
Abstract

A 40-year-old female was seen initially at an outside hospital in November 2012 and presented with severe dysphonia and near-complete aphonia. The patient had a history of rheumatoid arthritis (RA) and was previously on etanercept and methotrexate (MTX). She had wished to get pregnant, and her rheumatologist had discontinued these medications and placed her on high-dose prednisone 6 months prior to her presentation. Over the course of the following 6 months, she had gradual voice loss. An outside otolaryngologist performed a flexible laryngoscopy and noted a posterior glottic mass and subsequently referred her for a voice evaluation and videostroboscopy. The videostroboscopy demonstrated a left submucosal mass just anterior to the vocal process (Figure 1) causing incomplete glottic closure and stiffness of the left vocal fold with decreased amplitude and mucosal wave. The patient also had signs of laryngopharyngeal reflux including mucosal erythema, postcricoid edema, and interarytenoid pachydermia. The patient was started on a double-dose proton pump inhibitor and scheduled for excision in 1 month.

Intraoperative image of the vocal folds demonstrating the rheumatoid nodule on the left vocal fold.
The patient underwent suspension microlaryngoscopy with excision of the left vocal fold lesion by micro-flap technique and a vocal fold steroid injection. Pathology revealed fibrinoid necrosis surrounded by palisading histiocytes consistent with a rheumatoid nodule (Figure 2). The patient did well afterward with return to her baseline voice, and repeat stroboscopy at 3 months after the procedure revealed no submucosal masses. The patient was seen at regular 3- to 4-month intervals with an excellent voice and no return of a submucosal mass.

Pathology slide from the patient’s excised submucosal lesion, hematoxylin and eosin (H&E) stain. There are fragments of fibroconnective tissue with multiple foci of fibrinoid necrosis surrounded by histiocytes, focally palisading, and multinucleated giant cells. Lymphocytes and plasma cells are seen infiltrating the connective tissue.
At 18 months after her surgery, a left-sided submucosal mass was seen posterior to the original rheumatoid nodule adjacent to the vocal process (Figure 3). The patient was also developing rheumatoid nodules in her upper extremities. The patient had not gotten pregnant throughout this 18-month period, and she and her rheumatologist decided to place her back on her etanercept and MTX and discontinued the prednisone. In the following several weeks, the submucosal mass slowly receded, and she did not require additional surgery.
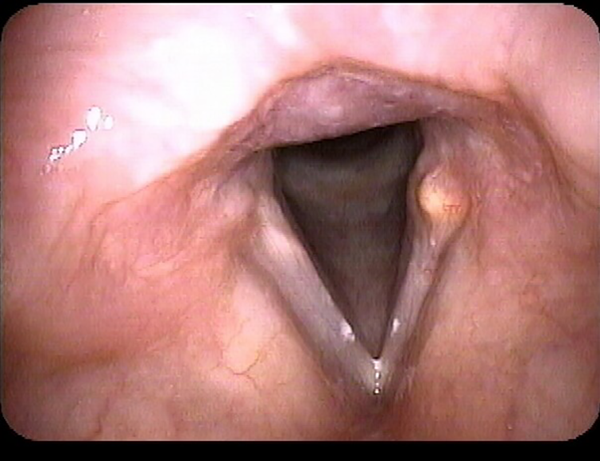
Laryngoscopic photograph demonstrating the recurrence of the vocal fold submucosal mass 18 months after excision.
The most common area of the head and neck affected by RA is the larynx, with postmortem studies suggesting it may affect close to 80% of patients with RA. 1 –3 This case is unique because of the setting in which the patient developed her laryngeal nodule, the location of the nodule, and the recurrence of the nodule following surgical excision. Although much attention has been given to cricoarytenoid (CA) joint arthritis in the setting of RA, discussion of rheumatoid nodules in this disease has not received as much attention, despite it being a debilitating manifestation of RA. In the case of our patient, she had near-aphonia that developed over 6 months, which can be quite incapacitating especially for patients whose job depends on using their voice. Several studies have stated that patients with increased use of their voice are more prone to developing such lesions. 4 Another more serious and life-threatening complication is airway obstruction secondary to poor CA joint mobility. In some cases, patients require permanent tracheotomy due to paralysis of the vocal folds. 5
Previous studies have stated that systemic steroids help decrease the size of rheumatoid nodules. 4,6 Yet, this patient started developing systemic nodulosis when starting high-dose prednisone. Additionally, the patient developed nodulosis after discontinuing MTX therapy. Methotrexate, which is used widely in the treatment of RA, has been associated with the increased development of rheumatoid nodules, 7 and reports have been made of patients developing laryngeal rheumatoid nodules while on MTX therapy. 8 When the patient eventually restarted her MTX and etanercept, however, her rheumatoid nodule decreased in size and clinical symptoms improved.
The location of the patient’s rheumatoid nodule in the larynx is also unique. Many of the nodules reported in the literature occur at the middle third of the vocal fold mucosa, and they are often bilateral. 4,9,10 Bilateral nodules occurring in this region have been named “bamboo nodes” and occur with many kinds of autoimmune disease, including Sjögren disease, systemic lupus erythematosus, systemic sclerosis, and Hashimoto’s thyroiditis. 4,10 It has been proposed that rheumatoid nodules tend to occur in regions that are subject to repeat “microtrauma.” 11 The area at the center of the vocal folds is subject to the greatest shearing forces during vibration. 10 This may also explain why such lesions occur most often bilaterally. 10 Yet, in our patient, the nodule occurred in the posterior third of the musculomembranous vocal fold and was unilateral. This may suggest a different mechanism for the development of rheumatoid vocal fold nodules that has not yet been explored.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.