
Abstract

A 37-year-old otherwise healthy male presented with a 3-month history of a gradually growing, painless, right cheek mass. There was no history of trauma or systemic complaints. He was diagnosed elsewhere with pleomorphic adenoma (PA) based on imaging and fine-needle aspiration (FNA).
On initial encounter, the patient was found to have a mass at the posterior border of the masseter muscle, which was firmly adherent to the mandible. Examination was otherwise unremarkable.
Review of imaging revealed a 2.5 cm × 2.5 cm × 1.8 cm heterogeneously enhancing mass with cystic change centered on the right masseter muscle. Periosteal reaction was present without cortical erosion (Figure 1A and B).
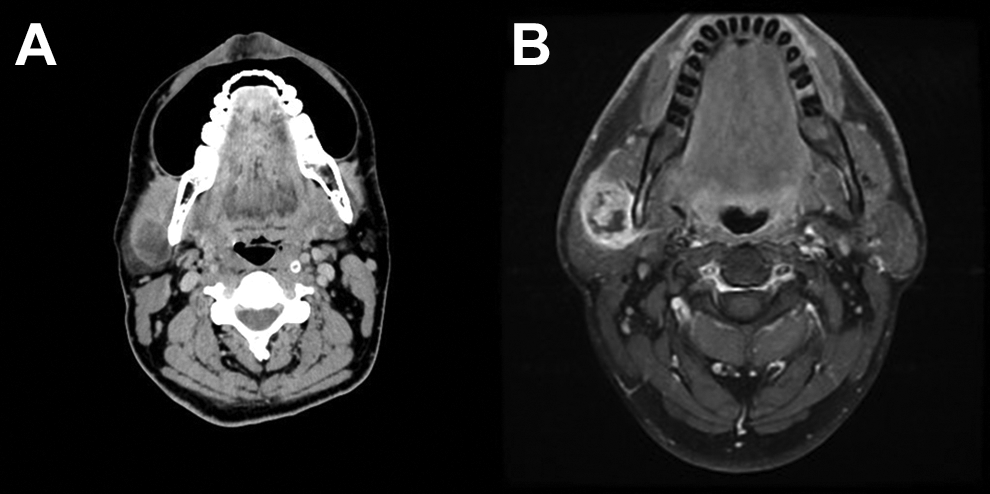
A, Contrast-enhanced axial CT demonstrates right masseter origin mass. B, Axial contrast-enhanced T1 MRI shows mass within the right masseter with periosteal reaction and mandibular enhancement. CT indicates computed tomography; MRI, magnetic resonance imaging.
Due to concern for malignancy, the patient underwent repeat FNA, with insertion of the needle posterior into the parotid gland to avoid artifact in the specimen. This sample was consistent with nodular fasciitis (NF). The patient elected to undergo surgical excision rather than observation. During excision, the parotid gland was elevated, the facial nerve was identified, and the inferior division was gently retracted to facilitate dissection down to the mandible, where the lesion was identified. The mass was intimately associated with the surrounding periosteum (Figure 2A). Scalloping was noted in the cortex of the underlying mandible without evidence of bony infiltration (Figure 2B). Excision was completed with negative surgical margins (Figure 2C), and the patient experienced an uneventful postoperative course.

Intraoperative images. A, The well-circumscribed lesion is seen deep to the parotid gland overlying the ramus of the mandible. B, Scalloping of the cortical bone is seen at the site of the mass. C, Complete excision of the mass is shown with negative gross margins.
Nodular fasciitis is a self-limiting, pseudosarcomatous lesion composed of fibroblasts and myofibroblasts. 1 Although arising most often within the extremities, NF can often arise within the head and neck. Nodular fasciitis arises within fascia or subcutaneous tissue but can also occur within muscle or organ parenchyma, such as the parotid gland.
The etiology of NF is poorly understood. Historically, it was thought to arise in the setting of trauma, but most cases have no significant traumatic history to support this. Recently, NF has been found to be associated with a somatic MYHP-USP6 gene fusion, suggesting that this is a transient neoplasm. 2
Nodular fasciitis typically presents as a rapidly growing, painless mass in patients between the ages of 20 and 40 years. 3 Although NF is a benign process, the rapid growth raises suspicion of malignancy when arising in the head and neck. In addition, nonspecific imaging and pathology findings often fail to quell these concerns. Fine-needle aspiration often shows increased cellularity and mitotic activity, similar to that of a malignancy. 4 Imaging can show lesions arising adjacent to parotid fascia with irregular and infiltrative borders.
The differential diagnosis for rapidly growing masses of the head and neck is broad and includes benign and malignant neoplasms. The cytology of NF shares many similarities with other tumors of the head and neck. 5,6 Furthermore, lesions of the masseter and surrounding fascia can be confused clinically with salivary neoplasm, given its close proximity to the parotid gland.
Nodular fasciitis misdiagnosed as PA based on histology has previously been reported. 7 Fine-needle aspiration demonstrating spindle or plasmacytoid cells within a myxoid background may appear consistent with PA. Also, en route to reaching lesions adjacent to the parotid gland, FNA may pick up cells from the overlying parotid gland, leading to a polymorphous tissue sampling. This phenomenon was seen in this case. Differentiating between NF and PA may be challenging, but the presence of chondromyxoid matrix and ductal structures suggests PA, whereas the presence of inflammatory cells and mitoses suggests NF.
Schwannomas are uncommon near the parotid gland but should be considered in atypical lesions such as this. These benign tumors are usually slow growing and tender, often associated with radiating pain. 1 Compared to NF, schwannomas are well circumscribed and encapsulated. Pathology shows directionality with palisades and Antoni A/B areas. Immunohistochemistry demonstrating S100 positivity can confirm epidermal origin, consistent with schwannoma. 1
One must consider the possibility of malignancy when evaluating a growing neck mass. Imaging of NF can demonstrate irregular and infiltrative borders, similar to sarcoma. Furthermore, FNA can show concerning features including frequent mitoses, spindle cells, and low-grade atypia. 1 It is important to distinguish NF from malignancy to avoid overly aggressive treatment. Fibrosarcoma can be differentiated from NF based on greater hypercellularity and mitoses with less myxoid background. 8
The differential diagnosis for NF is broad and includes both reactive and neoplastic processes. Once diagnosis is made, NF is commonly treated with limited surgical excision. Observation is also reasonable as these lesions tend to involute over time. Malignancy must be ruled out before deciding on conservative management, however. Recurrence of NF is uncommon and sequelae of these lesions are seldom seen.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.