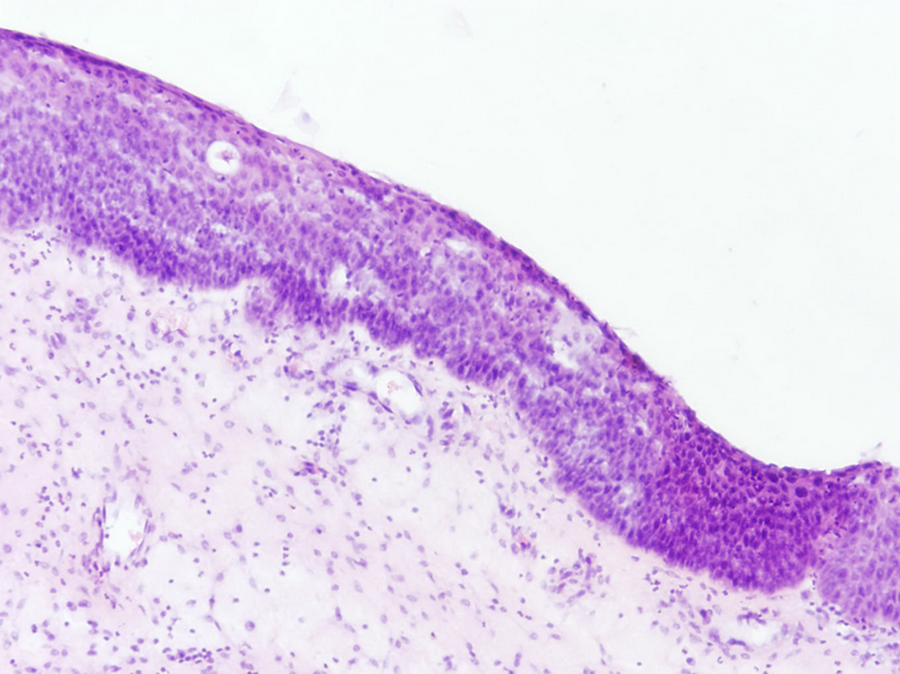
The so-called “transitional” epithelium from the surface of nasal polyp. Pseudostratified columnar epithelium is replaced by stratified epithelium, but features of keratinization are not present (hematoxylin and eosin stain, magnification ×200).
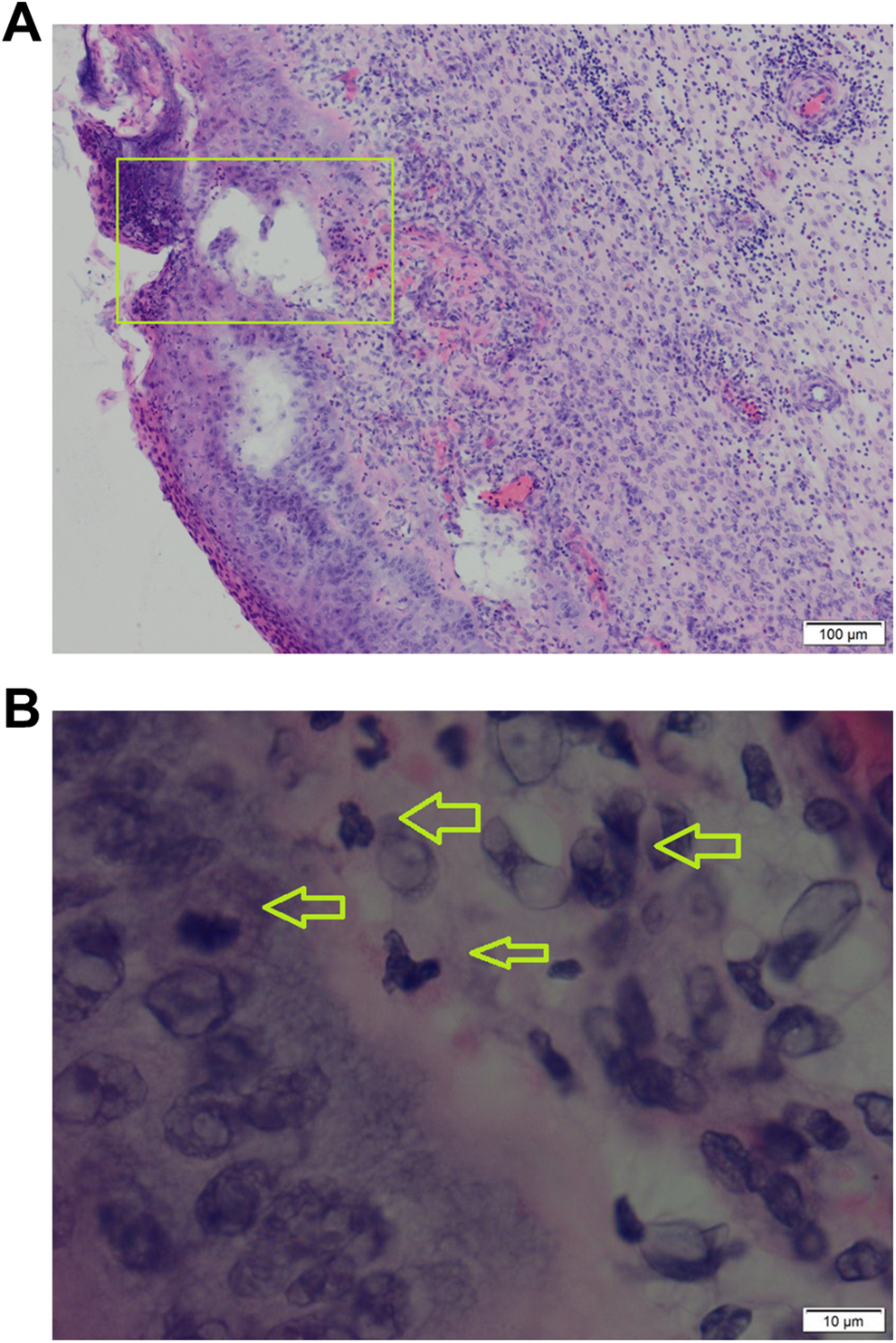
Microphotography showing histopathological feature of epithelial dysplasia. A, Inflammatory nasal polyp with edematous stroma and high metaplastic epithelium with an area of rich cellularity and epithelial basal atypia (inside the rectangle; hematoxylin and eosin staining, magnification ×100), (B) in the area above the basal membrane, the nasal epithelium showing high grade of anisocytosis and hyperchromatosis. The nuclei of atypical epithelial cells are hyperchromatic with marked variability in shape and size (arrow heads). However, the basal membrane is preserved (hematoxylin and eosin staining, magnification ×1000).
Discussion
Nasal polyps are histologically benign inflammatory outgrowths of the nasal and paranasal sinuses mucosa. However, the presence of epithelial atypia in NPs is more frequently seen during the routinely performed histopathological analysis than we think. In spite of that, cases of “true” malignant transformation in inflammatory NPs have not been well-documented in the medical literature. In particular, articles in English regarding the presence of epithelial atypia in NPs are scarce and, to our knowledge, only a few articles on this topic have been published. 5,10 -12 For example, Baird et al 5 found the prevalence of epithelial atypia in NP patients to be 17%, which is comparable with our result of 20.7%. De la Cruz Mera et al 10 found the incidence of 1.17% of carcinoma in situ among 170 cases of NPs. Our results suggest the incidence of epithelial dysplasia of only 0.5%. In our study, the majority of patients with epithelial atypia were male and one explanation for this might be that it is reasonable to expect that men are more likely to suffer occupational exposure to noxious chemicals than women. We found no influence of epithelial atypia on the frequency of main nasal symptoms and clinical severity of NP. We also found no relationship between the presence of epithelial atypia and cigarette smoking, which is in accordance with the results presented by Kule et al. 11 However, Gao et al 12 found that smoking has a strong association with squamous metaplasia in NP in Chinese patients with NP. Although allergic rhinitis can be an etiologic factor in the pathogenesis of NPs, our results showed no association of allergic rhinitis and epithelial atypia. On the other hand, according to our results, the presence of squamous metaplasia is more frequent in NP associated with AERD and in patients with prolonged exposure to various heavy metals, especially nickel and copper. Nasal polyposis as a part of AERD is one of the most severe form of chronic rhinosinusitis, where both the subepithelium and epithelium are strongly affected by toxic mediators released from mast cells and eosinophils during the chronic inflammatory process, especially by leukotrienes and eosinophilic enzymes. 13 Mechanisms for epithelial metaplasia and dysplasia in workers exposed to nickel and copper dust salt are not well investigated. A multitude of factors seems to contribute to the transformation of respiratory nasal epithelium to squamous epithelium. Type of work, number of years since the first nickel exposure, and tobacco consumption are the most important factors. 14 Other extrinsic factors such as temperature, humidity, and dusts of chemical compounds other than nickel in the atmosphere, may be responsible for some of the histopathological changes. 14 The loss of ciliated respiratory epithelial cells and the development of squamous epithelium were regarded as nonspecific histopathological changes. These changes may be essential steps in the development of high-grade epithelial dysplasia and nasal carcinoma. 14 Copper sulfate is the main copper compound mentioned in the toxicological literature. The symptoms produced by inhalation of copper dust are sneezing, cough, swollen mucosa, and epistaxis. 15 Some authors described superficial ulcerations of the nasal septum, deposits of copper dust on the nasal mucosa and slightly hemorrhagic, swollen mucosa of the nasal turbinates. 15 Histological changes included mucosal atrophy with secondary ozena, metaplasia of ciliated epithelium, and degeneration of glandular cells. 15 Interestingly, according to the available literature, all histological changes in the upper airway related to nickel and copper dust inhalation are situated in the nasal epithelium. 13,14 We suggest that precancerous changes may occasionally be noted in inflammatory NPs, especially in workers exposed to heavy metals, a fact that both rhinologists and pathologists should keep in mind.
Our study has some limitations. The medical histories of all patients were retrospectively reviewed and only clinical data regarding the frequencies of main nasal symptoms, association of NP with other conditions (eg, allergic rhinitis, AERD, occupational exposure to different noxious chemicals) and findings from CT scans were available for analysis. We had no data regarding the severity (intensity) of nasal symptoms, assessed by the visual analogue score or Sino-nasal outcome test (eg, SNOT-22), nor data concerning the duration of sinonasal complaints. So, prospectively designed studies concerning the influence of epithelial atypia on clinical characteristics of NP and the potential risk of neoplasia and recurrence of disease after surgery should be conducted in near future.
In conclusion, according to our results, the signs of epithelial atypia were found in 20.7% of patients with NP, but the feature of “true” epithelial dysplasia seems to be an extremely rare histological manifestation in NPs. We found no influence of epithelial atypia on the frequency of main nasal symptoms and clinical severity of NP. Our results suggest possible association of squamous metaplasia in NP epithelium with aspirin sensitivity and occupational exposure to different noxious chemicals, especially in workers exposed to salts of heavy metals. In the future, rhinologists and pathologists should make sure to analyze every surgical specimen of CRSwNP patients. We expect in that case that reports of carcinoma in situ in NPs will be more numerous.
Footnotes
Authors’ Note
The part of this article was presented as a poster at the 27th Congress of the European Rhinologic Society and 37th International Symposium of Infection & Allergy of the Nose, London, United Kingdom; April 22-26, 2018. Presented and awarded at the 2nd Balkan Rhino-Forum (Sinusitis, Skull Base & Rhinoplasty Symposium) in conjunction with 4th Symposium of Rhinology & Allergy Association of Serbia, Belgrade, Serbia; April 4-6, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.