
Abstract

A 50-year-old man presented to the clinic with a persistent draining wound over the left submandibular region. The left submandibular swelling developed 1 year prior. He later developed a sialocutaneous fistula over the area. He complained that saliva-like fluids drained from the wound in the skin when he had a meal. On clinical examination, a 0.5 cm erythematous opening was noted over a large indurated mass in the left submandibular region. The area was tender and purulent discharge could be expressed by palpation. Peroral examination revealed a 5-cm tender, firm mass in the left floor of the mouth near the submandibular gland. The ductal opening was normal.
A neck computed tomography showed a 5.2 cm × 4.2 cm stone within the medial aspect of the left submandibular gland, with periglandular infiltration and several ducts’ dilatation and wall enhancement (Figure 1). A calcified mass in the left submandibular gland hilum extended to the left parapharyngeal space with displacement of the left oropharyngeal wall. A fistula tract between the left submandibular gland and left paramedian skin was noted (Figure 2). On the serologic result, his calcium, ionized calcium, and parathyroid hormone level were within normal range.
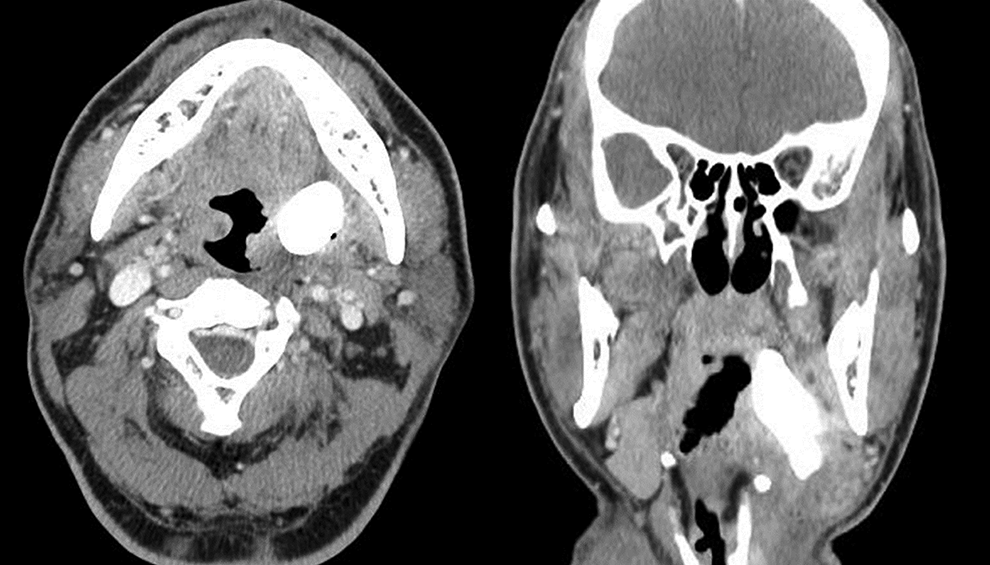
Computed tomography scan of the neck without contrast demonstrating a large sialolith of the submandibular gland on the left side. The stone lies on the medial aspect of the gland, compressing the left parapharyngeal space with displacement of left oropharyngeal wall.

Preoperative front view showing swelling in the left submandibular region with sialocutaneous fistula.
The submandibular gland with the calculus and sialocutaneous fistula were excised via an incision in the skin crease 2 cm below the lower border of the mandible and directly over the palpable submandibular gland. The skin was ellipsed around the area of the draining sinus and granulation tissue. The gland with the calculus was dissected free and the wound closed layer by layer. Pathology revealed a submandibular gland measuring 4.5 cm in its largest dimension, with the stone measuring 5.6 × 3.5 × 2.9 cm. The calculus was oval shaped, tan in color, and had a granular surface (Figure 3). The calculus was surrounded by granulomatous fibrous tissue. Adjacent to the calculus, there was inflamed yellowish salivary gland tissue.

Macroscopic view of the surgically obtained stone measured 52 × 42 mm.
Sialolithiasis is one of the most common diseases of the salivary glands in the adults. 1 It is a condition characterized by an obstructive process in a salivary gland or duct due to calculi. The patients suffer from local swelling and pain, including infection of the gland tissue and dilation of the duct. It is estimated that 80% to 90% of cases occur in the submandibular gland, while 10% to 20% occur in the parotid gland. 2 Most salivary stones range between 3 and 7 mm in size and are amenable to endoscopic removal. 3 Stones occasionally grow to large size (≥8 mm) and rarely grow to over 15 mm, at which point they are classified as megaliths.
Calculi greater than 15 mm in size are defined as giant sialoliths. Giant sialoliths measuring greater than 50 mm are rare, with only 6 cases published in the literature. 4 The largest sialolith reported was 72 mm in length in the Wharton’s duct. 4 However, it was fragmented during removal. Our case is the largest salivary stone with sialocutaneous fistula. The ability of a small stone to grow and become a giant sialolith depends on the affected duct’s reaction. When the sialolith is located in the distal part of duct, it can be dilated and allow a normal secretion of salivary flow around the stone, so the sialolith might increase in size while accommodating to the shape of duct, becoming a giant calculus, and remain asymptomatic for a long period. 5 Occasionally, stones located more proximally behind the posterior border of mylohyoid muscle (with recurrent episodes of obstruction) may increase in size, sometimes requiring an extraoral approach. Sialoliths might be associated with true salivary gland cysts. Such lesions occur due to the obstruction of the salivary flow, followed by a proliferation of the duct epithelium that surrounds the stone. The current specimen presented a squamous differentiation in accord with the literature. 2
The deposition of salivary calculi is not associated with systemic diseases involving calcium metabolism such as hypercalcemia and hyperparathyroidism. Gout can be associated, although gout calculi consist of urate. Salivary calculi consist of calcium phosphate with small accounts of hydroxyapatite, magnesium, potassium, and ammonia. 5 Sialocutaneous fistula is a very rare complication. Sialocutaneous fistula can be associated with tumorous conditions, 6 but to our knowledge, there was no case involved with giant sialolith excepting one megalith case with sialocutaneous and sialo-oral fistula. 7 It is possible that an impacted stone obstructing the submandibular duct resulted in stasis, infection, and subsequent skin rupture. In cases with megalith in the proximal duct of submandibular gland, the clinician should consider the possibility of complications such as sialocutaneous fistula.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Inha University Research Grant.