
Abstract
Objective:
To determine whether surgical case volume is a predictive factor of surgical outcomes when managing geriatric patients with head andneck cancer.
Methods:
A cross-sectional study design was used. Data were obtainedfrom the Vizient Database, which included a total of 93 academicinstitutions. Men and women aged between 65 and 100 years undergoing head and neck cancer surgery during 2009 and 2012,excluding cases of thyroid cancer and skin cancer of the head and neck(n = 4544) were included in the study. Hospital case volume was definedas low (≤21 cases/year), moderate (22-49 cases/year), or high (≥50 cases/year). The frequency of comorbidities and complications wasmeasured by hospital case volume using a χ2 test. Significancewas determined with an α level of .05.
Results:
The largest number of head and neck cancer cases involving comorbidities (90.54%) and the highest rate of overall complications(27.50%) occurred in moderate case volume institutions compared to athe complication rate of 22.89% in low volume hospitals and 21.50% in highvolume hospitals (P < .0001). The most common comorbidities across all3 hospital case volumes included hypertension, metastatic cancer,and chronic pulmonary disease and the most common complicationsincluded hemorrhage/hematoma and postoperative pulmonarycompromise.
Conclusion:
With more geriatric patients requiring surgery for head andneck cancer, it would be beneficial to manage the more complex cases at high volume centers and to develop multidisciplinary teams to optimizecase management and minimize complications.
Introduction
In the United States, the elderly population (aged 65 and older) comprises approximately 14.5% of the population or 46 243 211 people. 1 Even more significantly, this age group is expected to experience an increase of 205% by the year 2060. 2 Logically, the number of head and neck cancer cases will have a concurrent increase and thus require the management of a well-coordinated multidisciplinary team. Several studies have described the relative safety of anesthetics and surgery in the elderly patient population. 3 -5 Additionally, multiple studies have looked at complications and comorbidities in the geriatric population receiving head and neck surgery. 6 -10
It has been suggested that case volume is inversely related to complication rates for specific types of surgery. 11 -16 However, few studies look at complications and comorbidities in the geriatric population receiving head and neck surgery based on case volume. 17,18 Geriatric patients experience different physiological processes as they age, and the risk of surgical complications must be balanced against the functional and potential life-saving benefits gained by oncologic surgery. 19 There have also been studies that describe comorbidities and performance status as a predictor of whether curative treatment was provided, overall survival, and quality of life. 20,21 Therefore, this study was conducted to determine whether there is a difference in comorbidities and complications at a national level in the geriatric population receiving head and neck cancer based on hospital case volume.
Patients and Methods
Vizient Database
Prior to the initiation of any research, institutional review board approval at the Boston University Medical Center was obtained. Approximately 90% of the academic medical centers (93 academic medical centers) in the United States contribute to the Vizient (formerly University HealthSystems Consortium) clinical database/resource manager (CDB/RM) making this an appropriate generalized database for academic medical centers. 22 Members have access to discharge data allowing hospitals to compare clinical performance. These data are collected on patient-level UB-04 billing forms, which is a form approved by the Centers for Medicare and Medicaid Services to collect patient discharge diagnoses and billing data. The database includes variables such as age, race, sex, comorbidities, length of stay, mortality, readmission rates, cost, and complication rates. 11
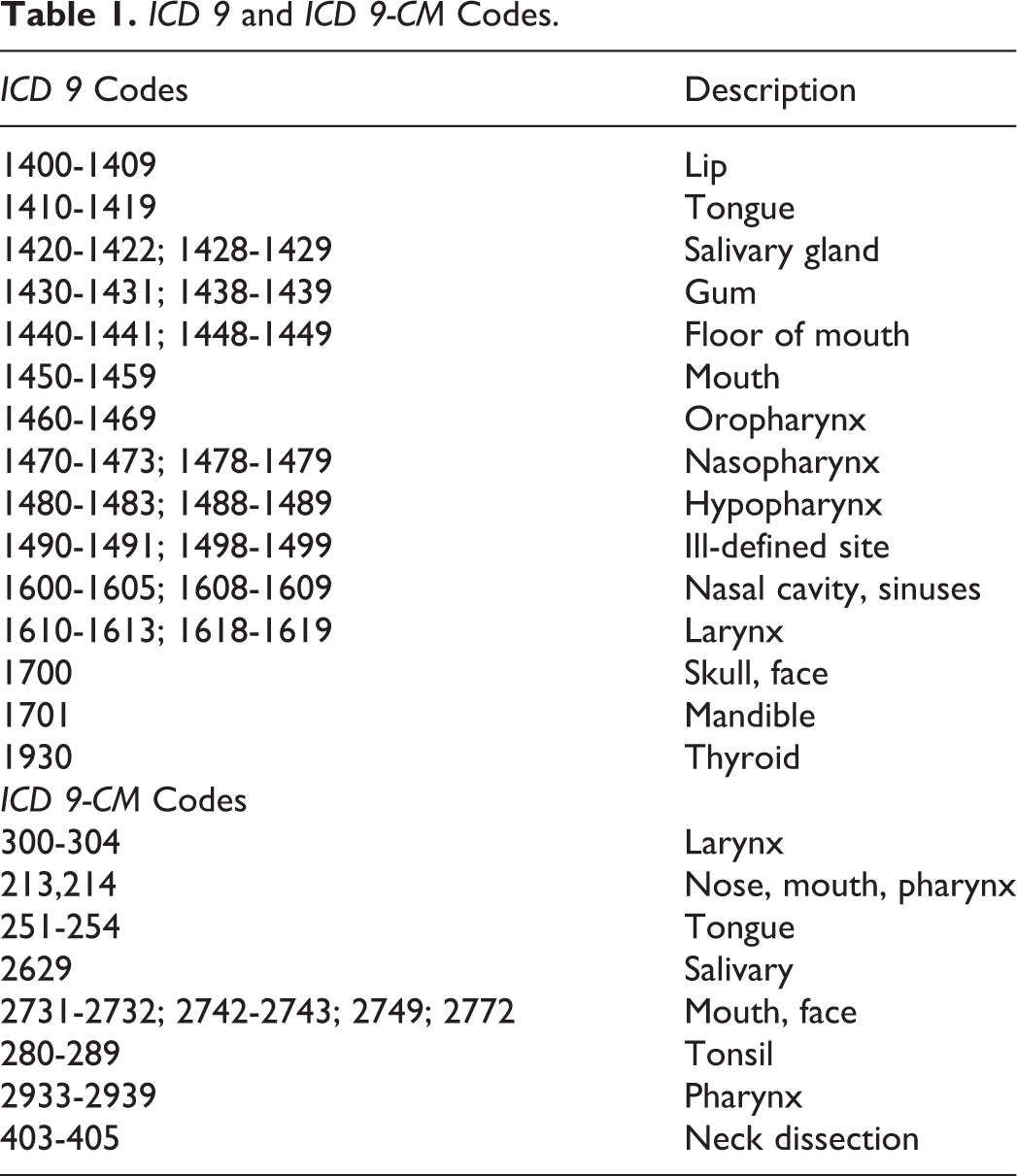
We analyzed the CDB/RM for discharge data on patients aged 18 to 100 years who underwent surgery for head and neck cancer at Vizient full-member academic medical centers between quarter 4 of 2009 and quarter 4 of 2012. All hospitalizations were identified on the basis of principal diagnosis, as specified by the International Classification of Disease, Ninth edition (ICD-9), and principal procedure codes, as specified by the International classification of diseases, Ninth edition, Clinical Modification (ICD-9-CM; see Table 1). All major cases of the head and neck were included and this yielded 22 357 patients. We then excluded thyroid cancer, skin cancer, and cases including patients less than 65 years of age. Thyroid cancer and skin cancers were excluded because, from our experience, these operations are very different in that the surgeries are shorter, have fewer complications, and require fewer days in the hospital. Extraction of cases with at least one of the diagnosis codes and at least one of the procedure codes resulted in 4544 cases of head and neck cancer during the 3-year time period evaluated.
ICD 9 and ICD 9-CM Codes.
Hospital volume was the primary independent variable in this study. Demographic information including a number of patients, sex, race, and number of comorbidities was also recorded. Cancer staging, cancer pathology, and histologic subtypes were not available from the Vizient database. Prior to analysis and after the dataset was obtained, hospitals were labeled into tertiles and described as high, moderate, and low volume hospitals. There currently exists no guideline as to what defines a high volume versus a low volume hospital for head and neck cancer. The analysis showed that high volume centers performed greater than 50 cases per year, moderate volume centers performed 22 to 49 cases per year, and low volume centers performed 21 cases or less per year during the time period evaluated.
Analysis
The primary clinical outcomes for this study were overall and specific surgical complications and comorbidities. Frequencies and proportions were calculated to describe the difference between 3 groups of hospitals for each of the outcome measures. The statistical software SAS version 9.3 (SAS Institute Inc., Cary, NC) was used. The χ2 test was performed to test differences in proportions between the 3 groups. A P-value less than .05 was considered significant.
Results
Patient Demographics
Ninety-three hospitals were involved in this study after the application of our criteria based on diagnosis and procedure codes. There were 12 high volume hospitals (n = 1544 cases), 20 moderate volume hospitals (n = 1543 cases), and 61 low volume hospitals (n = 1457 cases). The patient population was divided between the 3 hospital volume groups. Male patients comprised 63.7% of the study population; however, there was no significant difference in sex by hospital volume(P = .396). Furthermore, 84.4% of patients were defined as white compared to other races; with 75.22%, 84.39%, and 85.55% described as white in low, moderate, and high volume centers, respectively (P < .001). More specifically, high and moderate volume hospitals were more likely to treat white patients than low volume hospitals, with 35.0% receiving care at high volume centers, 35.5% receiving care at moderate volume centers, and 29.5% receiving care at low volume centers (P < .001). There was also a significant association between African-American and Hispanic patients and hospital volume, with 43.7% of African-American patients receiving care at low volume centers, compared to 29.2% receiving care at high volume centers (P < .001). Over half of Hispanic patients (56.9%) received care at low volume centers compared to 31.4% receiving care at high volume centers (P = .002).
Comorbidities
The percentage of patients with comorbidities managed by high volume hospitals (87.69%) was significantly less than those managed at moderate (90.53%) and low volume hospitals (90.19%; P = .020; see Table 2). The most common comorbidities seen across the 3 hospital volume groups were hypertension, metastatic cancer, chronic pulmonary disease, diabetes without complications, hypothyroidism, and fluid-electrolyte disorders. The only statistically significant comorbidities that differed across hospital case volume were metastatic cancer (P = .001), chronic pulmonary disease (P < 001), and fluid-electrolyte disorder (P = .0020). Comorbidities of metastatic cancer and chronic pulmonary disease were managed significantly more in moderate volume hospitals than high or low volume hospitals (metastatic cancer P = .002, P = .001; chronic pulmonary disease P < .001, P = .041; pairwise P-values are not present in tables). Other comorbidities that were significantly associated with volume-included deficiency anemia (P = .003), alcohol abuse (P < .001), weight loss (P < .001), obesity (P = .024), and chronic blood loss anemia (P < 0001).
Comorbidity Comparison.
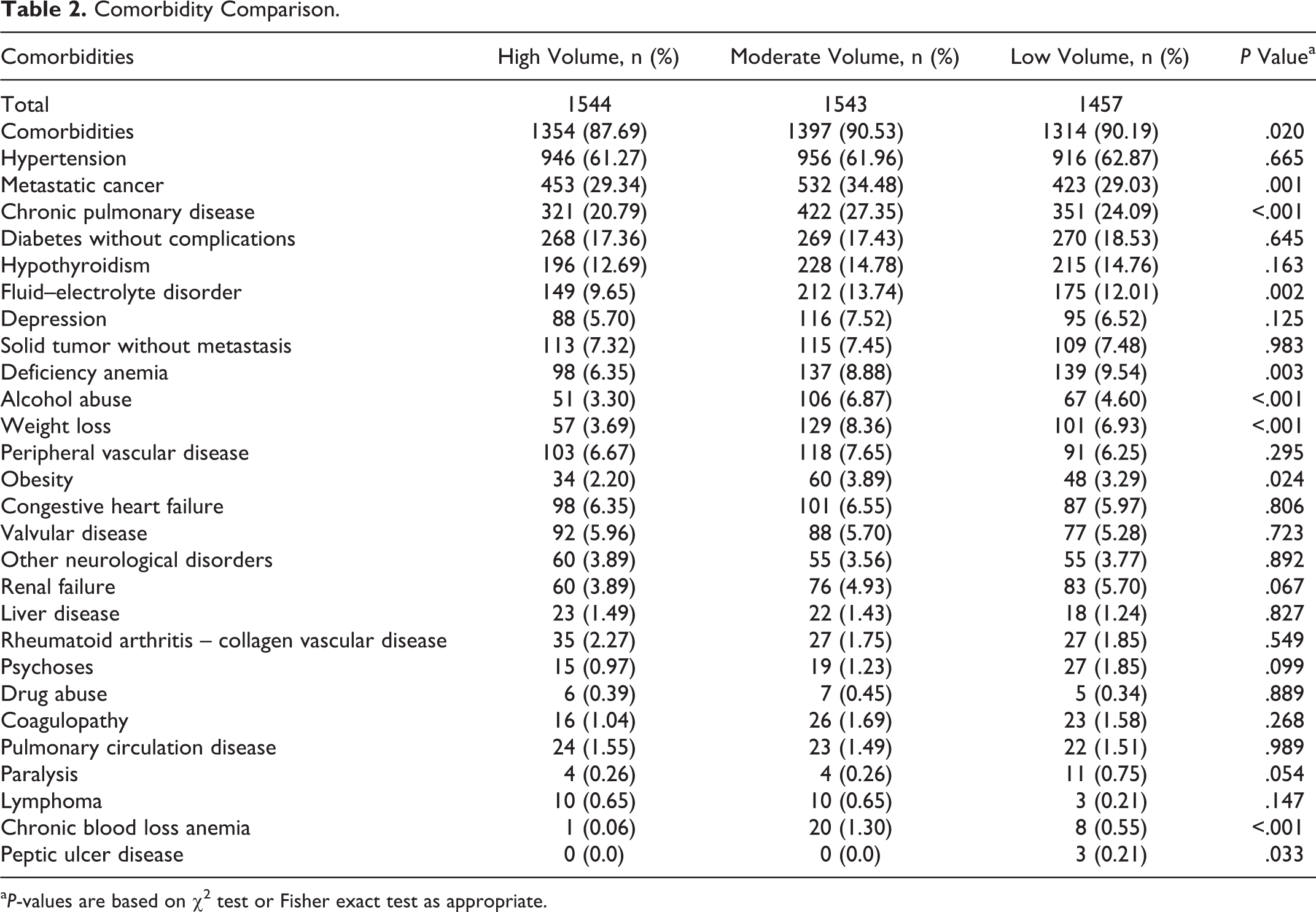
a P-values are based on χ2 test or Fisher exact test as appropriate.
Complications
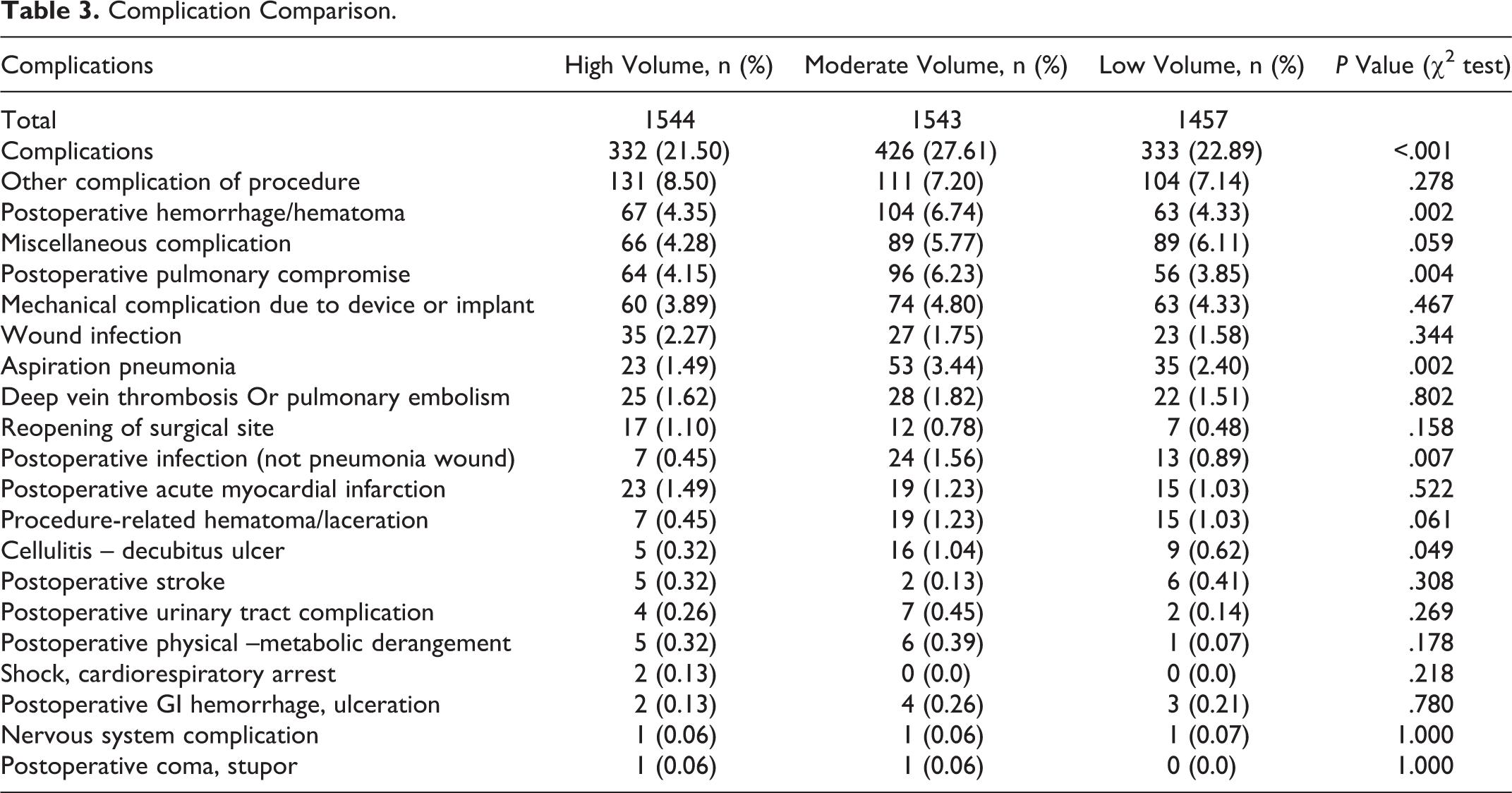
The overall complication rate was lowest in high volume hospitals (21.54%) and was significantly different than moderate (27.63%) and low volume hospitals (22.87%; P < .001; see Table 3). Miscellaneous complications included air embolism, blood incompatibility reactions, a foreign body accidentally left in a patient during a procedure, reaction to the foreign body left during a procedure, disruption of the wound, and emphysema. There was no overall significant association between miscellaneous complications and hospital volume (P = .059); however, there was a significantly lower rate of miscellaneous complications in high volume centers (4.28%), compared to low volume centers (6.11%; P = .024). There was a significant association between postoperative pulmonary compromise and hospital case volume (P = .004), with an increased rate of pulmonary compromise in moderate volume hospitals (6.23%), compared to high (4.15%) and low volume hospitals (3.85%). Furthermore, there was a significant association between hospital case volume and aspiration pneumonia (P = .002) with a higher rate in moderate volume hospitals (3.44%), compared to high volume hospitals, (1.49%; P < .001; pairwise P-values are not present in Table 2). There was also a significant association between hospital case volume and postoperative infection (P = .007) and cellulitis – decubitis ulcer (P = .049). The complication rates were lowest in the high case volume hospitals for both postoperative infection (0.45%) and cellulitis – decubitis ulcer (0.32%).
Complication Comparison.
Discussion
As a shift in demographics occurs over the next few decades with a higher percentage of people aged 65 years or older, it is necessary to focus on head and neck surgical outcomes within this population. According to the US Census, 1 in 5 people in the United States will be over the age of 65 by 2030. 23 Furthermore, it was projected that there will be an increase of 15.3% of head and neck surgical cases from 2006 to 2020, likely from the increased percentage of people in the geriatric population. 24 In an era of Accountable Care Organizations and pay for performance, it is necessary to be more cognizant of comorbidities specific to patients with head and neck cancer, in order to minimize intraoperative and postoperative complications. This information is even more crucial for geriatricians and primary care physicians because they often provide initial medical clearance for patients to receive head and neck surgery.
A subset analysis based on specific comorbidities indicated that the most common comorbidities in the geriatric population that are treated for head and neck cancer include hypertension, metastatic cancer, chronic pulmonary disease, diabetes without complications, and hypothyroidism. However, the only comorbidities that differed significantly across hospital volume were metastatic cancer and chronic pulmonary disease (P = .001 and P ≤ .001, respectively), which were both managed most often by moderate volume hospitals. In a prior analogous study examining a patient population of those aged 18 to 64 years, metastatic cancer was more likely to be managed by a high volume center. 11 A possible explanation for this disparity is that younger patients with head and neck cancer and metastatic disease are more likely to have the ability to travel to large academic medical centers to seek care, while geriatric patients have decreased ambulation and therefore seek care from the geographically closest qualified surgeon.
Although obesity was listed as a comorbidity associated with head and neck cancer, which was more likely to be managed in a moderate volume hospital (P = .024), there is some debate whether obesity increases the risk of surgical complications. 25,26 Yanquez et al. concluded that obesity alone does not increase the risk of surgical complications; however, more importantly, they did find that age combined with body mass index (BMI) was positively associated with increased morbidity and mortality in the higher age groups. 27 Some of the discrepancies regarding BMI and surgical outcomes can be attributed to the primary surgical site; nevertheless, we do not provide specific data to determine whether increased BMI is associated with increased surgical complications in patients receiving head and neck cancer surgery.
In addition to evaluating a patient’s comorbidities before recommending the head and neck cancer surgery, it is necessary to be able to inform patients of the most likely complications that may result from the procedure. The most common complications associated with head and neck cancer surgical procedures and that which demonstrated a significant difference based on case volume included postoperative hemorrhage/hematoma (P = .002), postoperative pulmonary compromise (P = .004), and aspiration pneumonia (P = .002). Although there were other complications that were also common, such as miscellaneous complications, mechanical complications due to device or implant, and wound infection (P = .059, P = .467, and P = .344, respectively), there was no statistically significant difference found based on hospital case volume. A possible reason why a higher complication rate of postoperative hemorrhage (6.74%), postoperative pulmonary compromise (6.23%), and aspiration pneumonia (3.44%), are more likely to occur in moderate case volume hospitals compared to low case volume hospitals is that complex head and neck surgical cases are more likely to be performed in moderate volume centers while low volume centers are less likely to perform acute surgical cases. Furthermore, high volume hospitals are less likely than moderate volume hospitals to have a high complication rate because they generally have more systems in place, such as more structured postoperative care, in order to minimize complication rates.
Although this study mainly focuses on surgical outcomes in geriatric patients, it is also important to note the effects of adjuvant therapy on this population. Landmark studies by Bernier et al and Cooper et al using a randomized control study design demonstrated that the use of adjuvant therapy including chemoradiation confers a survival benefit in patients with head and neck cancer with high-risk features (extracapsular extension and/ or positive surgical margins; 28,29 However, a recent study focusing on geriatric patients (age ≥70 years) with head and neck cancer with high-risk features showed that the addition of chemotherapy to postoperative radiation therapy did not confer a survival advantage. It is possible that the benefit of trimodality therapy including surgery, radiation, and chemotherapy may not apply to geriatric patients. 30
There may be some concern that free flap reconstruction is not appropriate for the geriatric population because of the increased operative time and multiple surgical sites; however, this is not the case. Although the results presented in this study are not specific to free flap reconstruction after tumor resection, there are multiple studies, which demonstrated no difference in surgical complications between elderly patients and younger patients, although geriatric patients are more likely to experience medical complications. 31,32
When performing head and neck cancer surgery on geriatric patients, it would be optimal to create a “surgical home;” 33 a multidisciplinary team that is designed to optimize outcomes for geriatric patients. For example, this team would include a head and neck cancer surgeon, geriatrician or primary care physician, social worker, dietician, therapists, and nurses. With a shift in medicine toward group decision-making, it is necessary to move away from the process in which a surgeon and patient solely make a decision regarding management of care. This process is necessary because geriatric patients receiving head and neck cancer surgery are often frail (inability to withstand physiologic insult) and ill 34 and are therefore at higher risk of complications from surgery. Furthermore, geriatricians and nurses trained to work with geriatric patients may be more aware of patient issues such as polypharmacy, postoperative delirium, baseline functional impairment, and other comorbidities that may result in complications during the postoperative period. 19 Additionally, having geriatricians and geriatric nurses use an assessment tool such as the comprehensive geriatric assessment or a shorter assessment tool such as the Geriatric 8, before and during treatment, will allow for better understanding of the patients’ functional age and prediction of how patients will respond to treatment. 35 -37 Ultimately, it is critical to remember that age in itself is not a reason to change the manner in which oncologic care is provided, although there are studies in the literature demonstrating that change in care does occur based on age, 38,39 but rather a functional status and comorbidities should be used to develop treatment plans. 40
There are several limitations to this study. First, this was an ecologic study since individual patient data are unavailable and therefore the study is susceptible to the “ecologic fallacy” in which we assume that individual members of the group have the characteristics of the group at large. For example, one individual low case volume hospital may have a lower complication rate than a high case volume hospital, even though high volume hospitals as a whole had a lower complication rate. Second, we are unable to differentiate between surgeon volume and outcomes, and therefore it is possible to say that high case volume hospitals may employ more head and neck surgeons and there is no proven association between surgeon volume and outcomes. Third, association does not mean causation, and therefore we cannot state that treating patients at high case volume hospitals will cause lower complications. It is possible that high volume hospitals have an additional factor unaccounted for that is causing the lower complication rate. Although there was a lower complication rate in high volume hospitals, the rate of comorbidities such as alcohol abuse and metastatic cancer were higher in moderate volume hospitals compared to high volume hospitals, and therefore it is possible that high volume hospitals may have a lower complication rate because they are treating “healthier” patients rather than as a result of case volume. Fourth, we listed the frequency of complications by hospital volume but did not determine if there were any noticeable trends over time. Fifth, we listed the most common comorbidities and complications; however, we were unable to describe which comorbidities cause patients to be more susceptible to specific complications.
Despite these limitations, we have demonstrated that managing head and neck cancer cases in the geriatric population is unique in comparison to the younger population. Geriatric patients are more at risk for different types of complications and present with more comorbidities. Therefore, it is necessary to manage cases using a multidisciplinary team and optimize communication between health-care providers. Although the option of hospice care and non-surgical management has not been emphasized in this article, it is necessary for geriatricians and head and neck cancer surgeons to be aware of this option to be able to best advise each patient.
This study used an externally managed national database to examine discharge data from 2009 to 2012, for patients who underwent surgery for head and neck cancer at 93 academic hospitals throughout the country. We found that high volume hospitals had a lower complication rate than low volume hospitals, although it is unclear whether decreased complication rates resulted from higher case volume or as a result of decreased rate of comorbidities in the patients treated at high volume hospitals. Therefore, it is difficult to definitely state based on the results that high volume hospitals will result in better outcomes compared to moderate or low volume hospitals and caution needs to be used when determining that high volume hospitals have better outcomes. As the demographics shift toward an aging population, it is necessary to improve communication between head and neck surgeons, primary care providers and geriatricians, and all others involved in caring for geriatric patients in order to minimize complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.