
Abstract

A 6-year-old boy presented with severe dysphonia after hitting his right neck on an opening car trunk about 6 hours earlier. He had no symptoms or signs of dyspnea. Physical examination revealed no neck crepitus, ecchymoses, or tenderness on palpation. Bedside flexible laryngoscopy revealed abnormal appearance and motion of the right arytenoid that could not be characterized further. Computed tomography showed no laryngeal framework injury.
Operative laryngoscopy and bronchoscopy within 24 hours of injury showed partial right arytenoid and glottic mucosal degloving with corniculate and cuneiform cartilage avulsion (Figure 1). The right vocal fold and arytenoid complex were moving symmetrically with the left. The arytenoid joint capsule was exposed. There was no evidence of trauma to the surrounding larynx or hypopharynx. A decision was made not to suture repair the degloved mucosa since it involved only the superior surface of the vocal fold and repair would require suturing to the free edge (medial surface) of the vocal fold, and the thickened, irregular degloved mucosa would have to be stretched over the arytenoid cartilage to suture repair the posterior aspect of the injury. Intravenous steroids, oral antibiotics, and an oral proton pump inhibitor were prescribed for the first 48 hours, 2 weeks, and 1 month after the injury, respectively.
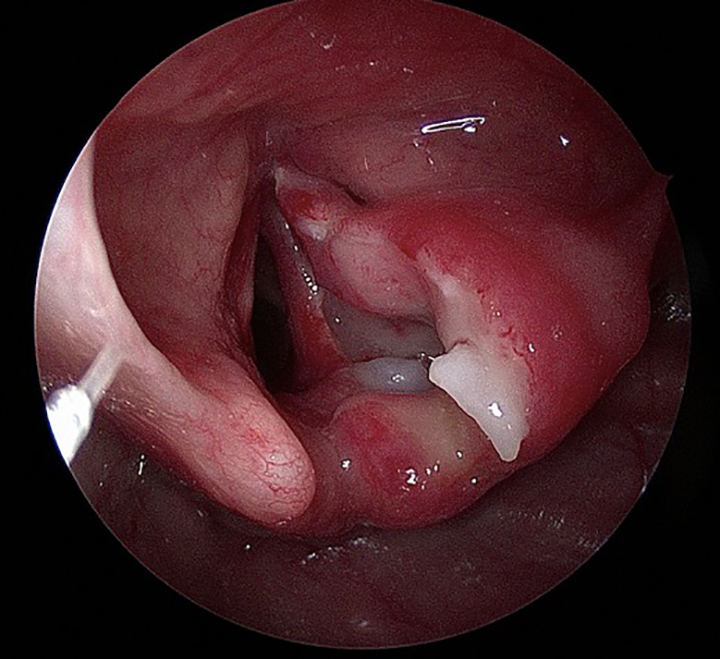
Initial degloving injury with partial exposure of the right arytenoid cartilage and superior surface of the vocal fold with avulsion of the corniculate cartilage.
Over the course of 4 months, his dysphonia resolved while dyspnea with exertion developed. Repeat operative laryngoscopy and bronchoscopy showed partially obstructive granulation tissue formation on the posteromedial area of previous degloving injury (Figure 2). There was continued symmetric movement of the vocal folds and arytenoid complexes. Conservative laser ablation and steroid injection of scar relieved dyspnea and maintained normal voice (Figure 3). During 12 months of follow-up, he had no dyspnea or dysphonia. In office, diagnostic laryngoscopy was performed before and after each operative laryngoscopy. Figure 3 shows an image from his final in-office flexible laryngoscopy. Each operative laryngoscopy was performed using spontaneous ventilation technique with mask ventilation prior to instrumentation. No jet ventilation or intubation was utilized during laryngoscopy and laser ablation.
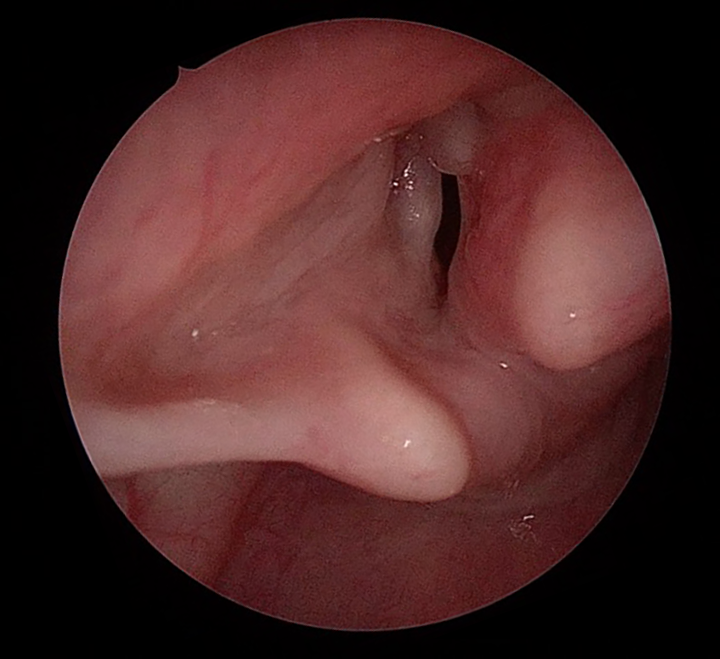
Laryngeal appearance 4 months after the trauma with partially obstructive granulation tissue along the medial surface of the right arytenoid.
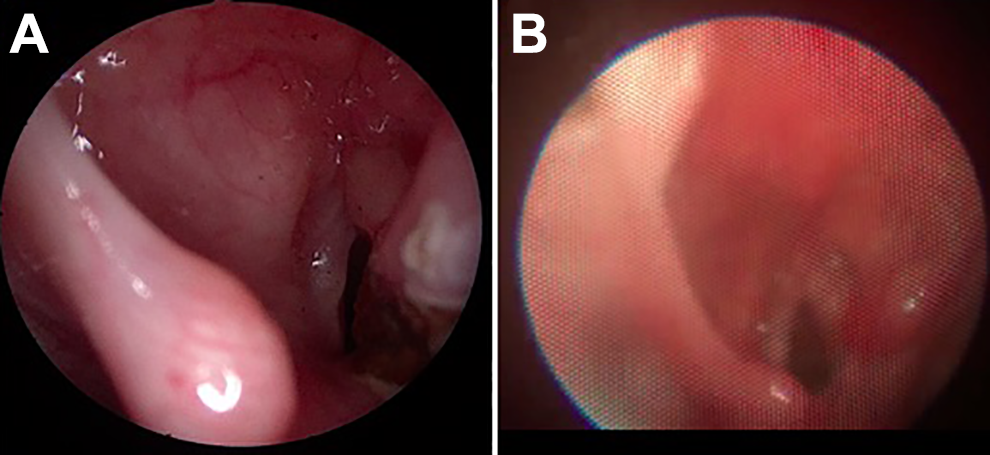
Laryngeal appearance after conservative granulation ablation with carbon dioxide laser. (A) is from the operating room at the time of laser ablation. (B) is from clinic 5 months after laser ablation.
Through this case, we found that primary closure of this arytenoid degloving injury was not necessary for a normal voice outcome. In this case, there was concern that suture repair would have impacted the voice outcome negatively because suturing would have involved the medial surface of the vocal fold and vocal process, while the degloving injury involved only the superior surface of the vocal fold. This is in contrast with the common teaching to primarily suture repair degloving injuries of the larynx. The authors are not suggesting one case should change general practice algorithms; however, we want to contribute this treatment option to the otolaryngologic body of knowledge.
Literature review identified one previous publication on pediatric arytenoid degloving injury. 1 The injury was similar to the case described in this report with similar presentation and outcome but was managed with endoscopic suture repair of the degloved mucosa, which has been described for pediatric vocal fold avulsion injuries, as well. 2 –4
More generally, the adult blunt laryngeal trauma guidelines published by Fuhrman et al include the most frequently cited and used laryngeal trauma classification system. 5 Pediatric-specific algorithms were published by Gold et al in 1997 6 and Cheng et al in 2017. 7 Both Fuhrman and Gold’s algorithms would classify this reports’ patient with grade III injuries and recommend primary surgical repair. A more recent publication notes that some deviation from Gold’s algorithm may be needed depending on the unique details of the case, 8 which this case supports as it presents an ideal voice and breathing outcome without suture repair of a large mucosal laceration with exposed arytenoid cartilage.
Footnotes
Authors’ Note
This research was a poster presentation at the ABEA Meeting; May 1-5, 2019; Austin, TX.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.