
Abstract

A 45-year-old man presented with progressive left nasal obstruction and recurrent epistaxis for several weeks. At our clinic, sinoscopy showed a reddish soft tissue tumor in the left nasal floor (Figure 1). The computed tomography of the sinuses showed a soft tissue mass in the lower left nasal floor without definite bony erosion (Figure 2).
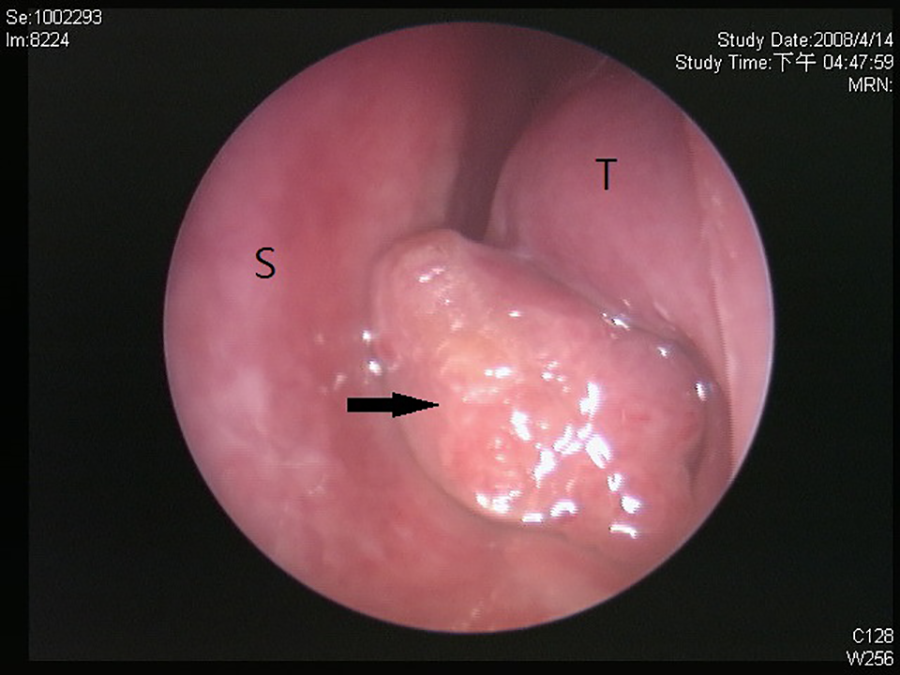
Sinoscopy showed a reddish soft tissue tumor (black arrow) in left nasal cavity, occupying the entire inferior meatus and the majority of the common meatus. S: left nasal septum. T: left inferior turbinate.
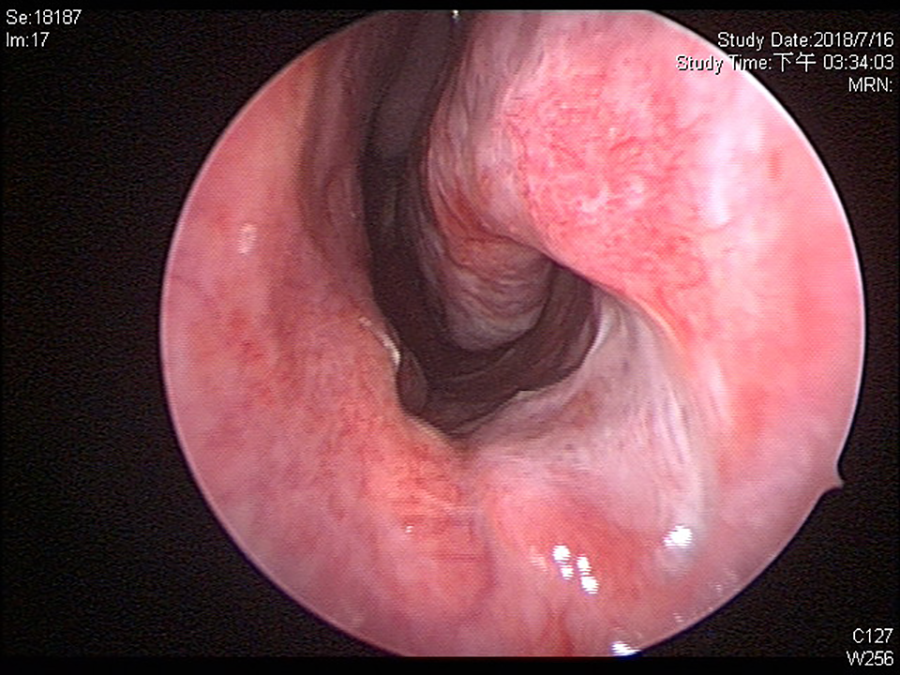
A follow-up sinoscopy revealed no recurrence 11 years after surgery.
Endoscopic resection of the tumor originating from the anterior portion of the left nasal floor was smoothly performed. There were no complications noted after surgery. The size of the tumor was 2.0 × 1.0 × 1.0 cm3. The pathological study revealed sinonasal angioleiomyoma (also known as vascular leiomyoma) with hypocellular growth of blended smooth muscle cells around venous vessels. The immunohistochemical stain showed desmin and smooth muscle actin positive which confirmed the diagnosis of leiomyoma. There was no recurrence during the 11-year follow-up.
Leiomyomas occur most commonly in the uterus (95%), followed by the skin (3%), and the gastrointestinal tract (1.5%). They are rare (less than 1%) in the head and neck areas and are especially rare in the sinonasal cavity. The first sinonasal leiomyoma case was reported in 1996. 1 Since then, only about 50 cases of sinonasal leiomyoma were described in the literature. The reported cases of sinonasal leiomyoma were in the inferior turbinate, followed by the septum. Our patient could be the first case of leiomyoma in the left nasal floor.
Leiomyoma in the sinonasal area was usually female predominant, and the female to male ratio was about 2:1. 2 The symptoms were usually nonspecific and characterized by nasal obstruction, recurrent epistaxis, and nasal discharge. These symptoms were caused by mass effect–related airflow changes that caused nasal crusting and nasal desiccation. 3
The most acceptable treatment was complete surgical excision with adequate surgical margin. The surgical methods depended on the size, location, and the extension of the tumor. In most cases, transnasal endoscopic excision could be performed successfully. For those in certain sites or larger and more extended tumors, transpalatal, Caldwell-Luc, lateral rhinotomy, external ethmoidotomy with medial maxillectomy, or craniofacial resection could be other possible treatment choices. 3,4
The prognosis of angioleiomyoma was favorable. No malignant transformation case has been published to date. 5 If the angioleiomyoma could be completely resected during surgery, recurrence was unlikely to happen. Our case has more than 11 years of follow-up, and there is no evidence of recurrence after completed transnasal endoscopic resection.
Footnotes
Authors’ Note
Ethics committee approval was obtained from the institutional review board and ethics committee at the Chang Gung Memorial Hospital, Taiwan.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Hsin-Ching Lin received research grants from Intuitive Surgical Inc., Sunnyvale, CA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.