
Abstract
Orbital apex syndrome (OAS) is a rare ocular complication following craniomaxillofacial trauma. This traumatic syndrome is a combination of features seen in both superior orbital fissure syndrome and traumatic orbital neuropathy due to nerve impingement. Due in part to the rarity of this disorder, the optimal treatment of traumatic OAS has yet to be determined. We present a case in which traumatic OAS was caused by direct compression due to a displaced fracture segment from the superior orbit. The patient was successfully treated with a combination of emergent decompression and urgent reconstruction suggesting that this may be an effective strategy in OAS resulting from direct nerve compression as a result of craniomaxillofacial fracture.
Case Presentation
A 21-year-old young woman was involved in a motor vehicle collision. She was a seated unrestrained passenger in a horse-driven buggy, which was struck by a motor vehicle. The patient sustained significant craniomaxillofacial injury including an open depressed skull fracture of the frontal bone and depression of the supraorbital rim with violation of dura, and visible brain parenchyma. Physical examination revealed ophthalmoplegia with limited ocular movement of the right orbit and a right relative afferent pupillary defect was noted, particularly on left lateral gaze, suggesting optic nerve impingement. Urgent ophthalmologic consultation revealed that the patient’s visual acuity was 20 out of 100 and intraocular pressure measured 14 mm Hg in the affected eye. Extraocular motility was also limited on the right with decreased superior, lateral, and medial gaze. The patient also had hypoesthesia along the ipsilateral face in the distribution of the ophthalmic and maxillary branches of the trigeminal nerve. Additionally, the patient did not have mobility of her right forehead suggesting injury to the right frontal branch of the facial nerve.
On imaging, it was confirmed that the patient had an open comminuted right frontal skull fracture, comminuted and depressed right supraorbital rim fracture with fracture of the orbital roof, medial orbital wall, and floor blowout. There was evidence of intraorbital displacement of orbital roof bone fragments abutting the optic nerve at the orbital apex. She was also found to have right zygomaticomaxillary, nasoorbitoethmoid, nasal septal, and superolateral anterior and posterior table frontal sinus fractures. Associated intracranial injuries included intraparenchymal hemorrhage with adjacent subdural hematoma. Soft tissue injuries included an 8 cm irregular laceration over the right frontal bone, a 6 mm full thickness laceration through the left nasal soft tissue triangle and a 2 cm right intranasal laceration. She was also found to have a right corneal abrasion. Remarkably, the patient complained only of diplopia.
Following admission to the surgical intensive care unit, a plan was made for a 2-staged procedure. First, an initial bedside washout and debridement of her wounds with closure of lacerations was performed. The following day, after the patient was stabilized and appropriately cleared for surgery from a neurosurgical standpoint, she underwent surgical reconstruction implementing a coronal approach to the frontal sinus and orbit with elevation of a pericranial flap. The superolateral segment of her frontal sinus was fractured through both the anterior and posterior table. However, the nasofrontal recess remained unobstructed and the mucosa of the frontal sinus was intact. The entire orbital roof was comminuted and was therefore removed including multiple segments of displaced bone fragments within the orbit abutting the apex (Figures 1A–D and 2). The right orbital roof and medial wall were reconstructed using a titanium cranial mesh plate in order to provide structural support and mitigate the risk of pulsatile exophthalmos. The dura was repaired and pericranial flap placed. A cranial plate was used to reconstruct the right lateral orbital rim. The supraorbital rim was also reconstructed using an X-shaped cranial plate (Figure 3A-C).
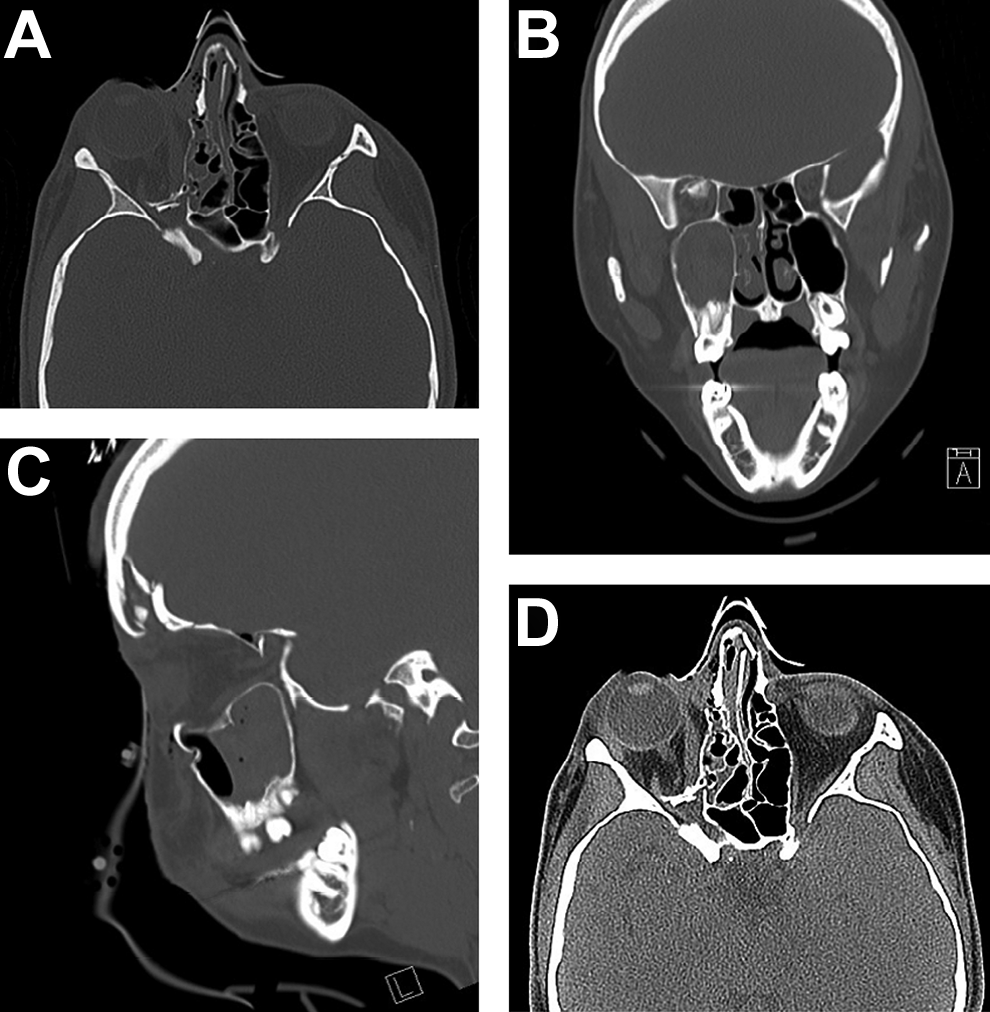
A, Axial CT showing bone fragment within posterior orbital cavity along the course of the optic nerve. B, Coronal CT; Orbital Blow-in fracture with osseous fragment along orbital apex. C, Sagittal CT; Orbital Blow-in fracture with osseous fragment along orbital apex. D, Axial CT soft tissue window displaying area of impingement by the bone fragment along the course of the optic nerve. CT indicates computed tomography.
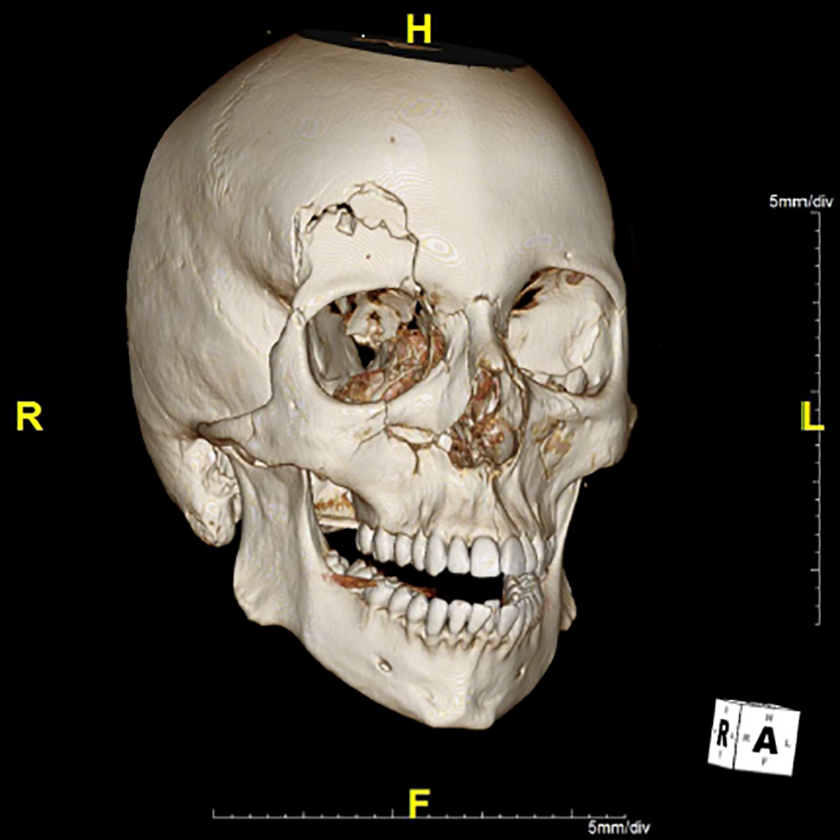
Three-dimensional reconstruction depicting free floating osseous fragment at orbital apex.
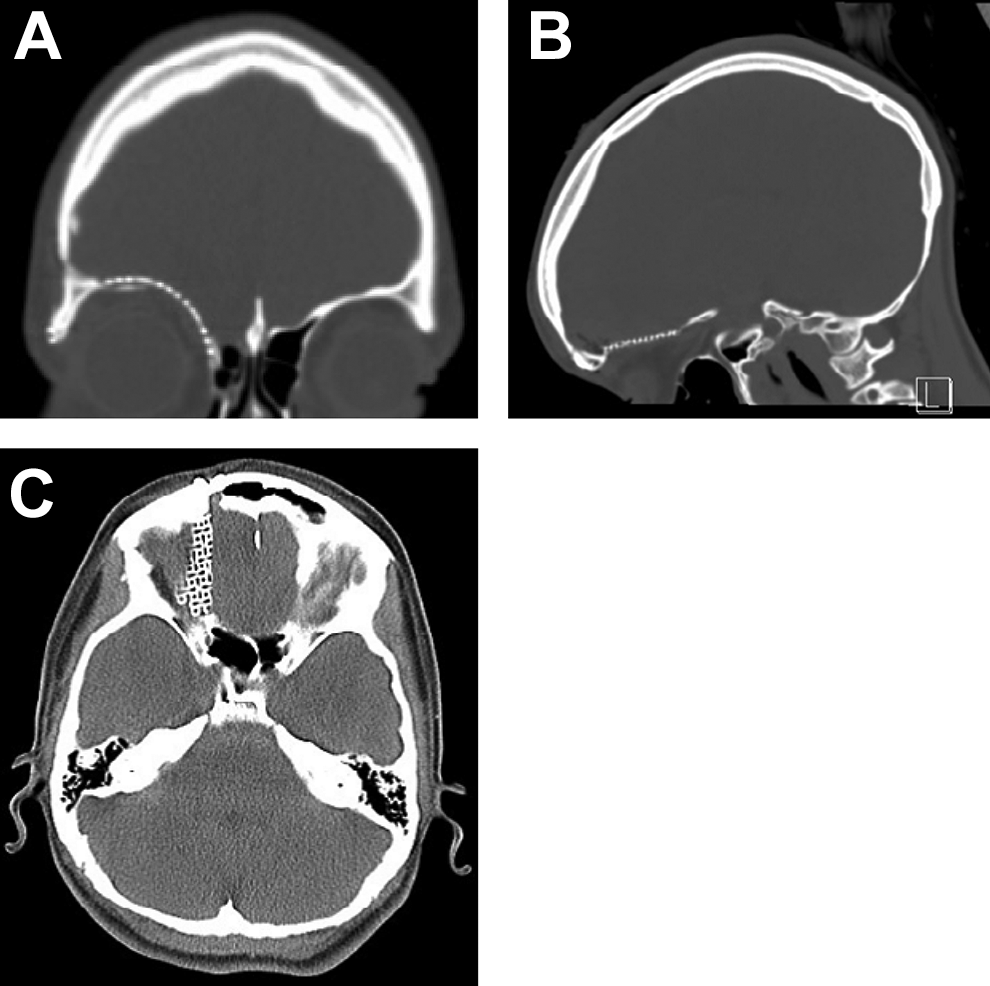
A, Coronal CT following reconstruction of orbital roof. B, Sagittal CT following reconstruction of orbital roof. C, Axial CT soft tissue partially displaying reconstruction of orbital roof in the area of prior nerve impingement. CT indicates computed tomography.
Adjunctive treatment of the patient’s traumatic optic neuropathy also included administration of high dose steroids in the form of 1 g of IV methylprednisolone daily for 3 days. Following surgical intervention, ophthalmologic assessment revealed visual acuity of 20 out of 70, normal intraocular pressure, and return of baseline ocular motility with mild mechanical restriction which was attributed to residual edema.
The patient was subsequently discharged after 6 days of inpatient care and returned in 4 days for further staged repair, as an outpatient, at which time she underwent open reduction and internal fixation of her right depressed zygomaticomaxillary fracture, orbital floor with placement of a porous polyethylene implant, and closed reduction of nasal septal fractures. Outpatient ophthalmology evaluation was approximately 2 weeks from onset of injury revealed subjective improvement in diplopia and overall vision. However, the patient continued to display ptosis of the right upper eyelid and endorsed pain and paresthesia along the ipsilateral forehead and cheek. She showed improvement in her relative afferent pupillary defect as well as improvement in overall eye mobility. She continued to display limitations with respect to down gaze. Two and a half months from her injury, ophthalmologic evaluation indicated that her vision had returned to premorbid baseline (visual acuity 20/20), she had no limitations to ocular movements, and she had regained motion of her forehead with resolution of her blepharoptosis.
Orbital apex syndrome (OAS) is an uncommon, but vision-threatening complication of craniomaxillofacial trauma. The hallmarks of OAS are optic neuropathy, ptosis, numbness along the territory of the ophthalmic branch of the trigeminal nerve and ophthalmoplegia from damage to oculomotor, abducens, and trochlear nerves. 1 –3 Orbital apex syndrome has classically been classified into 1 of 3 subcategories on the basis of anatomical location: superior orbital fissure syndrome (SOFS), and cavernous sinus syndrome, and true OAS. 1 Superior orbital fissure syndrome syndrome involves cranial nerves (CNs) III, IV, and VI as well as the ophthalmic division of CN V without evidence of optic neuropathy; this is the primary differentiating factor with OAS. This syndrome has been documented to occur in both incomplete and complete forms defined by the extent of involvement of CNs entering the orbit through the superior orbital fissure. 4 –6 Structures traversing the superior orbital fissure include the frontal nerve, lacrimal nerve, nasociliary nerve, superior and inferior branches of the oculomotor nerve, abducens nerve, trochlear nerve, and superior ophthalmic vein. 4,5 Damage to these structures may manifest as resultant ophthalmoplegia, ptosis, anesthesia in the distribution of the ophthalmic branch of the trigeminal nerve (V1), or a fixed dilated pupil. In cavernous sinus syndrome, CNs III, IV, VI, maxillary division of CN V (V2), and the oculosympathetic nerves are involved. Involvement of the optic nerve (CN II), resulting in optic neuropathy, differentiates true OAS from SOFS or cavernous sinus syndrome.
Underlying etiologies resulting in OAS include infections, inflammatory disorders, neoplasms, and vascular malformations. 1 Due to the small anatomical size of the orbital apex and confinement of critical neurovascular structures within this limited space, it may be particularly susceptible to injury during trauma. Fortunately, reported cases are rare as demonstrated in the literature. 2,6 –10 In fact, incidence of traumatic SOFS has previously been documented as <1% 2,11 –13 while that of traumatic optic neuropathy has been reported as 1% to 6%. 14 –16 It therefore stands to reason that the incidence of traumatic OAS, the coincidence of both previously mentioned conditions, would be significantly lower than either disorder alone. Due, in part, to this infrequency in occurrence, there has been a paucity of literature defining treatment guidelines for traumatic OAS. 16 –18 Therefore, due to these limitations much is extrapolated from the traumatic optic neuropathy literature.
Traumatic OAS may result from compression of neurovascular structures as a result of direct impingement from an osseous fragment, as reported in our case, or as a result of foreign bodies, hemorrhage, or significant edema. Gossman et al previously classified traumatic optic neuropathy into direct and indirect mechanisms. 18 They defined direct traumatic optic neuropathy as injury to the optic nerve arising from external compression from optic canal fracture, verified by radiologic imaging. Indirect injury was described as optic neuropathy without radiographic evidence of fracture or further evidence of pathology along the course of the nerve. This classification system has implications with regard to treatment and has been applied to SOFS as well. 12,13,18 –20 Injury resulting in direct traumatic optic neuropathy or direct traumatic SOFS should be treated with urgent surgical management. 12,13,16,19 –21 In other words, if there is radiographic evidence of nerve impingement due an osseous fragment, surgical intervention aimed at reducing the bony fragments would be expected to resolve any component of neuropathy attributable to nerve compression and should therefore be performed in an expedited fashion. 22 The time required for irreversible ischemic damage to the optic nerve is variable and dependent on the extent of injury. Therefore, specific timing of intervention remains controversial. However, studies indicate that ischemic changes are seen within 1 hour of injury. 21,22 With this in mind, patients should be evaluated for surgical management in a timely manner. Indirect and direct optic neuropathy are likely not mutually exclusive, particularly in cases of facial trauma, as there is often significant soft tissue edema, hemorrhage, or decreased venous return further exacerbating nerve compression. As such, these indirect causes of neuropathy must be addressed as well. Treatment of indirect optic neuropathy remains controversial. 23,24 Mega-dose steroids, quantities well above common clinical dosages, have been shown to result in progressive improvement of vision if started from time of injury. 16 An intravenous methylprednisolone 30 mg/kg loading dose followed by 5 to 15 mg/kg every 6 hours for 2 to 3 days has been previously reported in the literature with near complete resolution in the majority of patients’ visual symptoms but overall reported regimens vary. 12,16,21,23 Nevertheless, the role of steroids remains controversial. While some reports of improved recovery with concomitant use of steroids and surgical intervention exist other studies have shown no significant difference. 23 We elected to use a mega-dose steroid protocol to address perioperative swelling, as a temporizing measure prior to surgical intervention, as well as postoperatively.
Although, a review of the surgical approaches to the orbital apex are beyond the scope of this article, surgeons must be familiar with both transnasal endoscopic and transcranial approaches. 25 Additionally, as in our case, a multidisciplinary approach involving Ophthalmology, the facial trauma surgeon, and Neurosurgery is often necessary. The majority of reported cases of traumatic optic neuropathy are sustained in the context of sphenoid or orbital roof blow-in fractures. 1,11 These injuries often necessitate combined extra-and trans-cranial approach for appropriate exposure of the orbital apex and allow for complete decompression of the nerve. Although reconstruction may be performed in a single stage, we chose a 2-staged approach in order to allow time for resolution of soft tissue edema permitting reconstruction of the orbital floor and facial fractures without risking exacerbation of indirect optic neuropathy which has been previously documented in the literature if attempts at fracture repair are made too early. 26,27
Our case presentation adds further credence to the primary literature that advocates for timely surgical intervention in cases of direct OAS. As described above, the window of opportunity for successful intervention resulting in near total resolution of visual acuity is small. Blow-in orbital roof fractures that are likely to result in impingement, as a result of displaced bone fragmentation, often impair orbital venous drainage further exacerbating soft tissue edema and impingement of the nerve. 11 Therefore, prompt reduction in fragments with use of perioperative mega-dose steroids should be considered the optimal treatment for traumatic OAS until future large-scale studies are able to further elucidate specific evidence-based treatment parameters.
Traumatic OAS is a rare, but vision-threatening, complication of facial trauma. We report a case of OAS from direct impingement of the optic nerve from an osseous fragment resulting from an orbital roof blow-in fracture. Our patient regained vision in the setting of both timely surgical intervention to reduce bone fragments and use of perioperative mega-dose steroids.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.