
Abstract

An otherwise healthy adolescent girl presented with a mandibular swelling of 2 weeks’ duration. She reported paresthesia in the lower lip but denied pain or trismus. On examination, there was a firm mass with erythematous mucosa in the left oral vestibule. There was no lymphadenopathy in the neck.
Computed tomography of the face showed a 3.2 × 4.3 × 2.8-cm osteoblastic destructive mass breaching the cortical boundary of the mandible and extending into the surrounding soft tissues (Figure 1). Magnetic resonance imaging showed peripheral enhancement of the extraosseous soft-tissue extension (Figures 2 and 3). Technetium bone scan showed intense focal uptake in the left mandibular body (Figure 4). Biopsy proved an intermediate-grade osteosarcoma.

Axial nonenhanced bone algorithm CT image shows an osteoblastic destructive mandibular mass. CT indicates computed tomography.
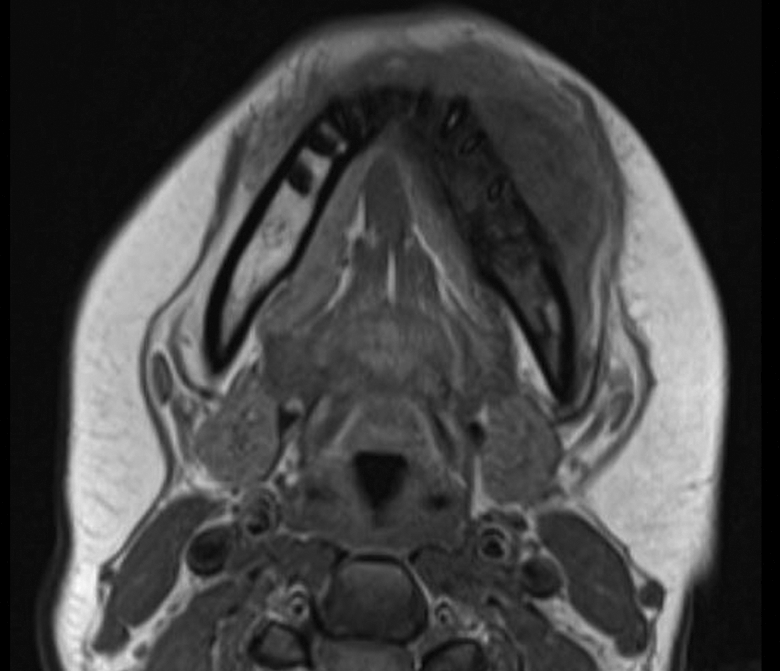
Axial T1-weighted MR image shows the extent of lesion outside of the jaw. MR indicates magnetic resonance.
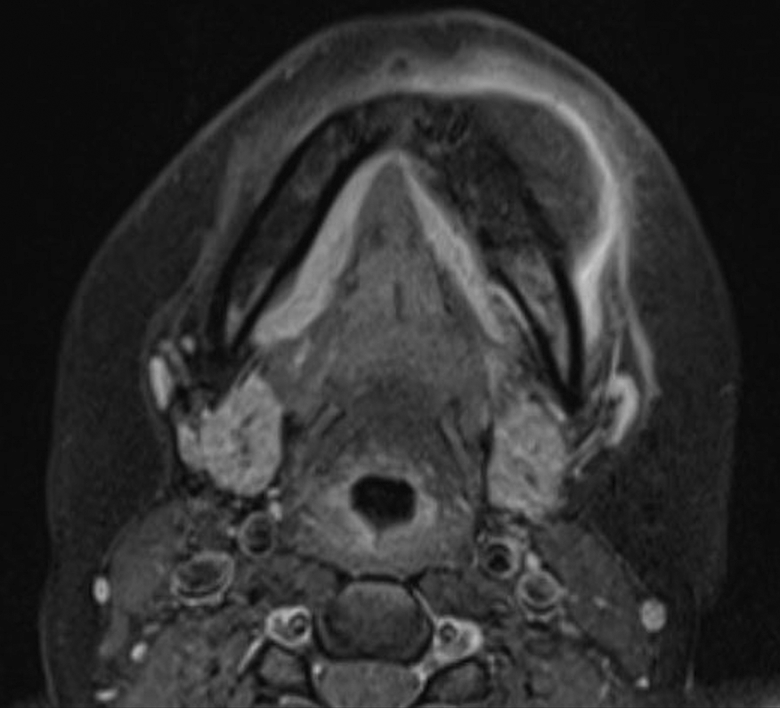
Axial postcontrast fat-suppressed T1-weighted MR image shows peripheral enhancement of the extraosseous soft-tissue extension. MR indicates magnetic resonance.
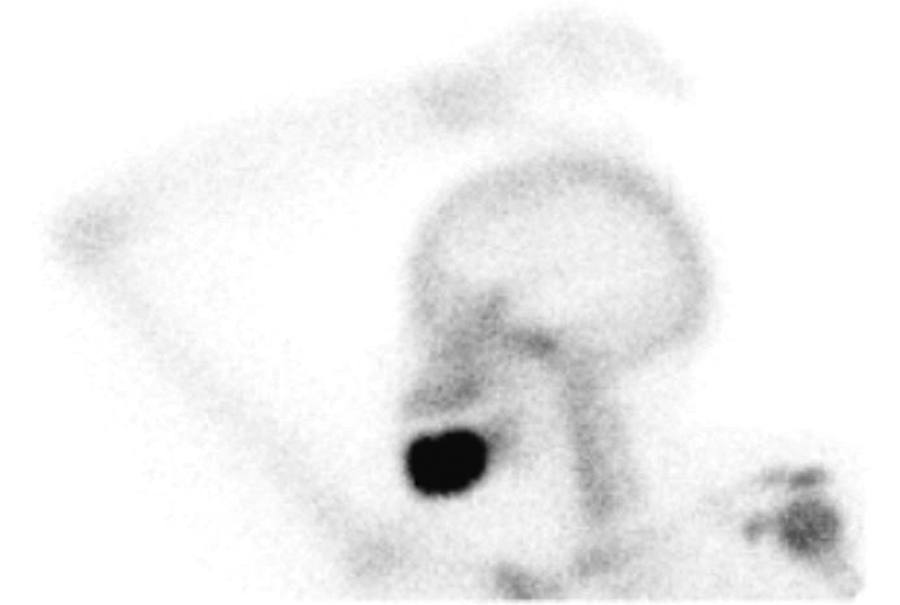
Technetium bone scan shows intense tracer uptake.
Osteosarcoma, or osteogenic sarcoma, is a malignant bone tumor in which the neoplastic cells produce osteoid or immature bone. Jaw osteosarcoma is uncommon, representing approximately 7% of all osteosarcomas. 1 Compared to the clinical presentation of long bone osteosarcoma, jaw osteosarcoma occurs in an older patient population (30-50 years) and tends to behave less aggressively. 1 The mandible is more commonly involved than the maxilla, and males and females are affected with about equal frequency. Osteosarcoma is known to occur in association with Paget disease of bone, retinoblastoma, and fibrous dysplasia after therapeutic irradiation. According to the relative amounts of osteoid, cartilage, or collagen fibers produced by the tumor, osteosarcomas are classified as osteoblastic, chondroblastic, or fibroblastic.
Swelling is the most common presenting symptom in patients with jaw osteosarcoma. 2 Other symptoms may include pain, paresthesia, loose teeth, and trismus.
The imaging appearance varies according to the extent of mineralization. Thus, the internal pattern may be osteolytic, mixed osteolytic-sclerotic, or entirely sclerotic. There typically is a “sunburst” appearance caused by spiculated bone formation on the surface of the lesion. Osteosarcoma of the jaw may first appear as a symmetrical widening of the periodontal ligament space around a tooth or a group of adjacent teeth. 3 In some cases, when the teeth are involved, there is “spiking” resorption of the roots of teeth involved by the tumor. 4 Magnetic resonance imaging usually shows a low and intermediate signal intensity on T1-weighted and T2-weighted images, respectively. There usually is nonhomogenous enhancement with contrast.
Osteomyelitis, chondrosarcoma, and Ewing sarcoma share some of the radiographic features of osteosarcoma. If spiculated periosteal bone reaction is present, prostate and breast metastases should be considered.
Surgical resection is the primary treatment modality for jaw osteosarcoma. Radiation and chemotherapy may be used as adjunctive therapies. Patients are prone to develop either a recurrence or distant metastases, particularly to the lungs. The 5-year disease-specific survival rate is 62%. 5
Footnotes
Authors’ Note
This article was not previously presented or published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.