
Abstract
The aim of this study was to examine how ibuprofen and paracetamol prevent pain after cold-steel extracapsular tonsillectomy in children. Also, we examined the relation between age, gender, nausea, postoperative bleeding, antibiotic use, type of diet, and postoperative pain intensity and the type of administered analgesic. A prospective study was conducted on 147 children (95 males and 52 females, aged 7-17 years) who underwent tonsillectomy in the Clinical-Hospital Center “Dragiša Mišović” from January 1 to June 30, 2016. The degree of pain was measured using a visual analog scale (VAS). We did not observe any significant differences in postoperative nausea, hospitalization rate postoperative bleeding, and antibiotic use between the paracetamol and ibuprofen groups. A test of within-patient effects showed that VAS scores changed significantly during the postoperative follow-up period (P = .00), but there were no significant differences between the groups (P = .778). After 12 hours, 29.3% of the patients on paracetamol and 21.8% on ibuprofen were transferred to a soft diet; after 24 hours, 84.8% of the paracetamol group and 85.5% of the ibuprofen group were on a soft diet (χ2 test, P < .05). There was a statistically significant correlation between VAS scores measured 4 hours after the surgery and the time of transference to the soft diet (Spearman ρ test, P < .001). The transfer to soft and normal diets was not significantly different between the 2 groups as assessed by the VAS scores (Pearson χ2 test, P = .565).There is still no consensus on the most effective postoperative pain-control regiment after tonsillectomy. This study showed that satisfactory pain management was achieved equally with both paracetamol and ibuprofen.
Introduction
Tonsillectomy is one of the most frequent surgical procedures in the world. Although the first intervention for tonsil removal was described by Celsus in the first-century AD, it was not until 1757 that Rheims described the first surgical technique of tonsillectomy. 1 Today, the most commonly used procedure is cold dissection extracapsular tonsillectomy. 2 Other techniques using bipolar electrocautery, laser, harmonic scalpel, and bipolar radiofrequency have been introduced in the attempt to lower the intensity of pain and postoperative bleeding. 3
The main postoperative concerns include pain, dehydration, and postoperative bleeding. Use of analgesics postoperatively is highly recommended. Also, postoperative analgesic consumption and nausea can be significantly reduced with perioperative and postoperative administration of high doses of steroids (dexamethasone or prednisolone), as recommended in the guidelines. 4,5
There are several reasons why the first 7 days after tonsillectomy could be problematic. Dehydration and poor food intake are closely associated with increased pain after tonsillectomies. 6 Noncompliant caregivers and not administrating analgesics to children postoperatively could be another significant contributing factor to poor control of postoperative pain. Also, it is under debate whether the administration of analgesics according to a fixed schedule is more efficient than dosing the medication as needed (PRN), since studies have indicated that children still complain of moderate pain intensity in both instances. 7,8 It was suggested that pain perception depends on the age of the child. Some studies reported that children younger than 12 years complained of less pain after tonsillectomy than teenagers and adults. 9
Standard analgesics used in postoperative child care in Serbia include nonsteroidal anti-inflammatory drugs (NSAIDs; ibuprofen or diclofenac) and paracetamol (acetaminophen). Opioids are not used for treating postoperative tonsillectomy pain.
The aim of this study was to examine how ibuprofen and paracetamol prevent pain after cold-steel extracapsular tonsillectomy. Also, we wanted to establish if age, gender, postoperative diet, occurrence of nausea, postoperative bleeding, repeated hospitalization, and antibiotic use were related to postoperative pain intensity and the type of administered analgesic.
Materials and Methods
This prospective study was conducted on 147 children (95 males and 52 females, aged 7-17 years) who underwent tonsillectomies in the Clinical-Hospital Center “Dragiša Mišović” from January 1 to June 30, 2016. The study and its duration were approved by the Institutional Ethics Board (decision number 1277/15). Indication for tonsillectomy was set according to a detailed history of the disease, documented episodes of recurrent tonsillitis, clinical examination, and laboratory tests. Children suffering from obstructive-sleep apnea weren’t included in the study. All patients underwent cold-steel extracapsular tonsillectomy under general endotracheal anesthesia. During surgery, anesthesia was delivered via inhalation of O2/nitrous oxide and sevoflurane (1.5-3 vol%), intravenous propofol (2.5-3 mg/kg), fentanyl (2-5 mcg/kg), rocuronium (0.6-0.8 mg/kg), or cis-atracurium (0.15 mg/kg). Antiemetic prophylaxis was conducted with dexamethasone (150 mg/kg).
Patients were followed until the first postoperative control, 7 days after the surgery. Patients were randomized by simple randomization into 2 groups, first group of 92 patients treated with paracetamol and second of 55 patients treated with ibuprofen for postoperative pain management. There are no differences between the groups according to age and gender. Analgesics were administered according to a fixed schedule given in the therapy chart: paracetamol: 10 to 15 mg/kg/dose every 6 hours (maximum 100 mg/kg/d or 4 g/d if >50 kg), or ibuprofen: 10 mg/kg/dose every 6 hours (maximum 40 mg/kg/d or 2.4 g/d). The degree of pain was measured using a visual analog scale (VAS; 0-100 m). The VAS was arranged as a 100-mm horizontal line with 2 end points (no pain and worst pain possible). The child was asked by a doctor to place a mark on the line at a point which they feel that represents the intensity of their pain. The VAS is scored by measuring from no pain to the point selected on the scale. Information and explanation on how to use VAS scale was provided to a child upon hospital admittance. Information about the type of diet (clear fluid, soft diet, or normal diet) was recorded, based on the information provided by the parents or guardians. In cases of postoperative fever (above 38°C) and high white cell blood counts (above 12 × 109/L), ceftriaxone was given for up to 3 days (in children <50 kg, 50-80 mg/kg once a day up to 2 g a day; in children >50 kg, 2 g once a day), with a switch to therapy with oral antibiotics, cefixime or cefpodoxime, for up to 7 days. Data for postoperative nausea, bleeding, repeated hospitalization, and antibiotic use were recorded during the follow-up period. Measurements were made 4 hours, 12 hours, 24 hours, and 7 days postoperatively.
SPSS v20 (SPSS Inc, Chicago, Illinois) was used for statistical analysis. Sample size was calculated based on a continuous response variable, that is, mean VAS pain scale from ibuprofen and paracetamol groups with 1:2 allocation ratio. For expected moderate size effect (Cohen d = 0.45), calculated sample size was 47 and 93 patients per ibuprofen and paracetamol group, respectively, to be able to reject the null hypothesis that the population means of the groups are equal with probability (power) 0.8. The type I error probability associated with testing this null hypothesis is .05.The total number of patients recruited for the study was then estimated to be 140. Descriptive statistics were calculated for demographic characteristics, risk factors, and other followed parameters and are presented as means (standard deviations [SD]), medians with interquartile ranges, or absolute and relative frequencies. t test, χ2 test, and analysis of variance for repeated measures were used to establish statistical differences between parameters. Statistical significance was considered at P <.05.
Results
The study included 147 patients, of which 95 (64.6%) were males and 52 (35.4%) were females. Patients were randomized into 2 groups: first, 92 patients treated with paracetamol and second, 55 patients treated with ibuprofen for postoperative pain management. Before surgery, most of the patients were without any preexisting condition or disease and were not using medication (94%). Nine patients (6%) had asthma and were on fenoterol–ipratropium bromide. All patients were without any respiratory infections or antibiotic therapy at least 3 weeks before the surgery.
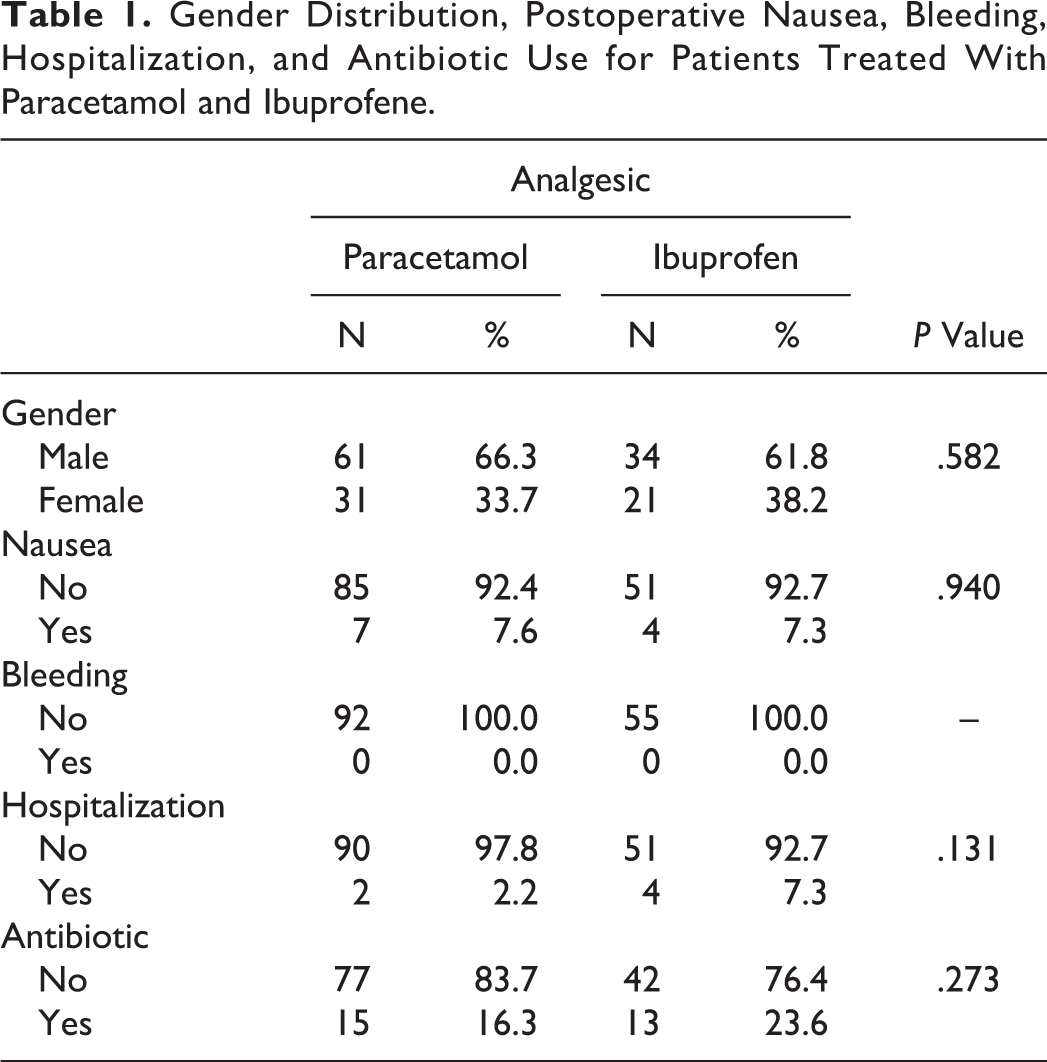
Patients were of the age 7 to 17 years, with a mean age of 9.54 years. Patients who were treated with paracetamol postoperatively had a mean age of 9.75 (SD 2.744), and patients treated with ibuprofen had a mean age of 9.2 (SD 2.656). There were no significant differences in age between the 2 groups (t test, P = .236). Data about gender distribution, postoperative nausea, bleeding, hospitalization, and antibiotic use are presented in Table 1. The gender distribution was equal between groups. There were no significant differences in postoperative nausea, hospitalization rate, and antibiotic use between the groups treated with paracetamol and ibuprofen. No postoperative bleeding was recorded during the 7-day follow-up period.
Gender Distribution, Postoperative Nausea, Bleeding, Hospitalization, and Antibiotic Use for Patients Treated With Paracetamol and Ibuprofene.
The VAS scores measured postoperatively are shown in Table 2 and Figure 1. The test of within-patient effects showed that VAS scores changed significantly during the postoperative follow-up period (P = .00), but there were no significant differences between groups (P = .778).
Postoperative VAS Scores for Patients Treated With Paracetamol and Ibuprofen.
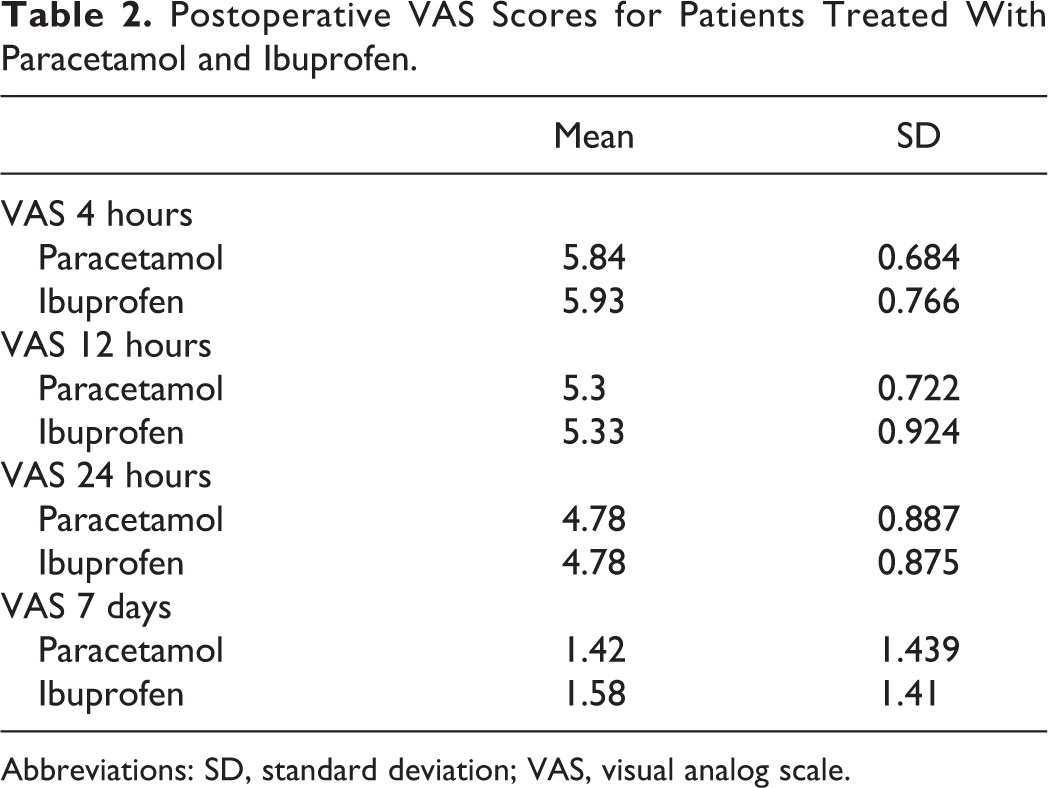
Abbreviations: SD, standard deviation; VAS, visual analog scale.
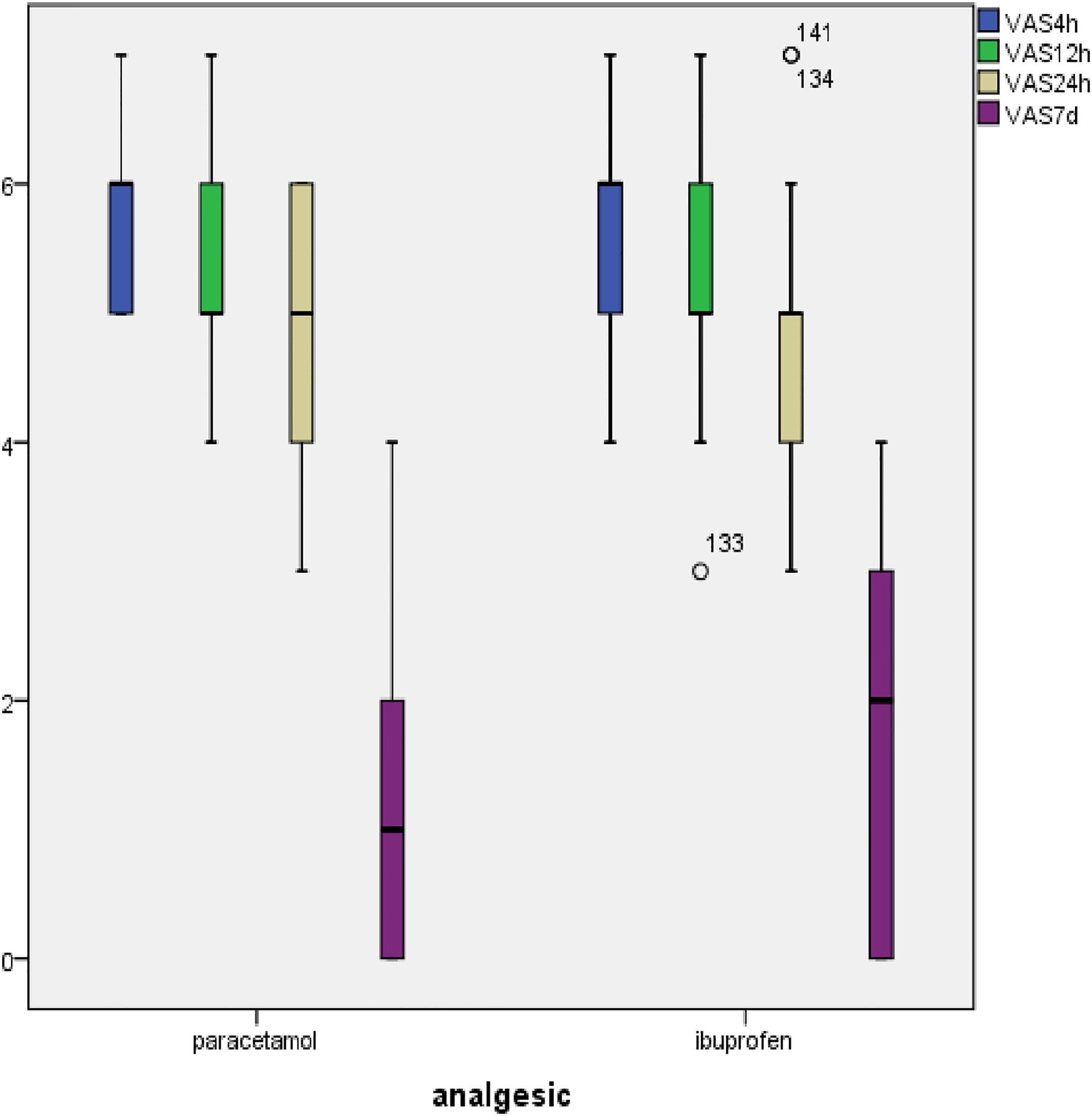
Postoperative VAS scores for patients treated with paracetamol.
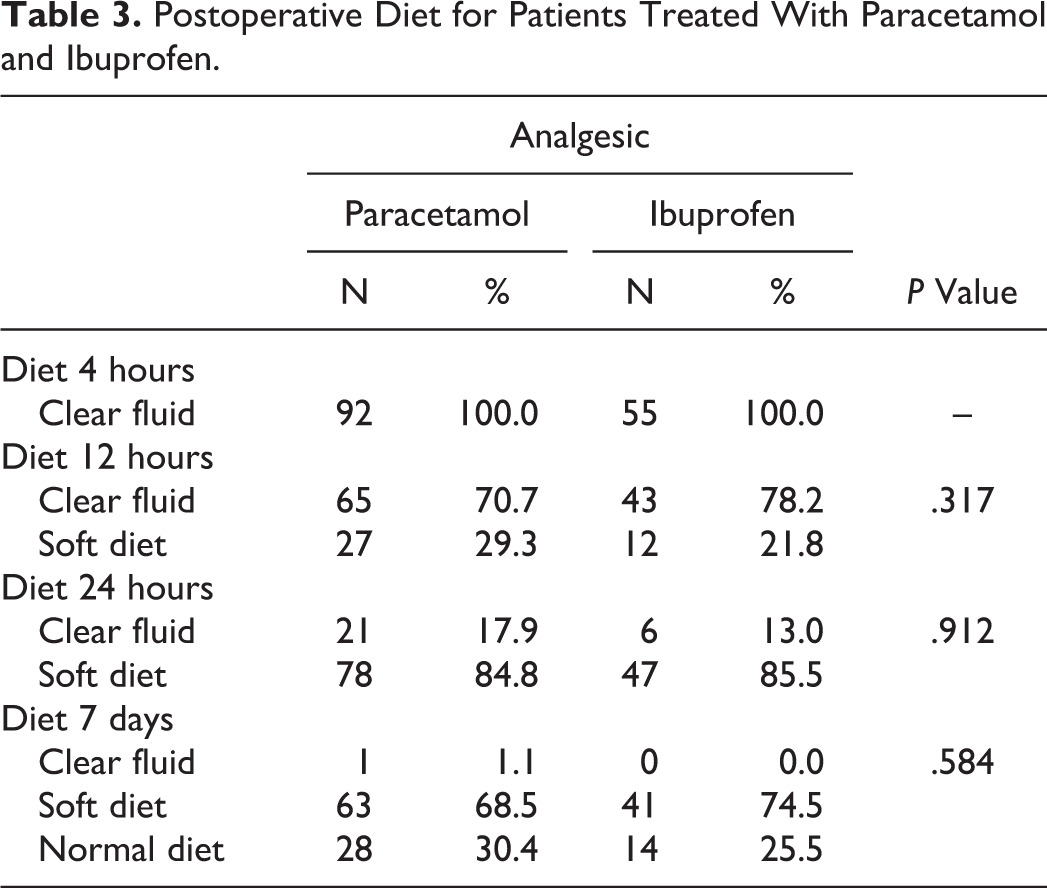
All patients had a clear fluid meal 4 hours after surgery (Table 3). After 12 hours, 29.3% of the patients who received paracetamol and 21.8% of the patients who received ibuprofen were transferred to a soft diet (χ2 test, P = .317). After 24 hours, 84.8% of the patients in the paracetamol group and 85.5% in the ibuprofen group were on soft diet (χ2 test, P = .912). Seven days after the surgery, 68.5% of the patients in the paracetamol group were on the soft diet and 30.4% were on the normal diet. In the ibuprofen group, 74.5% were on the soft diet and 25.5% were on the normal diet (χ2 test, P = .584). There was no statistical difference between the groups transferred to either the soft or normal diets (χ2, P = .565).
Postoperative Diet for Patients Treated With Paracetamol and Ibuprofen.
We examined variations of the VAS score depending on gender, age, and type of diet during the postoperative follow-up period. The VAS scores did not significantly vary depending on age (tests of between-patient effects, P = .675) and gender (tests of between-patient effects, P = .899), and they were not statistically significant. Transfer to soft and normal diet was not significantly different between the 2 groups depending on VAS scores (χ2, P = .565). However, there was statistical significant correlation between VAS scores measured 4 hours after the surgery and the time of transfer to the soft diet; if the VAS scores were lower, the transfer to soft diet was quicker (Spearman ρ test, P < .001).
Discussion
Tonsillectomy is one of the most frequently performed surgeries in the pediatric population. Considering that it is performed as a 1-day surgery, postoperative pain management is one of the main concerns. It can affect postoperative liquid and food intake, speed of recovery, and everyday activities in children.
Reliability and validity of VAS, as a self-assessment measure, have been the widely explored and well established. 10 Considering cognitive ability and age, it was confirmed that VAS can be reliably and accurately used in children aged 7 years and older. 11 -13 The VAS scores have been shown to be sensitive to changes in pain levels during postoperative periods 14 and following analgesic medications. 15 The minimum clinically significant difference in the VAS pain score for children 8 to 15 years old was determined to be 10 mm (95% confidence interval, 7-12 mm). 16 Reliability of the VAS for acute pain measurement was assessed at 90%, with the repeatability coefficient in children aged 8 to 17 years that varies from 6 to 12 mm on a 100-mm VAS. 17 -19 Children’s VAS scores were shown to correlate significantly with parent ratings of children’s pain and with medical personnel, as well as the scores of other types of pain. 13
Our study used VAS to evaluate the effects of paracetamol and ibuprofen as 2 of the most commonly used analgesics in pain management after cold dissection extracapsular tonsillectomy. In Serbia, opioids are not in use for postoperative tonsillectomy pain management.
The analgesic effects of paracetamol are mainly through central mechanisms, by inhibition of central COX systems, stimulation of descending serotonergic pathways, and indirect activation of cannabinoid receptors. 20 Nonsteroidal anti-inflammatory drugs also act by inhibiting COX, but there are differences. Paracetamol has a weak anti-inflammatory effect, few or no gastrointestinal side effects, and causes only a small dose-dependent alteration in platelet function. 21
Ibuprofen as NSAID has become a significant choice for postoperative analgesia. Although it provides adequate pain management, 22 its routine use remains controversial as NSAIDs also potentially cause platelet dysfunction that can lead to increased risk of postoperative bleeding. 23 Studies showed that a single dose of ibuprofen between 300 and 900 mg inhibits platelet aggregation 2 hours after administration. Low doses of ibuprofen (200 mg 3 times daily) didn’t prolong the bleeding time, but higher doses (up to 600 mg 3 times daily) influenced on bleeding time prolongation after administration. 24 In this study, postoperative bleeding was not noted in either patients who used acetaminophen or in those who used ibuprofen for a follow-up period of 7 days. Due to specific pharmacokinetic of ibuprofen, any adverse effects of ibuprofen would be expected in that time frame. Secondary bleeding occurs more than 24 hours after the surgery, often between 5 and 10 days, and is usually caused by fibrin layer detachment during healing. 7 According to recent literature, evidence confirming an increased risk of postoperative tonsillectomy bleeding associated with NSAID therapy is lacking. 25 -28
The regime of analgesic administration is still discussed in the literature. Medication according to a fixed schedule is widely used, as it was in our study; however, this could still be insufficient for pain management after tonsillectomy. According to a few clinical trials, during pain management with different analgesics as one medication (acetaminophen) or a fixed combination (acetaminophen and codeine or rofecoxib and hydrocodone), a fixed schedule is more effective than dosing medication PRN after tonsillectomy. 7,29 A fixed administration schedule is especially required to obtain paracetamol’s optimal analgesic effect. Its central activity depends on transport across the blood–brain barrier through passive diffusion, which is highly dependent on sufficiently high plasma concentrations of paracetamol. After oral administration, paracetamol uptake occurs mainly in the small intestine, so that plasma concentrations might be affected postoperatively because of impaired gastric emptying. It is known that surgical intervention itself can decrease gastrointestinal motility and delay gastric emptying; however, opioid analgesics, the fasting state, and supine positioning can all contribute to it. 30,31 As a result of paracetamol absorption, after oral dosing, its concentrations may not be as per published pharmacokinetic data, so that its fixed administration can provide adequate serum levels. Although some studies deemed paracetamol to be a safe drug but not potent enough to provide efficient analgesia after tonsillectomy, our results showed that paracetamol and ibuprofen have a very similar analgesic effect when administered according to a fixed schedule. 7,8
In the study, paracetamol was used for pain management was used in 92 patients, and ibuprofen was used in 55 patients. There are number of different available analgesics from NSAID group, and there is no significant difference in their efficacy. There are, however, significant individual variations in the patients’ response to those analgesics. 32 For developing an appropriate postoperative pain management plan, an assessment of past and current history of pain, including the use of, response to, and preferences for certain analgesics, is needed. 33 The choice of the right analgesic in this study was made by both physician and patient (or in many of cases in this study, parent or a guardian) on the balance between efficiency and risk and previously used analgesics that were efficient in pain management.
The children included in our study complained of moderate pain during the first 12 hours after surgery, with VAS scores below 6 in both groups, and below 5, 24 hours after the surgery. Seven days after the surgery, the children complained of mild pain, with VAS scores below 2 in both groups. No significant differences were noted between the paracetamol and ibuprofen groups, although the scores for the paracetamol group were slightly lower at 4 hours, 12 hours, and 7 days after surgery. We can say that postoperative tonsillectomy pain has its own natural course. Many studies have indicated that children, irrespective of the dosing regimen and analgesic choice, complain of moderate-to-severe pain, with VAS scores above 5 in the first 7 days after tonsillectomy. After 7 days, the VAS scores decreased significantly. 31,34,35 We could consider ibuprofen and paracetamol successful in achieving analgesia with VAS scores below 6 after tonsillectomy.
In other studies, no significant association between children’s age and sex and the intensity of postoperative pain was observed, which was also observed in our study. 36,37 Some authors used other measures, such as returning to a normal diet, refusing fluids, nausea, antibiotic use, and readmission to indirectly quantify postoperative pain. 38,39 In our study, children with nausea who were readmitted to the hospital and treated with antibiotics did not report significantly greater pain intensity. Pain intensity significantly influenced the transfer of patients from a liquid to a soft diet, but not from a soft to a normal diet. A possible explanation lies in the pathophysiology of the healing process after tonsillectomy. 40 Edema and pain are greatest immediately after surgery, probably as a result of thermal effects and the expression of inflammatory mediators that stimulate pharyngeal nociceptors. The VAS measurements in this study were performed in the first 4, 12, and 24 hours postoperatively to obtain result indicating moderate pain levels. Using paracetamol or ibuprofen was crucial for pain management and for early postoperative course in these children. Pain gradually decreases over time, with an increase in pain measured on postoperative days 3 to 5, which corresponds to maximal wound inflammation. Due to our study design, patients weren’t available for measures until first postoperative control on postoperative day 7. A fibrin layer starts forming after the surgery, followed by inflammation of the surrounding tissue. From postoperative day 7, fibrin starts to shed and reepithelization is usually finished by the end of 2 weeks. After the first week, pain significantly decreases. In our study, 30.4% of the children in the paracetamol group and 25.5% of those in the ibuprofen group returned to a normal diet 7 days after surgery.
The study has few weaknesses. First, although analgesics were administrated according to a fixed schedule, there are no measures of compliance with the administration of analgesics in our patients. According to the literature, compliance of the parents or guardians with the administration of analgesics following tonsillectomy is problematic. 7 Significant number of children receive little or no medication, despite reporting moderate to severe pain. Possible direction of future research of analgesics effectiveness should involve medication administration logs and a measure of total administered medication.
Second, the results indicate that there aren’t significant differences in the pain management between these 2 medications. However, it should be emphasized that this isn’t same as equivalence. Two medications used for pain management in the study have different chemical structure, mechanism of action, and dosing regime, but their effect on pain management after tonsillectomy was without significant differences. Although this study showed similar effects of paracetamol and ibuprofen in pain management, a possible future direction in post-tonsillectomy analgesia could be a multimodal approach. There is evidence that simultaneous administration of paracetamol and ibuprofen in the pediatric population is superior to monotherapy. 41,42 According to Swedish guidelines, COX inhibitors combined with paracetamol given regularly are often sufficient for 5 to 8 days after tonsillectomy. 43
In conclusion, there is still no consensus as to what is the most effective postoperative pain-control regiment after tonsillectomy. Also, the methods of pain measurement in studies are very heterogeneous, especially for the pediatric population. Postoperative analgesia needs to be effective and safe for children. This study showed that satisfactory pain management was achieved effectively with either paracetamol or ibuprofen without unwanted complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (Grant No. 175023).