
Abstract
The worst complication of cricotracheal resection (CTR) is anastomotic dehiscence, and to limit it, postoperative management at Michigan Medicine included the use of a modified Minerva cervical-thoracic orthosis (MMCTO). To date, there has been no analysis of the risks and benefits of the brace’s use following CTR. We analyze this with our retrospective study. A search with the keywords “cricotracheal resection” and “laryngotracheal reconstruction” was performed in the Electronic Medical Record Search Engine to identify patients retrospectively. The Statistical Package for Social Sciences was used for analysis; t test, χ2, and Fisher exact tests were used to analyze data. Fifteen males and 13 females with a median age of 4 years were identified, and almost 2/3 had a supra- and/or infrahyoid release performed. Postoperatively, 12 had a Grillo stitch and an MMCTO for a mean of 7 days. Most had no complications, but the most common complications were agitation due to brace discomfort and skin irritation. The worst complication was stroke. Our MMCTO’s design allowed for better head and neck control with relative comfortability, and most patients had no complications with its short-term use. Our modification may be useful adjunct in the postoperative management.
Keywords
Introduction
Subglottic stenosis (SGS) can lead to significant airway insufficiency. 1 Depending on the degree of stenosis, inspiratory stridor, dyspnea, or suprasternal and intercostal retractions may present in pediatric patients with mild to moderate SGS. 2 This narrowing occurs within the region inferior to the true vocal folds and superior to the inferior border of the cricoid cartilage, and sometimes may extend to the level of the carina. Stenosis is most commonly acquired secondary to prolonged endotracheal intubation (especially in neonates), congenital abnormalities, trauma, infection, or inflammatory causes. 3,4
Surgical management includes tracheostomy, endoscopic dilation, hot or cold incision, and open surgery with expansion (laryngotracheal reconstruction [LTR] with costal cartilage grafts), cricotracheal resection (CTR), tracheal resection (TR), or slide tracheoplasty. Excessive tension of the anastomosis following CTR and TR may cause anastomotic dehiscence. 3,5 -12 These surgeries are technically challenging and are not the first-line treatments in pediatric patients. 10
Pookamala et al advocate that a lower SGS and tracheal stenosis should be preferentially treated with CTR or TR. 9 To ensure success of the surgery, a Grillo stitch is placed for 1 week postoperatively while the patient is sedated to maintain neck flexion after the resection. However, the stitch does not prevent lateral movements of the neck, and it may irritate the skin or rupture with neck extension. 11 To prevent anastomotic dehiscence, various orthotic devices have been used to maintain neck flexion. Our modified Minerva cervical-thoracic orthosis (MMCTO) has been tailored to maintain middle and lower cervical spine flexion while keeping the upper cervical spine extended. 12 Our retrospective study aims to analyze its use and complications following CTR and TR.
Methods
A search with the keywords “cricotracheal resection” and “laryngotracheal reconstruction” was performed in the Electronic Medical Record Search Engine. From 1992 to 2016, sixty-six patients fitting these criteria were identified. Thirty-one of these patients had either a Grillo Stitch or a MMCTO in place following their operation. The patients’ age at operation, gender, grade of stenosis, type of surgery, the use of Grillo stitch and MMCTO, as well as the length of time used, and complications associated with the MMCTO were gathered.
The data were first extracted into Microsoft Excel for screening and preliminary analysis and then subsequently imported into Statistical Package for Social Sciences version 14 (IBM Corporation, New York, New York) for analysis. Descriptive statistics and Kaplan-Meier survival analysis were used as appropriate. Paired samples t test, χ2, and Fisher exact tests were used and a P value of below .05 was considered significant.
Results
Twenty-eight patients were included in the study. We excluded 2 patients who had their procedure at an outside institution as there was insufficient information and they were unlikely to have used our MMCTO. The median age was 4 years (range: 2 months to 60 years), with 15 males and 13 females.
The majority of these patients had grade 3 SGS (n = 19; 67.9%), followed by grade 4 (n = 6; 21.4%) and grade 1 (n = 3; 10.7%). Four (14.3%) patients had previous open-airway surgeries. Of the patients examined, 5 had CTR with an intrathoracic release, 8 had CTR with a hilar release, 3 had CTR with a suprahyoid release, 1 had CTR with a hyoid release, 1 had CTR with a hypoid muscle release, and 5 had CTR without a release. Additionally, 3 patients underwent LTR without a release.
Only the senior author of this report uses the Grillo stitch at our institution. Twelve (42.9%) patients had both a Grillo stitch and MMCTO in place in the initial postoperative period, and 6 (21.5%) patients had a Grillo stitch only. The median time in situ with the stitch was 7 days (range: 0-12 days). Over half of the patients (n = 16, 57.1%) had the MMCTO stay on for a median time of 7 days (range: 0-16 days).
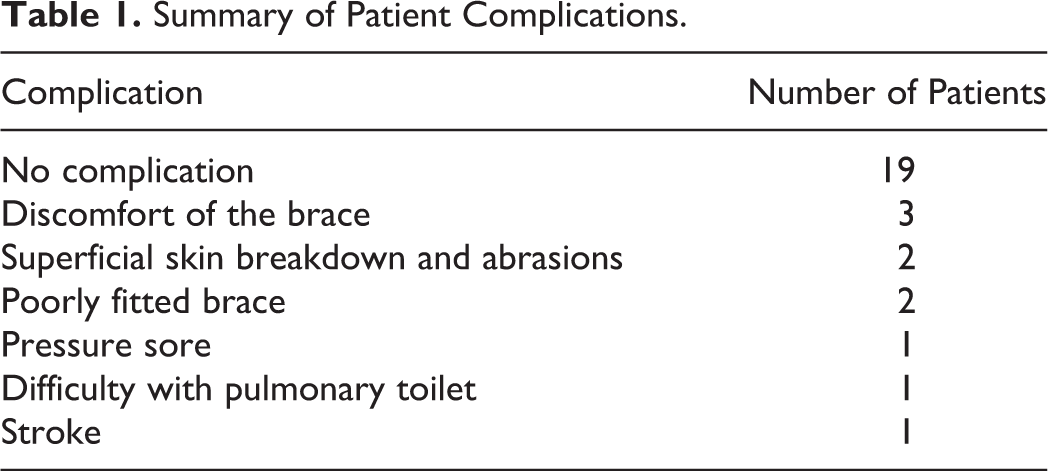
Most (n = 19, 67.9%) patients had no complications. The most common complications were discomfort of the brace, reported in 3 (10.7%) patients, followed by superficial skin breakdown and abrasions with a poorly fitted brace (7.1%). Other rarer reported complications included pressure sores, difficulty with pulmonary toilet, and stroke (3.6% in each category). All these complications were seen in patients with both Grillo stitch and MMCTO applications, except in one patient with MMCTO only who had discomfort. These complications are illustrated in Table 1.
Summary of Patient Complications.
A younger age was significantly correlated with the presence of complications, t(27) = 3.64, P = .001. Gender was also significantly correlated with the presence of complications (Fisher P = .016). There were 8 males with complications compared to 1 female. However, our sample size is small and this needs to be interpreted with caution. The presence of brace use (Fisher P = .003) and the length of time in the brace, t(27) = 5.37, P = .000, were also significantly correlated with the presence of complications, as was the length in time the stitch was present, t(27) = 6.53, P = .000. In addition, the grade of stenosis was also significantly correlated with the presence of complications, t(27) = −13.89, P = .000.
Discussion
The MMCTO maintains flexion of the cervical spine to reduce tension on the anastomosis following TR and CTR. It controls motion through the adjustable occipital support and headband strap, which prevent neck mobility and allow for custom fitting both preoperatively and postoperatively. Additionally, the modular components allow for the angle of cervical flexion and length of the orthosis to be changed with relative ease. The open design of the orthosis also permits examination of wounds and sutures, so that health-care providers may assess the healing process.
The MMCTO consists of anterior and posterior plastic sections, an occipital extension, and a series of straps. The mandibular extension of the traditional Minerva is removed. The presence of the manubrial–mandibular suture and small dimensions of our pediatric patients leaves little space for a rigid support under the mandible.
The anterior plastic piece is shortened and narrowed to fit inferior to the surgical site and stitch. It houses chafes for the straps which keep the child centered in the orthosis. The perineal strap prevents the orthosis from migrating superiorly on the patient. The straps can be made from VelfoamÒ (Alimed, Dedham, Massachusetts), a soft material that can rest directly against the skin.
The posterior plastic piece extends the lever arm of the orthosis to the lower thoracic level. The aluminum occipital extension is contoured to hold the neck in 0 to 20 degrees of flexion, as indicated on a case-by-case basis according to the length of resection and tension on the anastomosis. The forehead strap originates and fastens on the occipital piece to keep the head centered in the orthosis.
At our institution, the postoperative protocol includes sedation, intubation, and MMCTO. The orthosis is customized and applied immediately postoperatively. Patients are kept intubated and sedated in the pediatric intensive care unit for the first postoperative week. They are then taken to the operating room for direct laryngoscopy and bronchoscopy (DLB), removal of sutures and drains, and trial of extubation. Depending on the healing of the anastomosis seen on DLB, it is worn full time for a further 7 to 10 days.
The rigidity of an orthosis against bony prominences can lead to increased skin pressure that can surpass the maximum capillary pressure of skin, resulting in pressure ulcers. 13 These localized injuries to the skin and/or underlying tissue usually occur over a bony prominence due to shear, and if left, could necrose. 14 Only one patient developed an occipital pressure sore (stage 1), which formed 9 days after the MMCTO was fitted. Wound care was initiated and continued for 8 days, but by virtue of the superficial nature of the sore, no complications resulted. Pressure sore development was prevented by utilizing foam padding (Figure 1) underneath the brace and through the usage of soft straps, intensive monitoring, and regular nursing assessment and care.

Padding placed behind the occipital portion of the modified Minerva cervical-thoracic orthosis (MMCTO).
As for agitation due to the discomfort of the brace, 3 occurrences were reported. They all took place after the initial period following extubation. This may have been in part due to the withdrawal of sedatives, or due to confusion following a prolonged period of sedation, but they all resolved within 4 days.
Issues regarding the fit of the brace occurred in 2 patients. One patient’s cranial strap was not fitted properly, and as a result, the patient underwent undesired extending motions. A new MMCTO was then fitted 3 days later with a better fitting cranial band to discourage extension with the buckling motion. The second patient had his cranial strap bow down to his eyes, but this was promptly resolved in one day. In another patient, skin abrasions appeared superficially and minimally both on the right forehead and right chest, but both completely healed within 2 weeks.
The rarest and most devastating complication of a stroke due to the neck flexion occurred in one of our patients. Unfortunately, cervical manipulation therapy, including rotation, extension, lateral flexion, and nonforce and neutral position, has been linked to occasional spinal ischemia. 15 These ischemic events are often random, and therefore, difficult to predict. Our patient was noted to have no voluntary movements in addition to minimal respiratory efforts despite being weaned off sedation. It is uncertain if this occurred intraoperatively or in the postoperative period as he was sedated the entire time. Whether the injury occurred solely as a result of the position in the orthosis is difficult to determine; however, it is imperative to verify the angle of cervical flexion throughout the postoperative period. Use of additional pillows to bolster the head and neck under the orthosis should be avoided.
Difficulty with pulmonary toileting occurred in only one patient. However, this was not directly due to the brace itself, but rather due to the sedation resulting in atelectasis and increased pulmonary secretions. These are associated with a decrease in respiratory status overnight, requiring increased ventilatory settings. Complications of Grillo stitch were relatively minor including erythema and skin breakdown from tension of the stitch on skin potentially resulting in local infection. The stitch did not prevent lateral rotation.
Other orthoses were described to maintain cervical flexion postoperatively: the Halo orthosis, Aspen collar, Philadelphia brace, and Shiraz brace. Each of these reduced sagittal plane translations during flexion and extension, but the Minerva and Halo have been found to inhibit neck movements more efficiently. 16 We prefer our modified Minerva design over the more invasive Halo brace as it allowed for a greater ease of adjustment while also circumventing issues associated with halo pins: such as loosening, infections, and cerebral spinal fluid leaks. 17
Braces with chin and occipital support have a theoretical aspiration risk with limited oral range of motion, increased head elevation, or inhibited laryngeal movement during swallowing. 12 Swallowing function should therefore be assessed preoperatively.
Limitations of the Minerva design include soiling of the straps, as they rest directly over the skin. Thus, meticulous skin care is critical to prevent skin breakdown. Low-grade fever, transient hoarseness, and stiffness of facial muscles were reported to be related to Minerva use 12 ; however, we did not observe these in our series.
One challenge in the usage of these braces postoperatively is that the patients are sedated, so they are unable to give feedback on pain or discomfort. It is crucial that the care team monitor the fit of the orthosis throughout the entire course of wear time and not just in the initial fitting period. Patients can shift in bed due to various procedures, pressure relief, and so on. Proper positioning of the orthosis is crucial to ensure that the contours of the plastic lineup with the anatomical structures to avoid complications.
A major limitation of our study was the fact that it is retrospective in nature. There might be bias associated with inadequate documentation in the medical record or misclassification. With the relatively small sample size, our data do not completely encapsulate all complications associated with the brace’s use.
Conclusion
The MMCTO may be used to control cervical position following CTR and TR to ensure that disruption of the postoperative anastomosis does not occur. In our series, most patients had zero to minor complications, and it is a preferred alternative to other orthoses. However, it is important to be aware of these complications in order to prevent them.
Footnotes
Authors’ Note
Presented at the 120th Annual Meeting at COSM; April 28-29, 2017; San Diego, CA.
Acknowledgments
The authors thank Eric Broekuizen for a brace forming demonstration. Our patient for being a willing model for the brace.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.