
Abstract
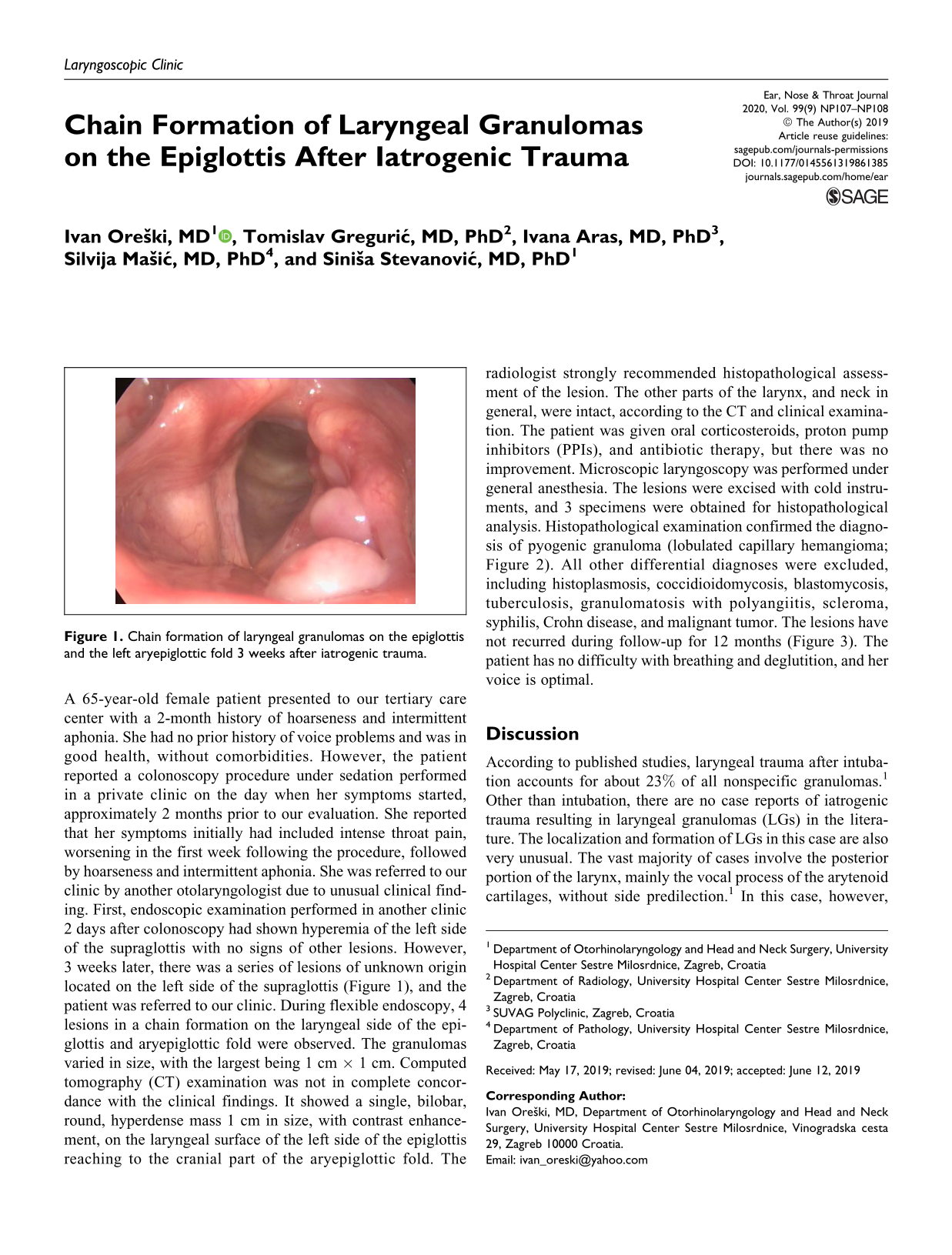
A 65-year-old female patient presented to our tertiary care center with a 2-month history of hoarseness and intermittent aphonia. She had no prior history of voice problems and was in good health, without comorbidities. However, the patient reported a colonoscopy procedure under sedation performed in a private clinic on the day when her symptoms started, approximately 2 months prior to our evaluation. She reported that her symptoms initially had included intense throat pain, worsening in the first week following the procedure, followed by hoarseness and intermittent aphonia. She was referred to our clinic by another otolaryngologist due to unusual clinical finding. First, endoscopic examination performed in another clinic 2 days after colonoscopy had shown hyperemia of the left side of the supraglottis with no signs of other lesions. However, 3 weeks later, there was a series of lesions of unknown origin located on the left side of the supraglottis (Figure 1), and the patient was referred to our clinic. During flexible endoscopy, 4 lesions in a chain formation on the laryngeal side of the epiglottis and aryepiglottic fold were observed. The granulomas varied in size, with the largest being 1 cm × 1 cm. Computed tomography (CT) examination was not in complete concordance with the clinical findings. It showed a single, bilobar, round, hyperdense mass 1 cm in size, with contrast enhancement, on the laryngeal surface of the left side of the epiglottis reaching to the cranial part of the aryepiglottic fold. The radiologist strongly recommended histopathological assessment of the lesion. The other parts of the larynx, and neck in general, were intact, according to the CT and clinical examination. The patient was given oral corticosteroids, proton pump inhibitors (PPIs), and antibiotic therapy, but there was no improvement. Microscopic laryngoscopy was performed under general anesthesia. The lesions were excised with cold instruments, and 3 specimens were obtained for histopathological analysis. Histopathological examination confirmed the diagnosis of pyogenic granuloma (lobulated capillary hemangioma; Figure 2). All other differential diagnoses were excluded, including histoplasmosis, coccidioidomycosis, blastomycosis, tuberculosis, granulomatosis with polyangiitis, scleroma, syphilis, Crohn disease, and malignant tumor. The lesions have not recurred during follow-up for 12 months (Figure 3). The patient has no difficulty with breathing and deglutition, and her voice is optimal.

Chain formation of laryngeal granulomas on the epiglottis and the left aryepiglottic fold 3 weeks after iatrogenic trauma.
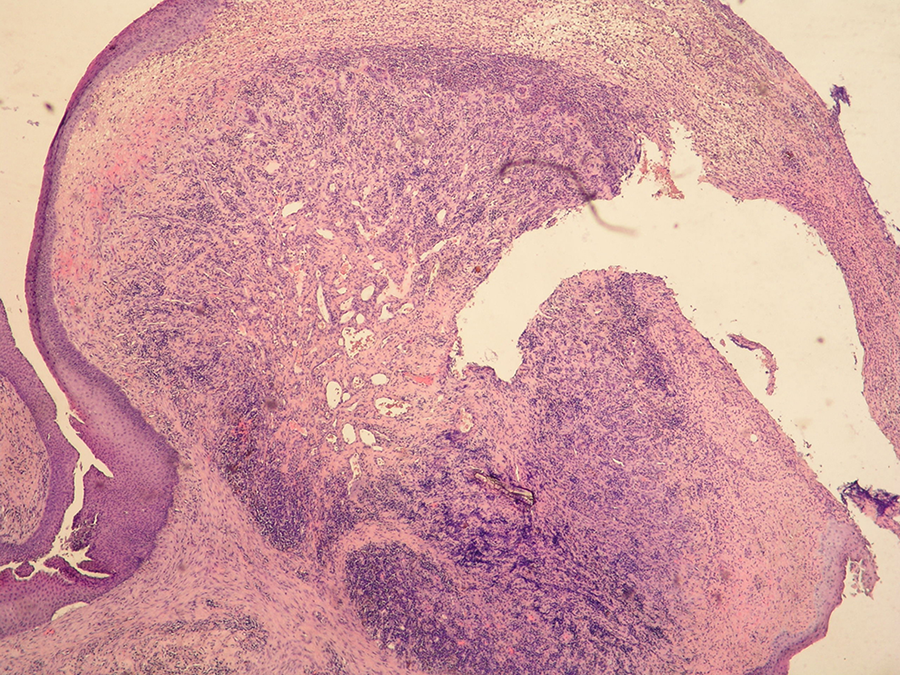
Lesion covered by partially ulcerated acanthotic squamous epithelium and comprised of small vascular spaces lined by normal endothelium, while stroma is focally infiltrated with dense mono- and polymorphonuclears; laryngeal granuloma (HE × 40).
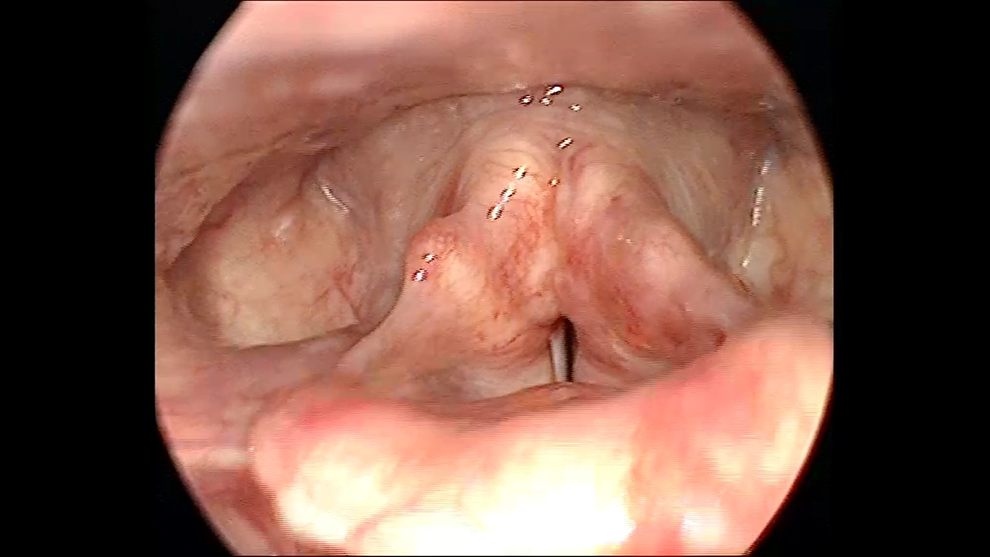
Postoperative finding of a completely normal larynx without traces of laryngeal granuloma.
Discussion
According to published studies, laryngeal trauma after intubation accounts for about 23% of all nonspecific granulomas. 1 Other than intubation, there are no case reports of iatrogenic trauma resulting in laryngeal granulomas (LGs) in the literature. The localization and formation of LGs in this case are also very unusual. The vast majority of cases involve the posterior portion of the larynx, mainly the vocal process of the arytenoid cartilages, without side predilection. 1 In this case, however, there were multiple granulomas in a chain formation located on the laryngeal side of the epiglottis. There is one case with a similar location. However, it involved a 3-year-old child without previous laryngeal trauma and a single lesion on the epiglottis. 2 Yakirevitch et al 3 and Dong et al 4 reported separate cases involving patients with a granuloma localized in the vallecula, but no clear connection with trauma could be made. There are also few cases of pyogenic granuloma located in the lower part of the respiratory tract. 5,6 The current management of the disease is not entirely clear. The majority of authors recommends a conservative approach, with only a 2A recommendation for PPIs. 7 Sometimes, however, as in this case, it is necessary to excise the lesion due to unknown origin and long-term presence of the lesion. This article shows that cases of LG can occur even after mild laryngeal trauma, such as instrument contact during saliva aspiration procedure. Aspiration is practically ubiquitous in modern medicine and occurs during many interventions, such as sedated colonoscopy, transesophageal echocardiography, heart ablation procedures, and many others. Medical professionals should manipulate instruments carefully and monitor sedation and aspiration expertly in order to avoid laryngeal trauma and subsequent LG formation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.