
Abstract
Objectives:
To describe a unique case of isolated bilateral sarcoidosis of the cerebellopontine angle as well as the related imaging in the case. To conduct a literature review of the published articles regarding sarcoidosis of the cerebellopontine angle.
Data Sources:
Representative case report from a single institution as well as PubMed and Scopus database searches.
Methods:
In addition to a retrospective review, all published case reports and case series of sarcoidosis involving the cerebellopontine angle from 1960 to July 2018 in the English language were reviewed. Demographic data, presenting symptoms, and outcomes were collected.
Results:
We identified 8 total cases with pertinent clinical information that were included.
Conclusions:
Isolated neurosarcoidosis of the cerebellopontine angle is an exceptionally rare phenomenon that, on history and imaging, presents similar to more common retrocochlear pathologies. Surgery may be required in large lesions unresponsive to traditional medical therapy with immunosuppression.
Introduction
Sarcoidosis is a chronic systemic granulomatous disease that most commonly affects the lungs but may also manifest in many other organs including the skin, lymph nodes, eyes, and the liver. 1 The prevalence of the disease in the United States is estimated to be between 1 and 40 cases per 100 000 people with African American people being affected 10 times more frequently than caucasians, 2 and women being affected 1.5 times more commonly than men. Nervous system involvement, or neurosarcoidosis, can be seen in 5% to 10% of cases and is usually seen in conjunction with systemic illness. 3 Most often, neurosarcoidosis involves the leptomeninges and cranial nerves. 3,4 Isolated intracranial tumors are a rare occurrence that are seen in less than 1% of patients who have sarcoidosis. 5 We present a case of an elderly woman found to have bilateral enhancing lesions of her cerebellopontine angle (CPA), mimicking vestibular schwannoma and/or meningioma. Unique to this case is the isolated presentation of her disease, without any evidence of systemic illness. Part of this patient’s clinical course with one tumor has been previously published 6 ; however, we present an extension of the report to include the outcome of the contralateral CPA tumor as well.
Methods
A comprehensive literature review of the PubMed and Scopus databases was conducted. The primary objective was to identify all cases of neurosarcoidosis of the CPA from 1985 to 2018 published in the English language. Search terms included “sarcoidosis” and “cerebellopontine angle.” Initial query yielded 21 results, which were then filtered to include articles with relevant clinical information. References of included articles were also screened for potential missed studies. All cases of CPA lesions from neurosarcoidosis were then included and reviewed by the senior authors (S.A.A. and R.M.W.) Any references without pertinent clinical information or cases that did not exhibit neurosarcoidosis of the CPA were excluded.
Case Report
A 62-year-old female presented to an outside emergency department complaining of progressive dizziness, hearing loss, and facial numbness for the past 2 to 3 months. Magnetic resonance imaging (MRI) was performed which showed bilateral tumors within the CPA; thus, she was transferred to a tertiary care academic center for evaluation and management. On physical examination, there were no significant otologic findings and no obvious cranial nerve deficits aside from grossly decreased hearing on the right side. On review of her MRI brain with internal auditory canal protocol, homogeneously enhancing dural-based lesions centered within the CPA were noted bilaterally (Figure 1). The patient’s audiogram revealed a right greater than left sloping high-frequency sensorineural hearing loss with a word recognition score (WRS) of 92% on the right and 96% on the left (Figure 2A). After a multidisciplinary discussion, a recommendation was made for surgical removal of the larger right-sided tumor via a retrosigmoid approach. Surgery progressed uneventfully, with intraoperative pathology favoring meningioma. Her postoperative MRI showed gross total resection of the right-sided tumor (Figure 3A). Interestingly, final pathology revealed noncaseating, non-necrotizing, granulomas with central aggregates of epithelioid histiocytes and surrounding lymphocytes on hematoxylin and eosin stain. These findings were most consistent with a diagnosis of sarcoidosis, and a rheumatology consultation was placed. Diagnostic testing for systemic illness was negative, and the patient was started on prednisone for the treatment of isolated neurosarcoidosis. Four months after surgery, her MRI showed a stable tumor on the left and audiogram showed improved hearing on the right (Figure 2B). The patient’s right facial numbness had resolved as well.
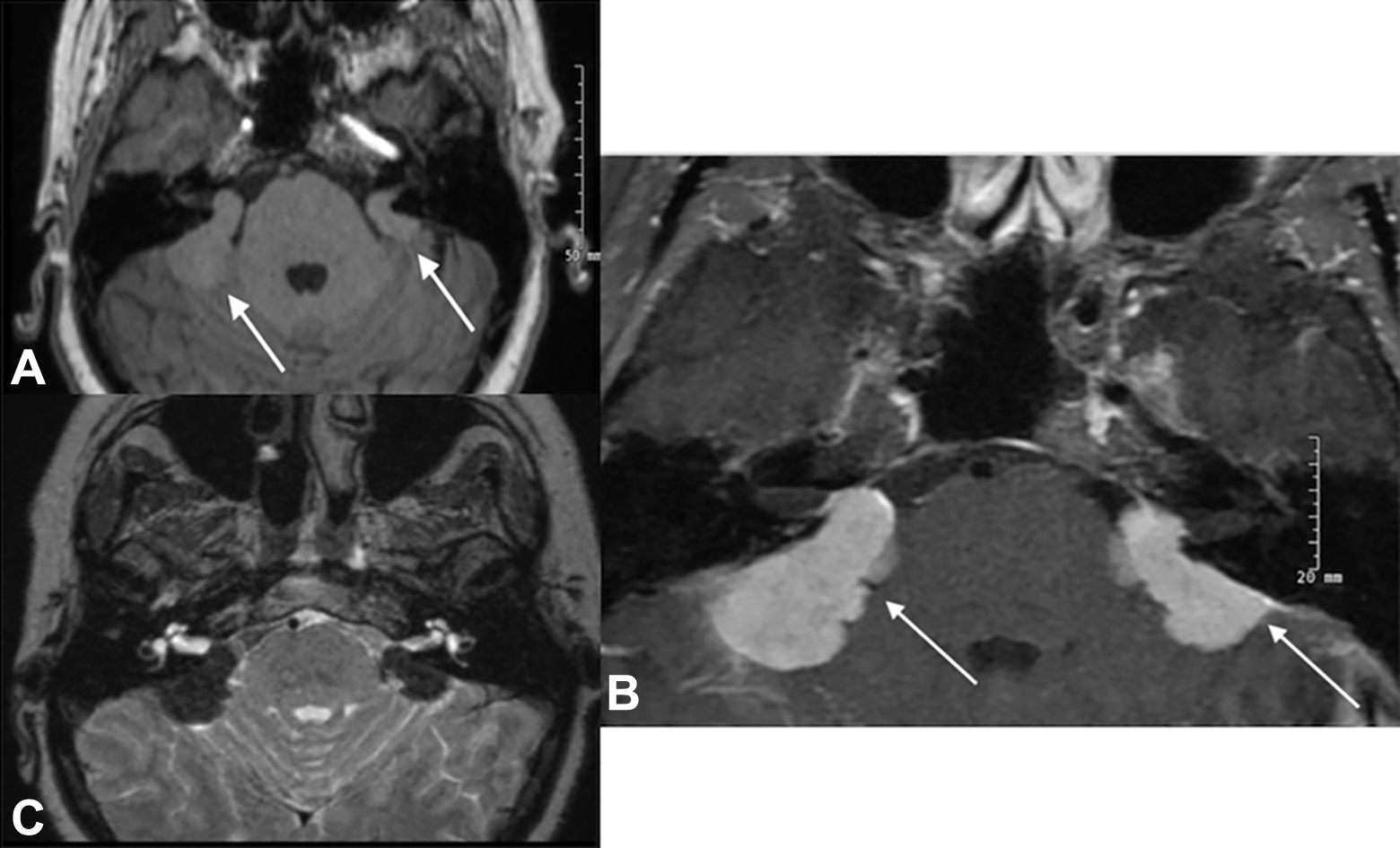
A, Axial T1-weighted precontrast image showing bilateral cerebellopontine angle (CPA) masses (arrows) that are isointense to surrounding grey matter. B, Axial T1-weighted post-contrast image showing avid enhancement of bilateral CPA masses (arrows) each with broad dural attachment to the posterior fossa; the right-sided tumor has a greater degree of involvement of the internal auditory canal. C, Axial T2-weighted image showing these masses as hypointense to surrounding tissue.
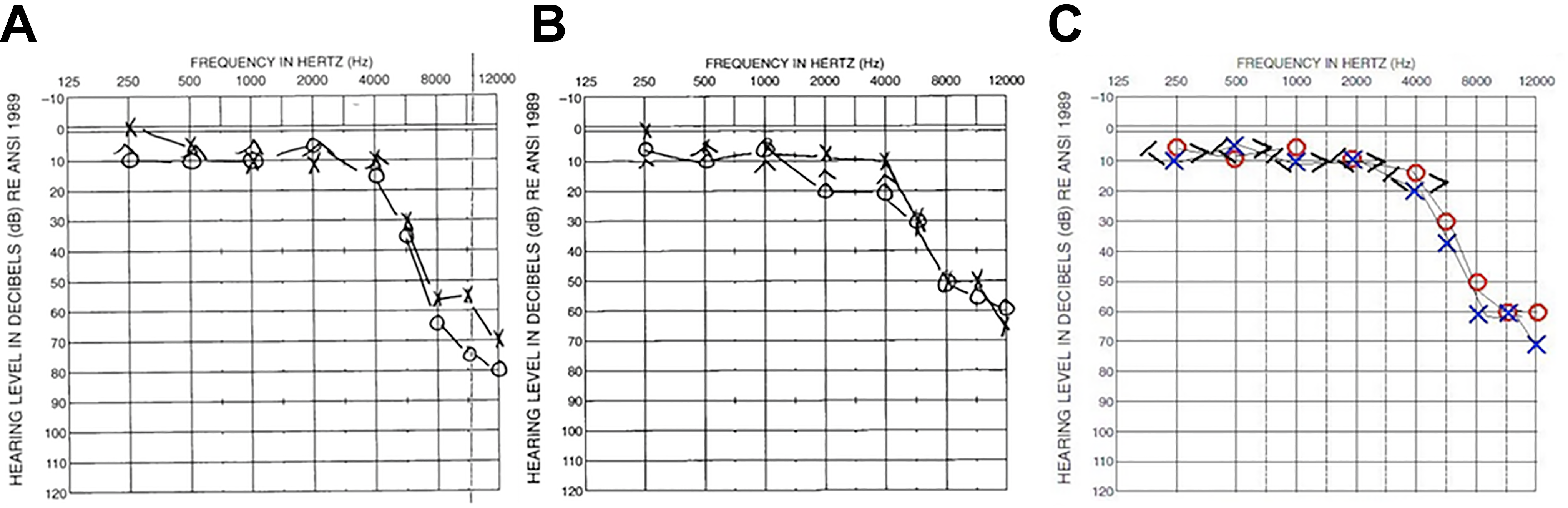
A, Pure tone audiometry prior to initial surgery showing right greater than left severe high-frequency hearing loss. B, Pure tone audiometry after surgery on the right sided, showing 10 to 15 dB improvement in thresholds on the right when compared to previous. C, Pure tone audiometry after surgery on the left side showing essentially stable hearing with a moderately severe high-frequency sensorineural hearing loss.
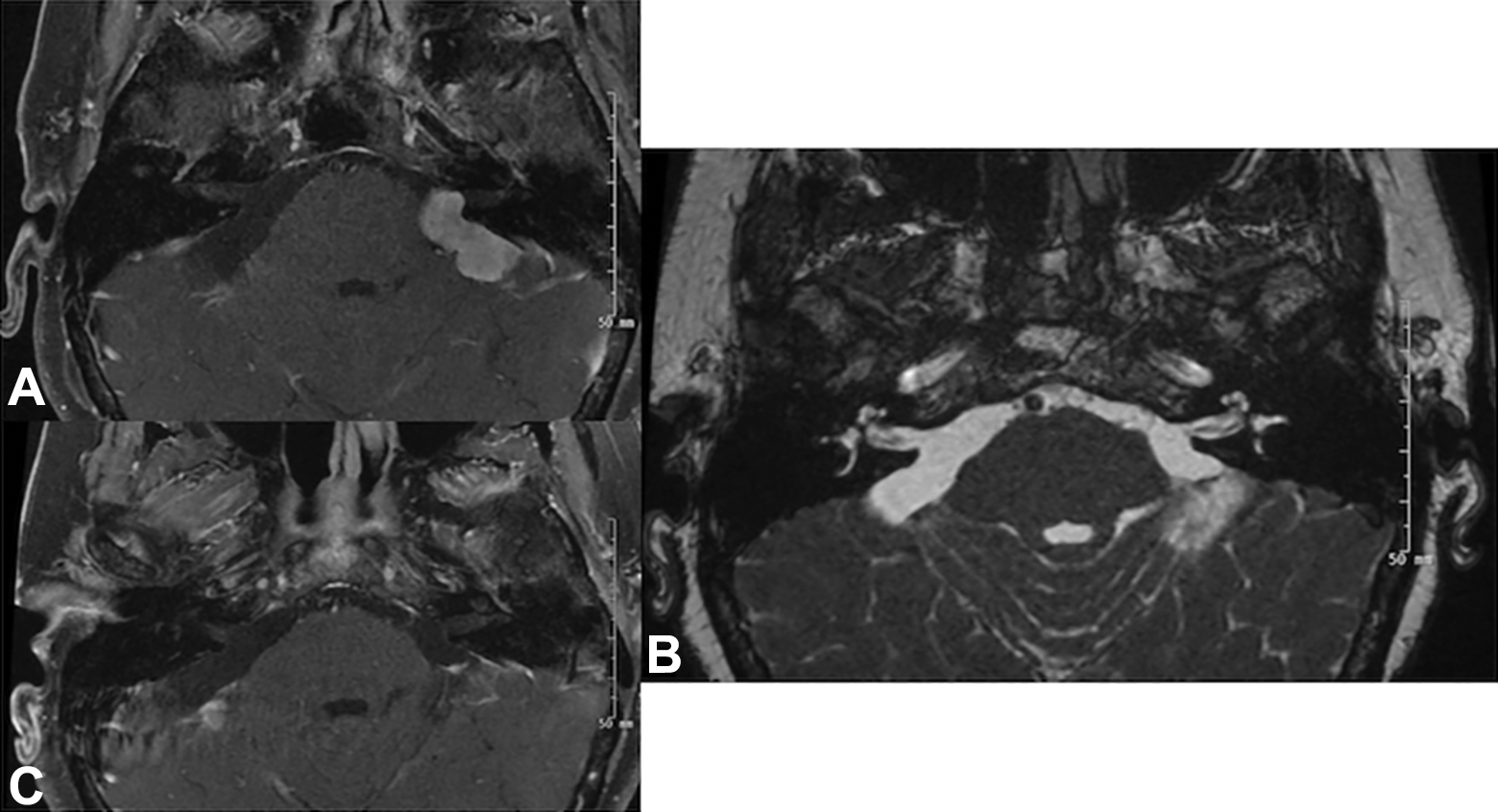
A, Axial T1-weighted magnetic resonance imaging (MRI) with fat suppression and post-contrast showing postoperative changes after resection of the right cerebellopontine angle (CPA) tumor. B, Axial FIESTA sequence showing postoperative changes after removal of both tumors with restoration of bright cerebrospinal fluid (CSF) signal in both spaces. C, Axial T1-weighted fat suppressed post-contrast image after removal of both tumors showing no residual enhancement in either CPA.
To attempt further immunosuppressive therapy in treating her remaining left-sided tumor, the patient was tapered off prednisone and started on azathioprine by rheumatology. In addition, she received 2 doses of rituximab. However, roughly 11 months after her first surgery, the left-sided tumor still had not shrunk in size. The patient complained of continued left-sided facial numbness and dizziness, which persisted despite her first surgery. After thorough consultation with multiple rheumatologists, the patient ultimately requested another surgery, which was also completed successfully through a retrosigmoid approach. Final pathology again revealed neurosarcoidosis. Six months after resection of the left-sided tumor, the patient’s symptoms resolved completely. Her second postoperative audiogram showed slight improvement in hearing thresholds with a WRS of 96% bilaterally (Figure 2C). At most recent follow-up, the patient was doing very well with no subjective hearing loss, dizziness, or facial numbness. Her last MRI is shown in Figure 3B and C.
Literature Review
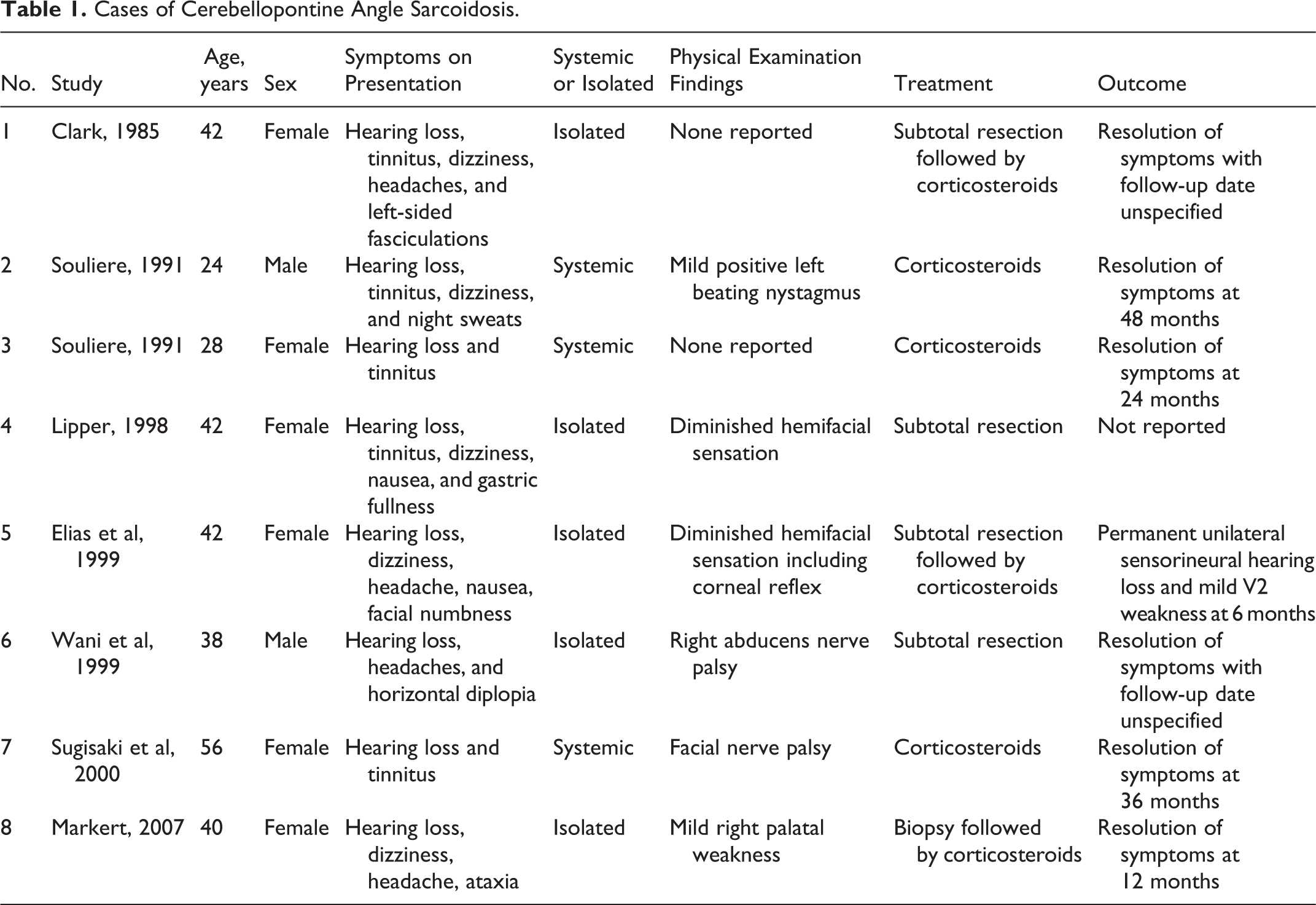
Over the past 33 years, we identified 8 total cases of sarcoid tumors in the CPA. 7 –13 Details of these cases can be seen in Table 1. In line with more common pathologies of the CPA, hearing loss and dizziness were the most common symptoms on presentation. 14 Hearing loss was present in all patients and frequently associated with tinnitus. Other cranial nerve neuropathies were also seen. Cranial nerve neuropathies are considered to be the most common neurologic complication in cases of neurosarcoidosis, and of these, the facial nerve and optic nerve are thought to be most often involved. 3 Facial nerve weakness can be central or peripherally caused. In our review, only 1 patient exhibited a true facial nerve palsy. 12 A more frequent cranial nerve manifestation was hemifacial hypesthesia, which was seen in 2 of the patients. 9,10 The patient in our report also presented with bilateral facial numbness. Tumors of the CPA have been associated with trigeminal neuralgia, which can present as pain and/or hypesthesia. 15 This is explained by compression of the fifth cranial nerve root by the tumor. Decompression, as in the case of our report, can lead to resolution of these symptoms. The majority of cases in our literature review had isolated neurosarcoidosis of the CPA, while 3 cases had evidence of systemic disease.
Cases of Cerebellopontine Angle Sarcoidosis.
Discussion
Definitive diagnosis of neurosarcoidosis requires radiologic evidence coupled with pathologic confirmation. 16 In this case, the imaging on presentation was very similar to what one would expect with classic CPA tumors such as vestibular schwannoma or meningioma. 17 Figure 1A shows an axial T1-weighted image with no contrast, and panel 1B demonstrates the avid enhancement post-contrast administration along with broad attachment to the dura. This is typical for meningioma. Figure 1C shows an axial T2-weighted image that reveals the signal void in the cerebrospinal fluid (CSF) space caused by the bilateral tumors. Dural-based neurosarcoidosis does typically show as dark on T2; however, this can classically also be seen in calcified meningioma. 18,19 Figure 3A and C shows T1 post-contrast images after resection of the right and left sarcoid lesions, respectively. Figure 3B shows an axial FIESTA (fast imaging employing steady-state acquisition) sequence with restoration of normal CSF signal intensity.
Neurosarcoidosis is an uncommon disorder, with only 5% to 10% of all patients with sarcoidosis having some sort of central nervous system involvement. Isolated neurosarcoidosis, that is without any evidence of systemic illness, is even more rare. In a recent series of 166 patients with neurosarcoidosis, only 6 patients showed isolated disease. 20 In patients with a known history of sarcoidosis who develop suggestive neurologic complications, imaging of the central nervous system is vital. Although the rates of estimated antemortem neurosarcoidosis are lower, autopsy results in patients with sarcoidosis can show nervous system involvement in as many as 30% of patients. 21,22
Due to the paucity of the disease, there are no randomized clinical trials regarding the treatment of neurosarcoidosis. Typically, it has been treated similar to the systemic form of sarcoidosis with the use of corticosteroids as first-line therapy. Secondary drugs for unresponsive disease include immunosuppressive medications such as methotrexate and azathioprine and biologic modulators such as rituximab and infliximab. 2,23 In our literature review, all identified cases of CPA sarcoidosis were effectively treated with combination surgery and corticosteroids or steroids alone. Our case showed a contralateral tumor that was unusually refractory to medical therapy with not only steroids but further immunosuppressive medication as well. Thus, we believe that in rare cases of solitary neurosarcoid tumors that are unresponsive to medication therapy, surgical resection can be considered.
The primary focus of this case report and literature review was to demonstrate how rare neurosarcoidosis of the CPA presents and expand the scope of viable treatment options. We found extensive literature of neurosarcoidosis regarding common clinical presentations, imaging findings, diagnostic criteria, and treatment options, particularly the 2015 review of 305 patients by Carlson et al. 5 However, most of these studies did not explicitly report cases of neurosarcoidosis of the CPA and, thus, were excluded from the literature review. The lack of cases supported our efforts to shed light on this uncommon presentation. Also, surgical resection is a possible treatment option in cases of isolated neurosarcoidosis because it has the potential to resolve some, if not all, clinical symptoms as shown in this case report.
Conclusion
Sarcoidosis has often been referred to as “the great imitator” due to the myriad of symptoms a patient may display associated with this disease. Even in neurosarcoidosis, the manifestations can range from solitary parenchymal lesions to involvement of the meninges or even the spinal cord. 20 Although rare, neurosarcoidosis and other granulomatous lesions should remain in the differential for tumors of the CPA, especially in the setting of systemic autoimmune illness. Solitary sarcoid lesions of the CPA may mimic more common pathology on traditional imaging; however, the tumor will show as consistently dark on T2-weighted MRI. Usually, these lesions can be treated with medical therapy, but surgery can be considered for unresponsive tumors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.