
Abstract
We report an interesting case of maxillary sinus pneumocele that presented with aesthetic deformity and completely treated with Caldwell-Luc approach and thoroughly review all of the past literature focusing on clinical symptoms and surgical approach. Based on our comprehensive review of maxillary sinus pneumocele, we found 2 important characteristics. First, maxillary sinus pneumocele may be asymptomatic but cause various symptoms owing to the displacement of neighboring structures, such as facial symptoms, eye symptoms, and nasal obstruction. Second, there is no standard operation technique for maxillary sinus pneumocele, but surgical approach should be individualized depending on patient’s symptoms and needs. Therefore, more case studies are needed to confirm this.
Introduction
Pneumocele is a rare lesion of the paranasal sinus characterized by abnormal expansion of an air-containing sinus lined with normal mucosa. 1 It gradually displaces the surrounding structures as the bony sinus wall becomes thinner. This lesion can occur in any sinus, with the frontal sinus most commonly affected, whereas involvement of the maxillary sinus is an exceedingly rare condition. 1,2 Maxillary sinus pneumocele was first described by Noyek et al in 1974, followed by only 10 additional cases. 1,3 –12 Maxillary sinus pneumocele is usually asymptomatic over long periods but may cause significant clinical symptoms related to compression of adjacent structures such as facial pain and aesthetic deformities cause by the locally gradual expansion. 4 –6
In this article, we describe the case of maxillary sinus pneumocele presented with both right facial pain and aesthetic deformity with literature reviews focusing on clinical symptoms and surgical approach.
Case Report
A 23-year-old man presented with right facial pain that had not improved by medication for 2 years. The pain was aggravated after nose blowing or flight. He also complained of the change in right facial contours that did not become worse after 2 years ago. The patient denied any history of sinusitis, facial trauma, or prior nasal surgery. On physical examination, there was a hard, nontender, and 2 × 2 cm–sized bulging on the right maxillary area without overlying skin changes (Figure 1A and B). Nasal endoscopy showed no abnormal findings. Facial computed tomography (CT) images revealed the marked expansion of the right maxillary sinus with anteromedial displacement and thinning of the bony wall, but there was no defect (Figure 2A-C).

Preoperative external photographs show a 2 × 2–cm sized protrusion on right maxilla area (A and B). Clinical photographs 6 months after surgery show the improvement of facial contour compared to preoperative state (C and D).
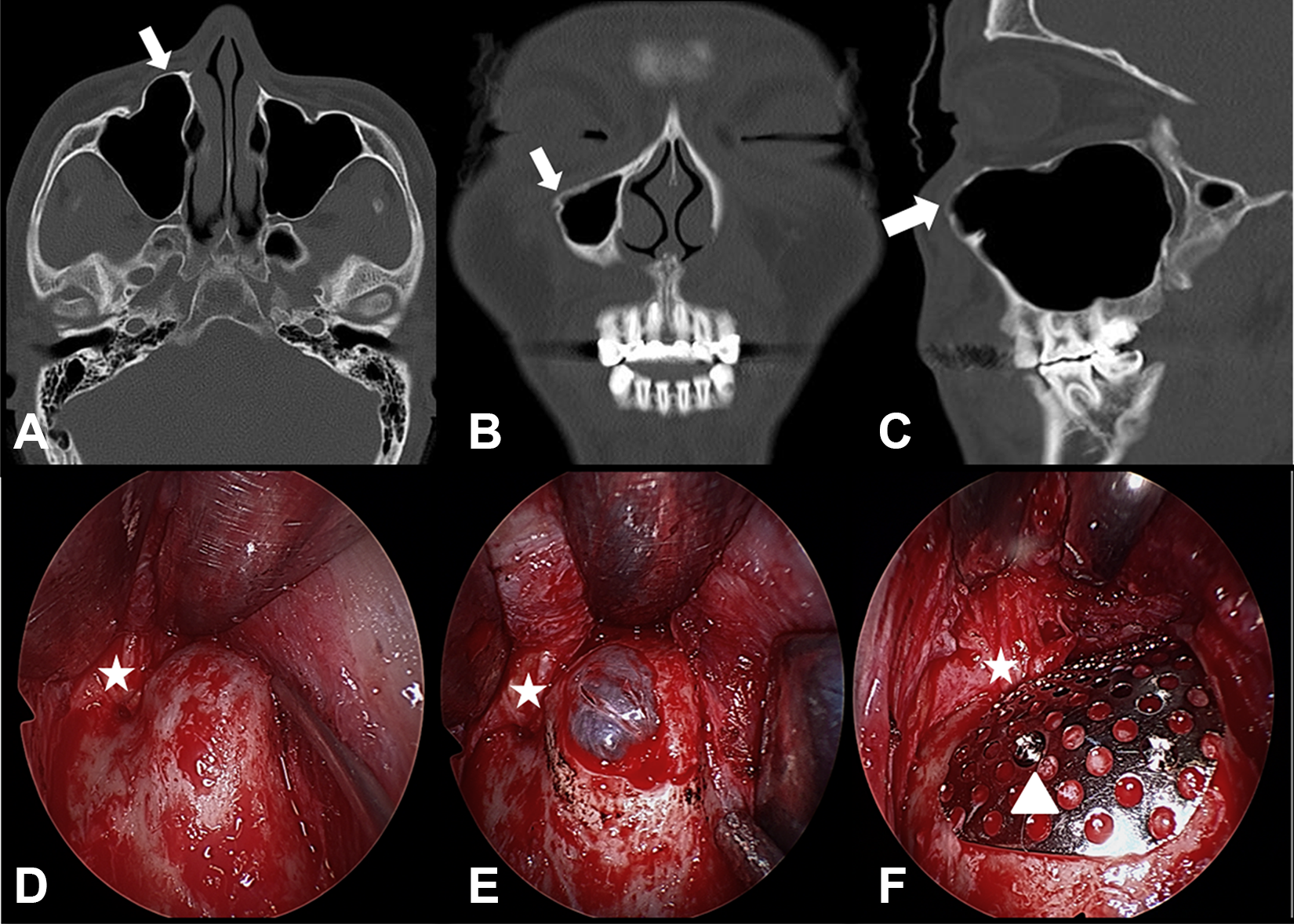
Facial CT scan shows enlarged right maxillary sinus (arrows) expanding anteromedially with thinned bony wall; axial view (A), coronal view (B) sagittal view (C). Operative findings show protruded anterior maxillary wall before the osteotomy by Caldwell-Luc approach (D). After the removal of bony wall (E), the defect was reconstructed with titanium mesh (F; asterisk: infraorbital bundle, arrow head: mini-screw). CT indicates computed tomography.
Based on abovementioned findings, we clinically diagnosed as maxillary sinus pneumocele and decided to perform pneumocelectomy for decompression using Caldwell-Luc approach under general anesthesia. The operative findings were that the bony wall of right maxillary sinus showed the anteromedial protrusion compared to the left side and the overlying mucosa appeared normal after removal of the protruded bony wall (Figure 2D and E). We used titanium mesh to reconstruct the anterior wall of right maxillary sinus (Figure 2F). The patient discharged without postoperative complications. After 2 weeks, facial pain subsided completely and the preoperative facial asymmetry was largely improved (Figure 1C and D). There is no evidence of recurrence during a follow-up 12 months.
Discussion
Diseases causing pathological expansion of the paranasal sinuses containing only air include hypersinus, pneumosinus dilatans, and pneumocele, but terms are often used interchangeably. Hypersinus refers to air-filled sinus so that the size of the sinus does not compress the surrounding structures without presenting symptoms. Pneumosinus dilatans denotes expanded sinus beyond the normal boundaries, but the sinus wall thickness is normal without any defect. 13 Pneumocele is similar to pneumosinus dilatans but characterized by the enlarged sinus in which the wall thickness is not uniform and partly thinned with loss of integrity. According to this definition, pneumocele is most suitable for our case in that the bony wall of maxillary sinus lined with normal mucosa is thinned, but not eroded.
Based on previously reported cases, pneumocele of the frontal and sphenoid sinus is frequently described, but only several cases have been reported in the maxillary sinus where the anteromedial portion is often involved. 10 It is thought that the anteromedial wall in the maxillary sinus is the thinnest and most affected when changes in barometric pressure occur. Pneumatization is a physiologic process that occurs in all paranasal sinuses during the growth period. However, pneumatization of the paranasal sinuses shows broad individual differences in dimension not only in dependence on the patient’s age. The pathogenesis of pneumocele remains unclear, but the presence of a 1-way valve is known as the most convincing mechanism. 1,12 Nasal polyps, redundant mucosa, inflammation and anatomic variation which caused obstruction of the natural orifice act as a 1-way valve. This allows air to enter the sinus with cough or nose blowing (chronic air trapping) but prevents subsequent pressure equalization and produces air trapping (intrasinus pressure disequilibrium). The increased intrasinus pressure leads to chronic expansion of the sinus wall (hyperpneumatization). 12 In our patient, there was no evidence of obstructive lesion around the maxillary sinus ostium at first visit, but considering that the patient complained of changing facial contour 2 years ago, pneumocele might be occur when the 1-way valve of the maxillary sinus ostium was present.
We reviewed 11 maxillary sinus pneumocele cases that selected patients of 11 retrieved articles from PubMed (Table 1). 1,3 –12 The mean age was 29.1 years, ranging from 9 years to 62 years with a female to male ratio of 6:5. All 11 patients had unilateral lesion with right side preponderance; the involved side was on the right side in 9 patients and on the left side in 2 patients.
Reported 11 Cases of Pneumocele of the Maxillary Sinus.
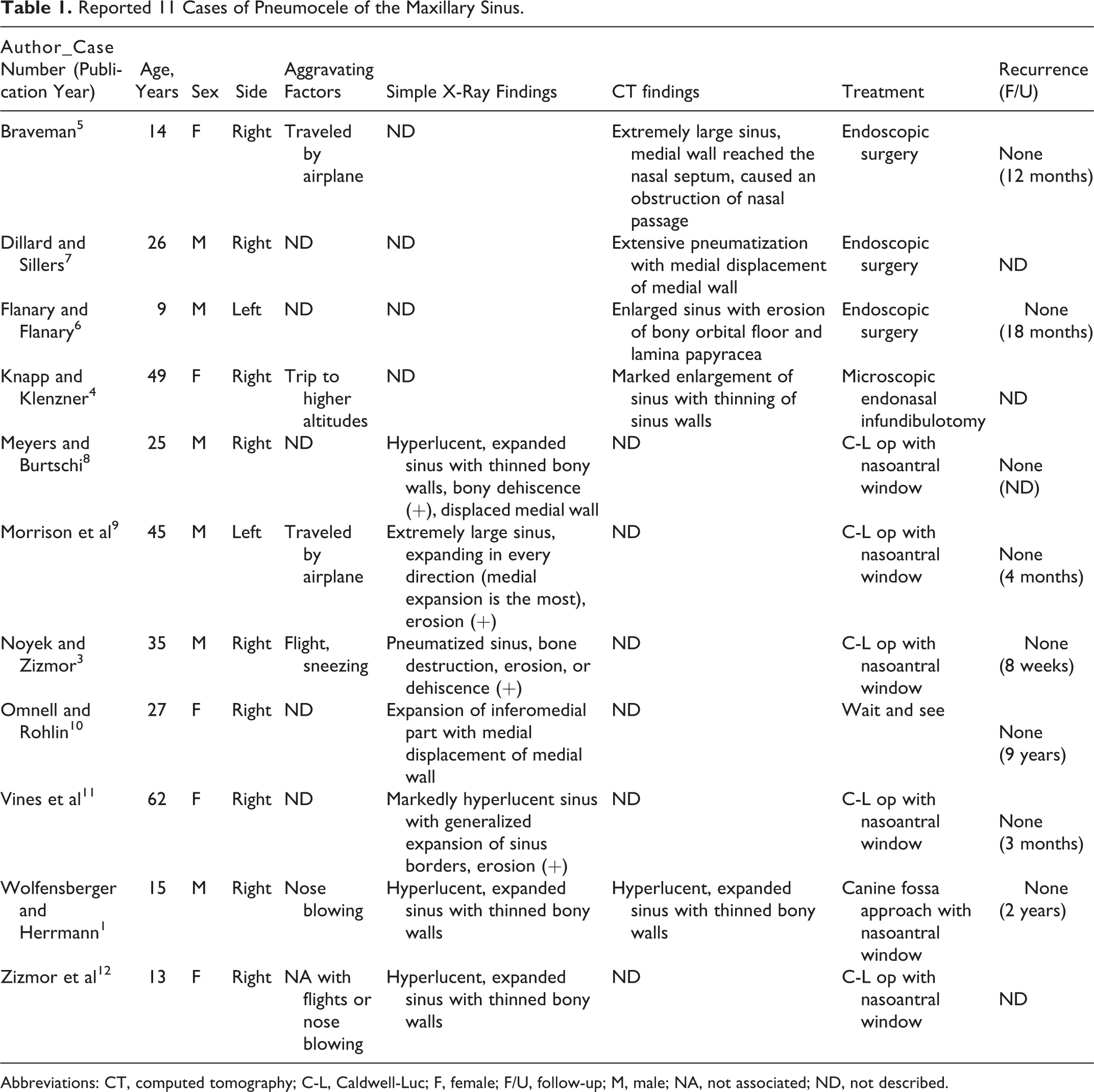
Abbreviations: CT, computed tomography; C-L, Caldwell-Luc; F, female; F/U, follow-up; M, male; NA, not associated; ND, not described.
Maxillary sinus pneumocele may be asymptomatic but cause a variety of symptoms described in Table 2. It may usually be presented as facial symptoms including slowly changing facial contours over long periods and dull maxillary cheek pain or pressure on the affected area. 4 Other associated symptoms are included in eye symptoms such as exophthalmos and increased scleral show and nasal symptoms, especially unilateral nasal obstruction owing to the displacement of neighboring structures. 5,6
Descriptive of Patients With Maxillary Sinus Pneumocele of Current Literature Review.
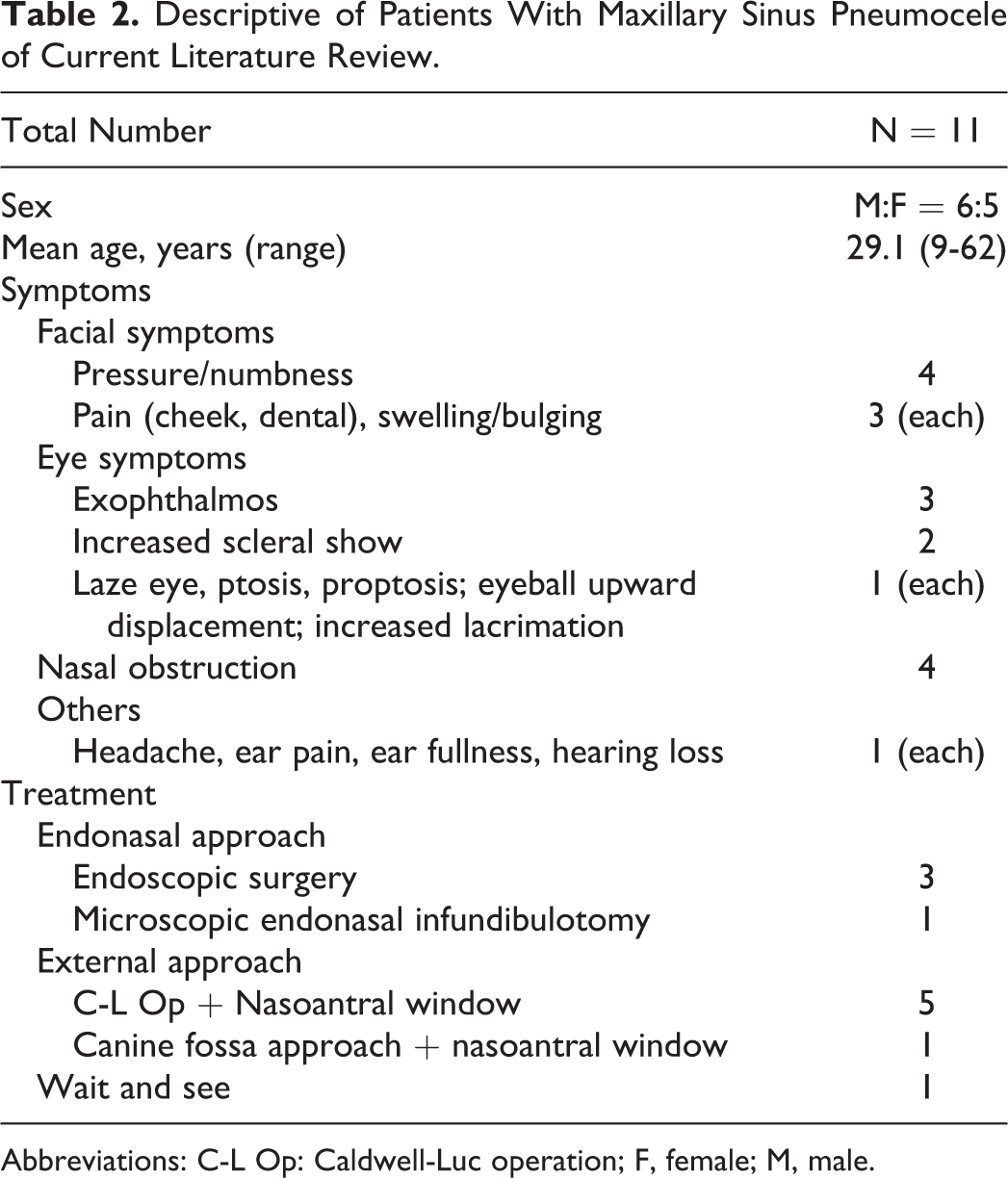
Abbreviations: C-L Op: Caldwell-Luc operation; F, female; M, male.
Maxillary cheek pain or pressure may be caused by irritation of the maxillary division of trigeminal nerve (trigeminal irritation) due to the mass effect or direct pressure on the nerve. The pain is exacerbated with sudden changes in atmospheric pressure, such as in trips to the mountains, flying, diving, or when blowing the nose by the mechanism described earlier. 1,4 Although the only early symptom of maxillary sinus pneumocele is pain accentuated by nose blowing, whether increased antral pressure after nose blowing is indeed responsible for the expansion of the maxillary sinus may still be open to debate. 1 The diagnosis should be clear with CT scans after the associated symptoms have presented. 6 Computed tomography scans show a hyperpneumatization of the sinus with bony thinning. Nasal endoscopy shows normal mucosa without secretions. Pneumocele requires differential diagnosis with mucocele and benign or malignant neoplasms. 4 In addition, trigeminal neuralgia should be taken into account. 4
Surgery is curative. 12 However, surgery is not necessary if the lesion does not cause discomfort or continue to expand on regular follow-up. 10 Based on our review, all except one patient were treated surgically. The surgical approach used in 10 patients is described in Table 2. Endonasal approach was used in 4 patients, 3 patients received endoscopic sinus surgery, and 1 patient received microscopic endonasal surgery. Six patients were treated with external approach, of which 5 patients received Caldwell-Luc approach, and 1 patient was treated by canine fossa approach. Since the report of Noyek et al 3 in 1974, Caldwell-Luc approach had been used in the past. Recently, according to the development of various endoscopes and endoscopic sinus surgery since 1990s, the decompression through endoscopic endonasal approach with creation of an adequate nasoantral window is the method of choice that may enable good ventilation of the sinus and relief of the entrapped air. 4,5 However, clinical symptoms of the reports treated with endonasal approach were cheek pain or pressure and eye symptoms, not facial asymmetry. There is no standard operation technique for the correction of facial deformity due to the rarity of previously reported cases. In our case, he chiefly complained of the change in right facial contours (facial deformity) as well as dull facial pain. Thus, we decided to achieve both surgical purposes through Caldwell-Luc approach. The anterior protruded wall of maxillary sinus removed through Caldwell-Luc approach was so broad that we reconstructed the anterior wall with titanium mesh and mini screw. However, we did not make the nasoantral window, since the natural ostium of the maxillary sinus was normal on preoperative CT scans. The patient was satisfied with the facial contour as well as the loss of pain.
In conclusion, we report an interesting case of maxillary sinus pneumocele that presented with aesthetic deformity and completely treated with Caldwell-Luc approach. Also, based on our comprehensive review of maxillary sinus pneumocele, we found 2 important characteristics. First, maxillary sinus pneumocele may be asymptomatic but cause various symptoms owing to the displacement of neighboring structures, such as facial symptoms, eye symptoms, and nasal obstruction. Second, there is no standard operation technique for maxillary sinus pneumocele, but surgical approach should be individualized depending on patient’s symptoms and needs. Therefore, more case studies are needed to confirm this.
Footnotes
Authors’ Note
Written consent was obtained for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.