
Abstract
Introduction:
Conventional surgical approaches to the lateral aspect of a well-pneumatized sphenoid sinus are associated with significant surgical morbidity. Transorbital endoscopic approaches have recently gained favor as an alternative approach to the skull base. We describe the use of a contralateral precaruncular endoscopic approach to provide a surgical pathway to the lateral aspect of the sphenoid sinus, allowing for improved and direct visualization of the surgical field, with limited morbidity.
Case Report:
A 60-year-old female patient, with a spontaneous cerebrospinal fluid leak from a Sternberg canal defect in the sphenoid sinus, underwent repair of the defect at Groote Schuur Hospital (Cape Town, South Africa). A contralateral precaruncular approach, using the left medial orbital portal, was utilized to access the defect in the lateral aspect of a well-pneumatized right sphenoid sinus. Computer modeling software was used to predetermine the surgical pathway, and the case was performed under navigation guidance. Adequate surgical access was obtained to the lateral sphenoid sinus and sinus defect, with superior visualization compared to a pure transnasal or transpterygoid approach to the lateral sphenoid sinus.
Conclusions:
This case validates the use of computer simulation to plan and decide on the best operative approaches in skull base surgery and describes the contralateral precaruncular approach as a surgical pathway to the lateral sphenoid sinus. Advantages of the contralateral precaruncular approach include a direct trajectory toward the sinus defect, easy access with a standard 18-cm, 4-mm, 0-degree rigid endoscope, and straight instruments, with sparing of the pterygoid base and contents of the pterygopalatine fossa.
Keywords
Introduction
Spontaneous meningoencephaloceles of the sphenoid sinus are an uncommon cause of cerebrospinal fluid (CSF) rhinorrhea. 1 -3 Surgical repair of the defect is indicated in cases of CSF leakage or a history of meningitis. The traditional surgical approach to these lesions involved a temporal craniotomy to achieve adequate exposure of the defect. Advances in endoscopy have subsequently led to the development of an endonasal transpterygoid approach to the lateral recess of the sphenoid sinus. Although the transpterygoid endoscopic approach is associated with a significantly reduced morbidity when compared to the open approach, the extent of dissection that may be required often results in complications such as hemipalatal hypoesthesia and lacrimal gland hyposecretion. 4 Transorbital endoscopic approaches have recently gained favor as an alternative approach to the skull base. 5 We describe the use of a contralateral precaruncular approach to provide a surgical pathway to the lateral aspect of the sphenoid sinus, allowing for better direct visualization and instrument manipulation, obviating the need for transpterygoid dissection.
Case Report
A 60-year-old female patient, with comorbid hypertension and diabetes mellitus, presented to our department with recurrent, spontaneous CSF rhinorrhea, confirmed with positive β-2 transferrin testing. She had undergone one previous surgical repair of the defect in 2000. No surgical notes were available regarding her previous intervention. A computed tomography scan and magnetic resonance imaging identified a skull base defect and possible meningoencephalocele in the lateral wall/recess of a well-pneumatized right sphenoid sinus—a common site for a spontaneous CSF leak (Figure 1). The defect was not accessible using a traditional endoscopic transsphenoidal approach due to the trajectory and angulation required. Alternative surgical pathways considered included the transpterygoid and contralateral precaruncular approaches. Despite cataract surgery 2 years prior, and after consultation with an ophthalmologist, no specific contraindications to the precaruncular approach were identified. Written informed consent was obtained from the patient to publish this case report and all accompanying images.
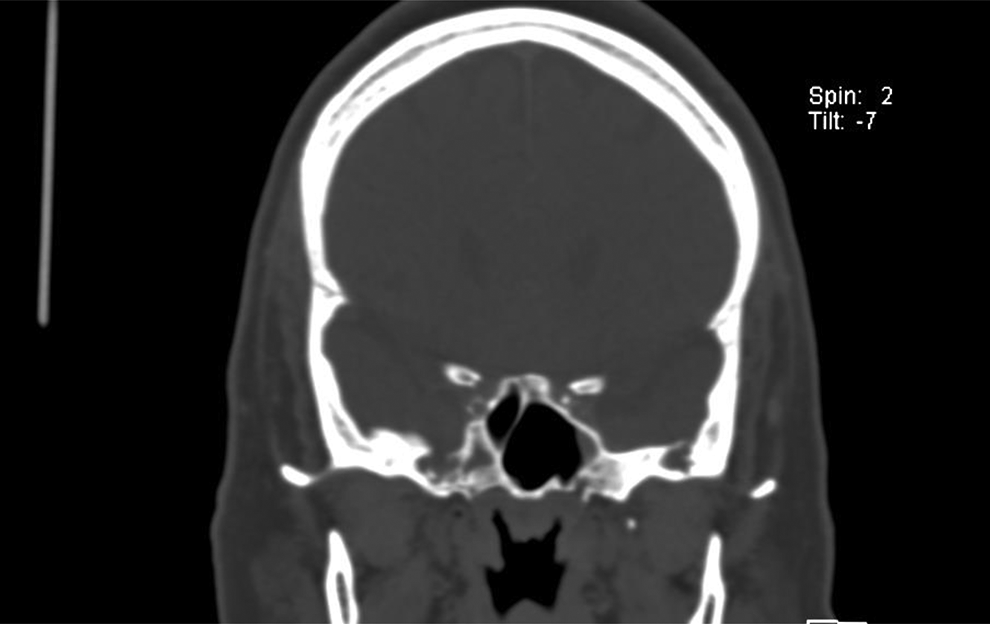
Coronal computed tomography (CT) image demonstrating skull base defect in the lateral aspect of the right sphenoid sinus.
Cadaver Dissection
Cadaver dissection was performed prior to surgery to simulate the surgical approach and trajectory from the caruncle of the left eye to the right lateral sphenoid sinus, and to aid in determining which preset navigation reference points should be applied to facilitate this approach.
Computer-Assisted Surgical Access and Pathway Planning
The Karl Storz NAV1 electromagnetic navigation system with SinusTracker computer modeling software (Karl Storz Endoscopy, Tuttlingen, Germany) was used to compare different surgical trajectories from left caruncle to the lateral aspect of the right sphenoid sinus and to plan the final surgical route. Ten anatomical reference points were manually programmed into the software system as surgical checkpoints along a preplanned surgical pathway. The left medial canthus was set as the entry point. A direct trajectory toward the lateral right sphenoid sinus was plotted, with the skull base defect located 83 mm from the entry point.
Surgical Technique
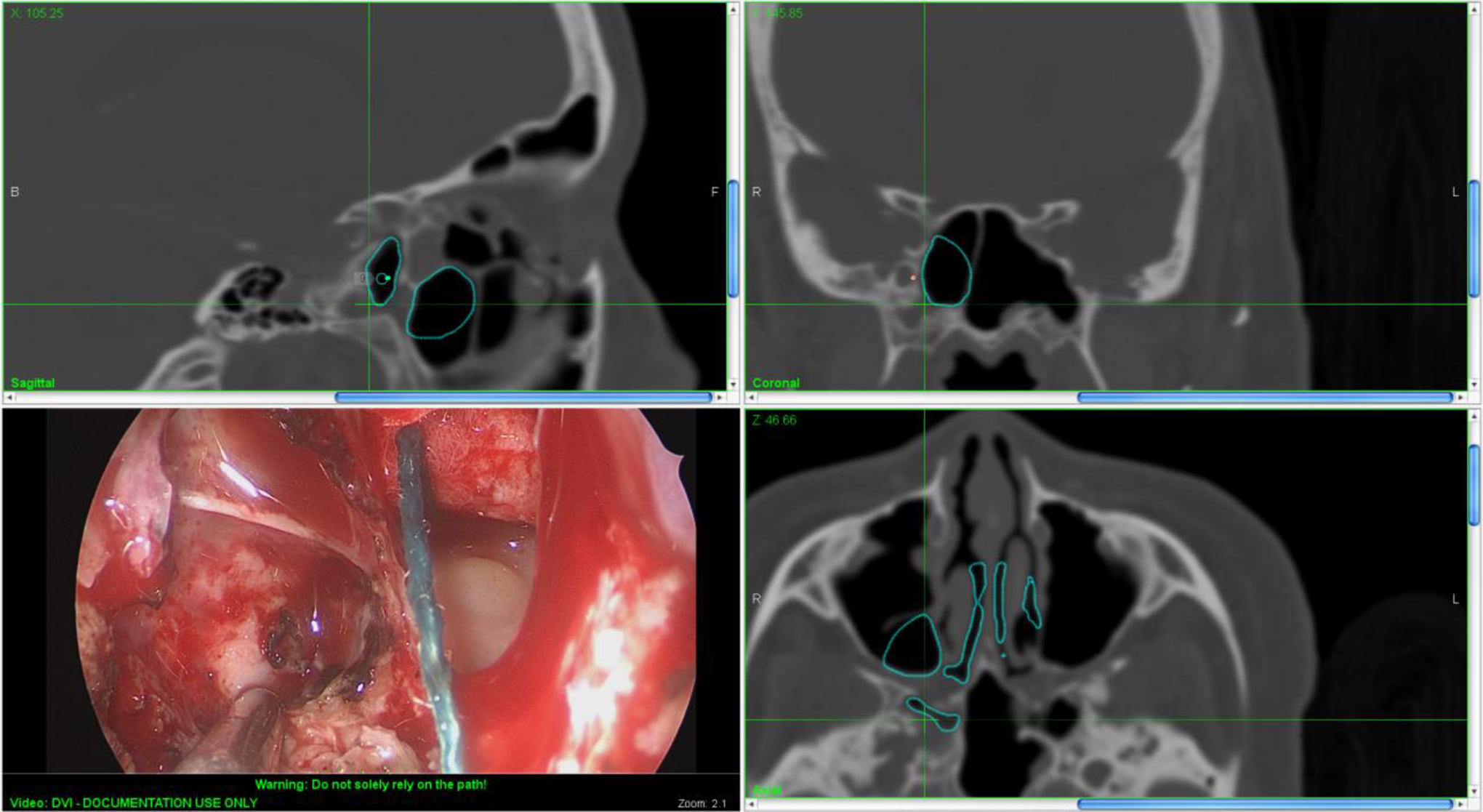
Surgery commenced with bilateral endoscopic anterior and posterior ethmoidectomies and sphenoidotomies as preoperative imaging had revealed incidental mucosal thickening and early polypoidal changes in the anterior and posterior ethmoid sinuses bilaterally. A mucoperichondrial septal flap was harvested from the right nasal septum and pedicled on the preserved sphenopalatine artery on the same side as the defect. Having previously undergone a repair of the defect 17 years prior, a small septal perforation was noted in the midpart of the nasal septum, involving the vomer and perpendicular plate of the ethmoid bone. In addition, a small amount of fat occupied the lateral aspect of the right sphenoid sinus, presumably a remnant of the previous defect repair. A left (contralateral) precaruncular incision was made between the caruncle of the left eye and the medial canthal skin (Figure 2).

Contralateral (left) precaruncular incision and surgical approach/pathway allows for multiportal access to lateral sphenoid defects.
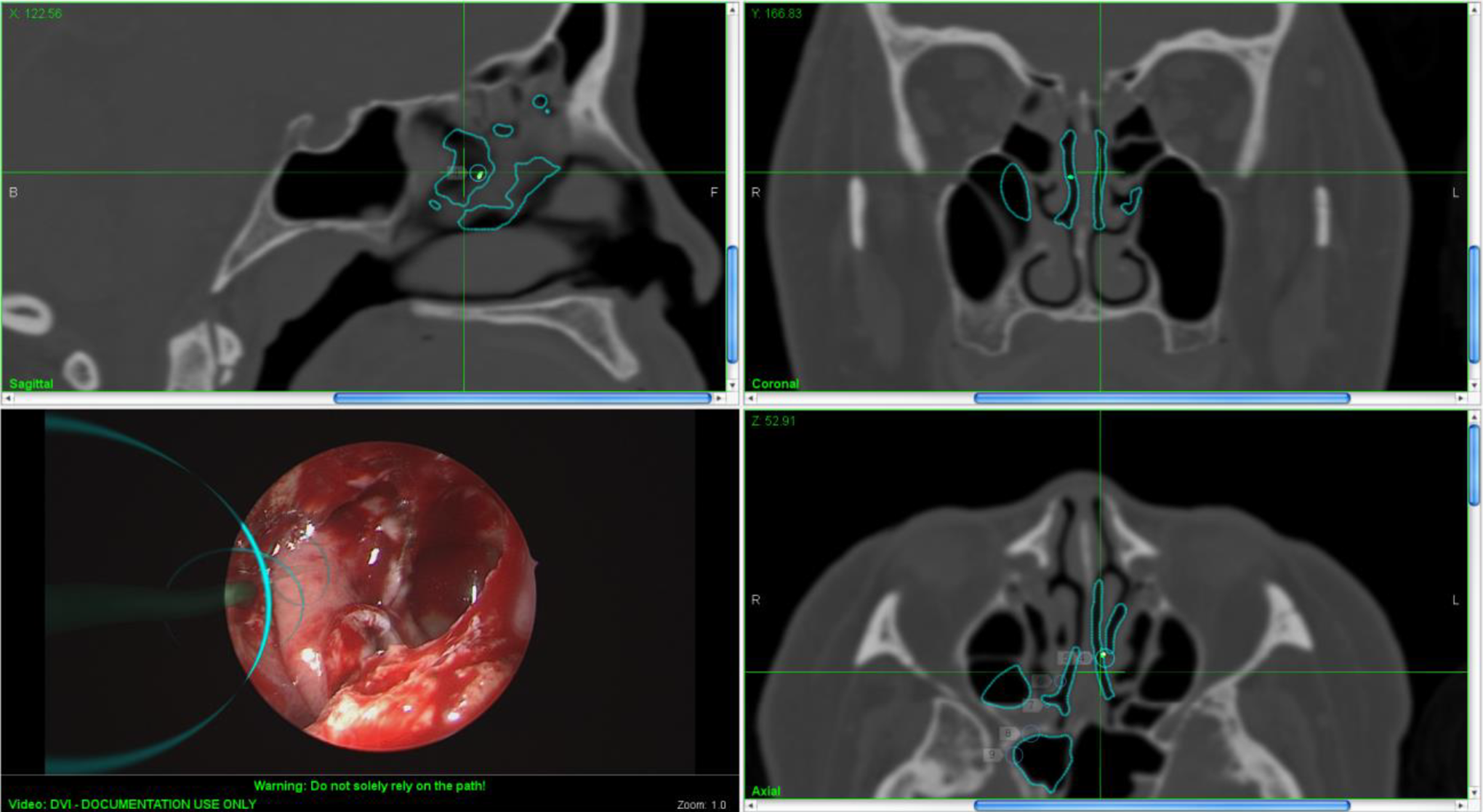
The anterior ethmoidal artery was identified along the frontoethmoidal suture line at the anterior ethmoidal foramen, and the lamina papyracea was breached 1 cm inferior to the artery to enter the posterior aspect of the left ethmoidal bulla. Multiportal access was gained through both nostrils and the left precaruncular pathway to advance and manipulate the rigid endoscope (Karl Storz Hopkins Telescope: 0-degree, 4 mm diameter, 18 cm length) and surgical instruments. The posterior basal lamella of the middle turbinate was breached to identify the left superior turbinate, and a posterior septectomy was performed to gain access to the right sphenoid sinus. Sphenoidal rostrum was drilled down between the 2 sphenoid ostia, and the face and floor of the sphenoid sinus were removed up to the vidian canal laterally. A rigid endoscope was passed through the left precaruncular incision and advanced through the left nasal cavity, through the posterior septectomy (transseptal) and into the right nasal cavity, together with a 3-mm Frazier suction tube (Karl Storz) held by an assistant. An endonasal drill (Medtronic, Dublin, Ireland) was inserted through either the left or right nostril, depending on the angle of approach required, with a second Frazier suction tube inserted through the contralateral nostril. Up to 6 surgical instruments could be used simultaneously, through 3 surgical portals, by adopting this multiportal approach. The defect in the lateral aspect of the right sphenoid sinus was easily visualized when advancing a 0-degree rigid endoscope through the left precaruncular portal toward the right sphenoid sinus. Exposure of the lateral right sphenoid sinus and surgical access to the defect were improved when compared to accessing the defect via the left and right nostrils alone. The advantage of the precaruncular approach is that it offers a more direct pathway to the defect (Figure 3).
The contralateral precaruncular approach allows for direct visualization of the lateral wall of the pneumatized sphenoid sinus and associated skull base defect.
Bipolar cautery was used to shrink a small meningocele found herniating through an underlying bony defect in the skull base. The full circumference of the bony defect was identified, and sphenoid sinus mucosa removed in preparation for the mucoperichondrial flap. A standard multilayer repair of the defect was performed. Abdominal fat was harvested and placed as an underlay intradural graft to seal the CSF leak. DuraGen Secure Dural Regeneration Matrix (Integra LifeSciences Corporation, Plainsboro Township, New Jersey) was placed over the defect as an extradural (between dura and bone) second layer. The ipsilateral mucoperichondrial septal flap was placed over the repair (Figure 4), and additional abdominal fat was packed tightly around the flap to keep it in place. An inflatable nasal tampon (Rapid Rhino; Smith & Nephew, Inc, Fort Worth, Texas) was passed through the right nasal cavity to support the septal flap and hold it in place. A lumbar drain was not deemed necessary. The precaruncular incision site required no suturing.
An ipsilateral (right) septal mucoperichondrial flap was harvested and used in a multilayer repair of the defect in the lateral sphenoid sinus. The preplanned surgical pathway (left lower image) was programmed with navigation software and superimposed onto the surgical field (turquoise circles). In this image, the defect/terminal point of the surgical pathway is covered by the septal flap.
Results
The patient was admitted to a general ward postoperatively and did not require observation in an intensive care unit. Pain was controlled with simple analgesia, and no postoperative antibiotic prophylaxis was administered (patient did receive routine intraoperative antibiotic prophylaxis). The patient was admitted for a total of 3 days, primarily to ensure adequate control of her hypertension and diabetes mellitus. She had no postoperative complications, no periorbital bruising or ecchymosis from the precaruncular approach, and no deterioration in preoperative visual acuity, as determined on serial ophthalmological evaluations (Figure 5). The patient was followed up for 21 months postoperatively, without recurrence of her CSF leak.
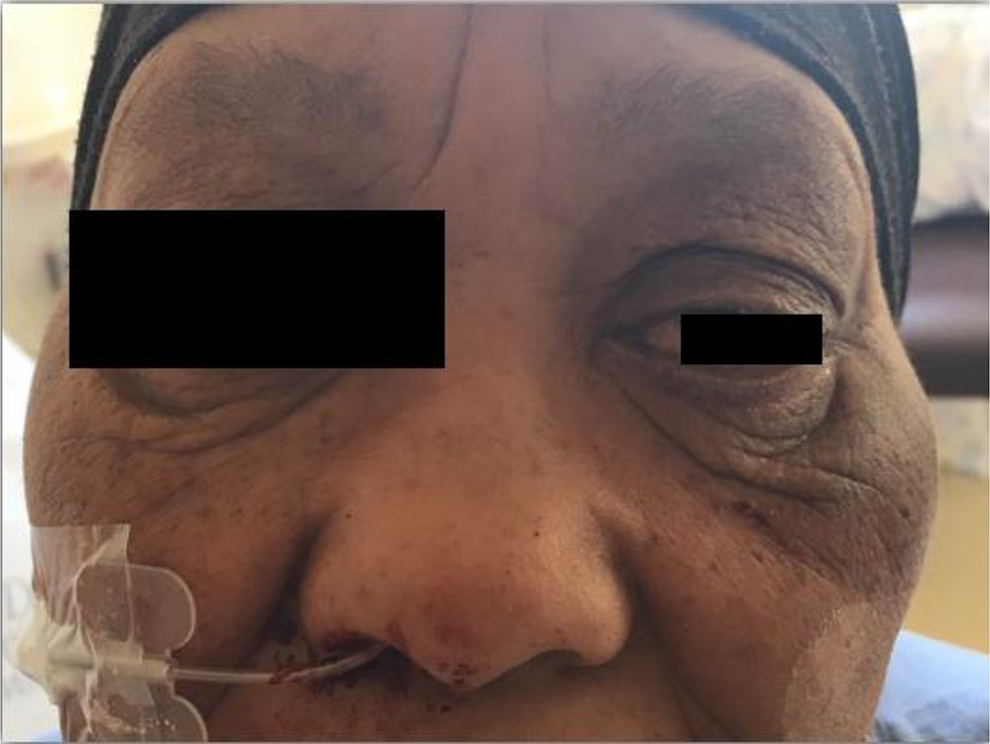
Photograph taken on first postoperative day: Rapid Rhino inserted into the right nasal cavity and inflated to support a right septal mucoperichondrial flap; no suturing of the left precaruncular incision required, with no periorbital bruising.
Discussion
Sphenoid sinus defects and CSF leaks occur more commonly secondary to trauma, tumors, or as a complication of surgery. Spontaneous meningoencephaloceles involving the sphenoid sinus were originally thought to arise from Sternberg canal, 6 a congenital bony defect in the lateral wall of the sphenoid sinus. However, current opinion suggests a multifactorial etiology and an interplay between anatomical (radiological findings of a pneumatized lateral recess of the sphenoid sinus, arachnoid pits, and an empty or partially empty sella turcica) and physiological factors (idiopathic intracranial hypertension). 7 -9 Furthermore, Settecase reviewed the radiological findings in 29 cases of spontaneous lateral sphenoid encephaloceles and categorized them into 2 types, depending on the presence or absence of a pneumatized lateral recess of the sphenoid sinus. 1 Type 1 defects communicate with the lateral pneumatized recess of the sphenoid sinus and present with CSF rhinorrhea and/or headaches, whereas type 2 defects herniate into the greater wing of sphenoid and are more likely to present with seizures, meningitis, headaches, or cranial neuropathy.
Surgical approaches to repair skull base defects have evolved from external (accessed via craniotomy, transfacially, or via sublabial approach) to endoscopic techniques. Traditional transseptal, direct transnasal, and transnasal transethmoidal endoscopic approaches to the sphenoid sinus do not provide satisfactory visualization of the lateral sphenoid recess for adequate repair of skull base defects in this challenging area. The endoscopic endonasal transpterygoid approaches to the lateral sphenoid recess are a recent development in the management of CSF leaks involving the lateral sphenoid recess and were born out of a need to minimize the morbidity associated with middle cranial fossa approaches. These expanded endonasal approaches to the skull base have been further refined, and some authors report a successful defect closure rate of up to 97%.
2
One of the limitations of the transpterygoid approach, however, is the need to resect a portion of the pterygoid plate, the extent of which is dependent on the location of the defect. Various classification systems have been used to describe the site of skull base defects and sphenoid encephaloceles, from pure anatomical descriptions to more practical systems based on surgical access. Kasemsiri et al devised a classification system based on the radiological distance of the vidian canal from the midline and the horizontal and vertical distances from vidian canal to foramen rotundum.
7
The most appropriate surgical corridor was planned preoperatively and involved classifying the surgical approach as 1 of 5 endoscopic endonasal transpterygoid approaches (A-E), based on the site and extent of pterygoid removal and dissection of adjacent structures. Lesions of the lateral sphenoid recess require removal of the anteromedial aspect of the pterygoid process (group B). The pterygoid process acts as a pillar anterior to the recess and obstructs exposure of the defect, necessitating removal. Developing a more direct trajectory toward the lateral recess of the sphenoid sinus would obviate or limit the need for dissection of the pterygopalatine fossa and resection of the pterygoid process. Advantages to using the contralateral precaruncular approach instead of the transpterygoid approach include: Maintaining the integrity of the pterygopalatine fossa with reduced risk of vidian nerve injury and postoperative palatal hypoesthesia. Preservation of both sphenopalatine arteries and the option of harvesting an ipsilateral septal mucoperichondrial flap for defect repair. A shorter flap can be raised, reducing septal cartilage and bone exposure with quicker healing and minimal crusting of the nasal cavity. A direct surgical trajectory from caruncle to surgical site allows for standard sinus surgery instruments to access the surgical site.
Transorbital neuroendoscopic approaches described by Moe et al have looked to build on the increasing tendency toward more minimally invasive approaches to the anterior skull base. 10,11 These transorbital portals complement established endonasal techniques and are advantageous in that they overcome the limitations of traditional endonasal approaches, that is, distance and angles of approach. A multiportal surgical approach allows enhanced visualization of the anatomical site and multisurgeon access, with multiple surgical instruments. In this case, a contralateral precaruncular pathway was utilized to allow a transseptal, sagittal approach to the contralateral (and involved) sphenoid sinus using a 0-degree, 4-mm rigid endoscope.
Conclusion
Through multidisciplinary collaboration, transorbital approaches to the skull base are evolving to play an important role in augmenting traditional endonasal surgical approaches to the skull base. When indicated, these techniques can improve surgical access and allow for easier instrumentation and manipulation of the surgical site. The contralateral precaruncular transorbital, transseptal, sagittal approach to the lateral recess of the sphenoid sinus provides a direct view into the lateral recess of the sphenoid sinus and obviates the need for extensive dissection in the region of the pterygoid process. This simple additional step adds significant value in terms of enhancing surgical access and minimizing surgical morbidity.
Footnotes
Authors’ Note
D.E.L. developed the study concept and design, drafted the manuscript, and performed the final review. H.W., P.D-.J., H.M., and P.L.S. contributed to patient clinical care, data collection, manuscript preparation, and editing. All authors read and approved the final manuscript. Written informed consent was obtained from the case patient for publication of this case report and all accompanying images. The University of Cape Town, Department of Surgery Research Committee/institutional review board was informed of our intention to submit this case report for publication. Need for ethics approval was waived.
Acknowledgments
The authors thank Karl Storz for providing the Karl Storz NAV1 SINUS TRACKER planning software used in conjunction with the Karl Storz NAV1 Electromagnetic navigation system in this case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.